
Abstract
Background
*N.P. and M.P. contributed equally to this study.
Objective
The objective of this article is to assess the prevalence and risk factors for esophagitis in Spain.
Methods
A prospective, observational, cross-sectional, multicenter study (PRESS study) was conducted among 31 gastrointestinal endoscopy units throughout Spain. A total of 1361 patients undergoing upper gastrointestinal endoscopy were enrolled. Sociodemographic, clinical and treatment data were recorded.
Results
A total of 95% of patients were Caucasian and 52% were male (mean age: 53 ± 17 years). The most frequent symptoms prompting endoscopy were heartburn (40%), regurgitation (26%) and dysphagia (15%). Fifty-four percent of patients undergoing endoscopy were receiving proton pump inhibitor (PPI) treatment. Esophagitis (mainly mild-moderate) was present in 154 (12.4%) patients. The severe form was recorded in only 11 (0.8%) patients. Multivariate analysis results indicated that the likelihood of esophagitis was higher in men (OR = 1.91, 95% CI = 1.31–2.78), in patients with high GERD-Q scores (OR = 1.256, 95% CI = 1.176–1.343), weight increase (OR = 1.014, 95% CI = 1.003–1.025) and high alcohol consumption (OR = 2.49, 95% CI = 1.16–5.36).
Conclusion
Severe esophagitis is a rare finding in the Spanish population. Male gender, high GERD-Q score, weight increase and high alcohol consumption are main risk factors for its appearance.
Keywords
Introduction
Gastroesophageal reflux disease (GERD) is a common condition that affects about 15%–30% of the population.1–5 GERD comprises a wide variety of clinical manifestations, ranging from reflux symptoms without visible lesions on conventional endoscopy (non-erosive reflux disease, NERD) to grossly visible esophagitis with varying extent of mucosal breaks.6,7
Endoscopy is generally accepted as an important clinical tool for the identification of esophageal injury syndromes. 8 For patients with esophageal symptoms unresponsive to adequate empiric therapy, the aim of the endoscopy is to make a positive diagnosis of esophagitis and to assess or to rule out other esophageal conditions. 8
Data on the current endoscopic prevalence of esophagitis and severe esophagitis in southern Europe are scarce. Furthermore, many factors that might influence the development of these diseases – for example, the type of predominant diet, tobacco or alcohol consumption, or proton pump inhibitor (PPI) use – have been steadily changing in recent years. A previous retrospective study by our group found the prevalence of esophagitis to be low, appearing in only 8.7% of 93,699 endoscopies reviewed. 9
In addition, at present, it is not fully understood which additional risk factors contribute to the development of reflux esophagitis or what influence these factors might have on disease severity. Possible risk factors reported include overweight, male gender, history of GERD, smoking habit, absence of Helicobacter pylori or presence of hiatal hernia.1–3,10–13 As far as severe esophagitis is concerned, the clinical data suggest a relationship with severity of symptoms, presence of heartburn for more than five years, obesity, presence of hiatal hernia, male gender and Caucasian ethnicity.14,15
Finally, the role of drugs in the pathogenesis of severe esophagitis is especially controversial and has been only partially evaluated. While the use of PPIs is considered to be a protective factor,11,16 the role of other drugs such as anticholinergics, 17 nitrates11,18 and tricyclic antidepressants, calcium antagonists or sulcralfate 11 is more debatable. In particular, the results of studies of the effect of nonsteroidal anti-inflammatory drugs (NSAIDs) have been contradictory.15,18–20
In this context, we assessed the prevalence and risk factors of esophagitis, and specifically the role of NSAIDs, in an observational, cross-sectional, nationwide, multicenter study (Prevalence and Risk factors for Esophagitis in Spain (PRESS)).
Methods
Study design
From January to December 2009, an observational, cross-sectional, nationwide, multicenter study (PRESS study) was conducted in the context of the routine clinical practice of gastroenterologists from gastrointestinal endoscopy units at 31 Spanish National Health Service and private centers (Figure 1). Hospitalized patients or outpatients from primary care or specialist settings who underwent upper gastrointestinal endoscopy were enrolled.
Geographical distribution of participating centers.
Once a month, on a randomly selected working day, all patients undergoing an upper gastrointestinal endoscopy were evaluated for inclusion in the study. Patients who agreed to participate underwent a clinical interview and a clinical exploration, and socio-demographic and clinical data were recorded. Socio-demographic characteristics included sex, age, ethnicity, place of birth, socioeconomic status, weight, height, abdominal perimeter, alcohol consumption and tobacco use.
Clinical characteristics included clinical history of GERD (frequency and severity of typical symptoms of heartburn, regurgitation and dysphagia, and time from onset), previous diagnosis of reflux disease, esophagitis and Barrett's esophagus, comorbidities, current treatments and indication for endoscopy. Moreover, before the procedure, the patient was asked to complete two self-administered questionnaires: the general questionnaire named “Gastrointestinal Symptom Rating Scale” (GSRS), modified for patients with upper gastrointestinal disorders 21 and GERD-Q, the specific questionnaire for assessing GERD. 22
The GSRS includes 15 items for the description of gastrointestinal symptoms. 21 GERD-Q includes six items for scoring the number of days with symptoms and the use of over-the-counter (OTC) medications during the previous seven days.22,23 Six symptoms, including heartburn, regurgitation, and upper abdominal pain, were evaluated for frequency on a four-point Likert scale. A cut-off score of 8 points has the highest specificity and sensitivity when testing for GERD. 24
Information on treatment was collected by structured interview before the procedure. The medication taken during the last month was recorded, with a specific register of NSAIDs, acetyl salicylic acid (AAS) and other antiplatelet drugs, PPIs and histamine H2-receptor antagonists. In all cases, the name of the drug and medicinal product, posology and period of treatment were recorded. If necessary, data were confirmed after the procedure by telephone.
During the procedure, endoscopic findings were recorded. Esophagitis was diagnosed and classified according to the Los Angeles classification (LAC). 25 The presence and size (cm) of hiatal hernia was recorded and other lesions were briefly described. H. pylori determination was not mandatory. The decision of whether H. pylori study was necessary and the choice of the method for investigating the infection were left to the criteria of the endoscopist.
Statistical analysis
In the statistical analysis, frequency tables, percentages and 95% confidence intervals (95% CIs) were obtained for categorical variables, while measures of central tendency and dispersion were calculated for continuous variables (mean, standard deviation (SD), standard error (SE), minimum and maximum and 95% CIs, median and quartiles Q1 and Q3). For analysis, weight and height were stratified according to sex. Abdominal perimeter was considered to be increased when it was above 101 cm in males and 88 cm in females. 26 Alcohol intake was considered significant when it was more than 20 drinks per week. Smoking was considered significant when patients consumed 10 or more cigarettes per day and major when they consumed 20 or more cigarettes per day.
The chi-square test was used to compare qualitative variables between groups, and non-parametric tests and analysis of variance (ANOVA) were used to compare quantitative variables.
Univariate and multivariate logistic regressions (stepwise method) were performed to determine which factors were associated with esophagitis and, particularly, with severe esophagitis. Finally, the Hosmer-Lemeshow test was performed to establish the goodness of fit of the models. In all cases, statistical significance was defined as a p value less than 0.05, and the statistical analysis was performed using SPSS v.21.0 (IBM Corp. Chicago, IL, USA).
Sample size calculation
A sample size of 1300 patients was calculated a priori as sufficient for detecting a minimum increase in odds ratio (OR) of 1.5 related to NSAID use, with an alpha level of 0.05 and a beta level of 0.20.
Ethics statement
The study was reviewed and approved by the ethics committees of both the Hospital Universitario La Fe (Valencia, Spain) and the Corporació Universitària Sanitària Parc Taulí (Sabadell, Spain). Written informed consent was obtained from all participants. Data were coded in order to avoid patient identification and managed in accordance with the Spanish “Ley de Protección de Datos de Carácter Personal” (https://www.boe.es/buscar/pdf/1999/BOE-A-1999-23750-consolidado.pdf).
Results
Sociodemographic and clinical characteristics of patients
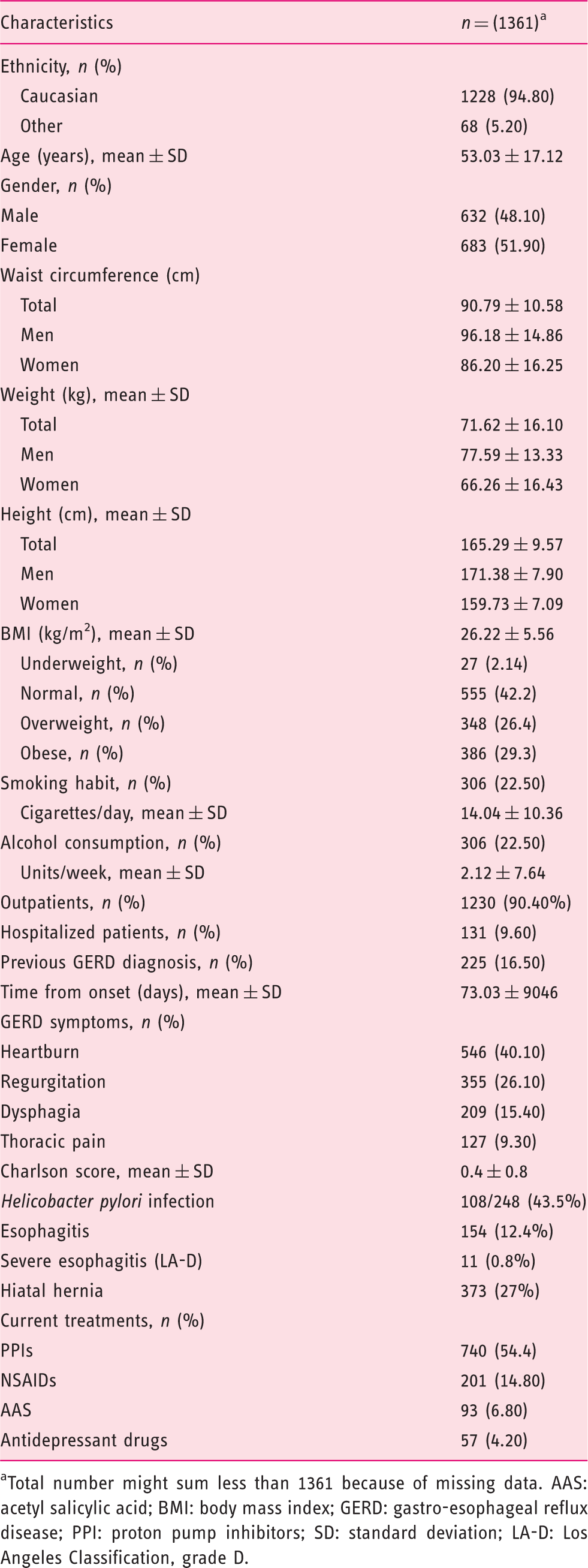
Total number might sum less than 1361 because of missing data. AAS: acetyl salicylic acid; BMI: body mass index; GERD: gastro-esophageal reflux disease; PPI: proton pump inhibitors; SD: standard deviation; LA-D: Los Angeles Classification, grade D.
A total of 225 patients (16.5%) presented with clinical diagnosis of GERD previous to endoscopy. Mean time from symptoms onset was 73.0 ± 90.5 days (range: 1–502 days) (Table 1). The most frequent symptoms prompting endoscopy were heartburn (40.1%), regurgitation (26.1%), dysphagia (15.4%) and thoracic pain (9.3%). Comorbidities were infrequent, with 88.2% of patients having a Charlson score of 1 or lower (Table 1).
More than half of the patients were taking PPIs (continuous or intermittent) (54.4%), while 14.8% were consuming NSAIDs, 6.8% AAS and 4.2%, antidepressant drugs (Table 1). Most patients took PPI at a standard dose either once a day (84%) or twice a day (16%). Both higher doses or half-doses were exceptionally used in this series. In addition, less than 5% of the patients stopped PPI before the endoscopy and, of them, most stopped the drug for less than 10 days.
Most patients underwent endoscopy on an outpatient basis (90.40%), and only 9.6% of patients were hospitalized. Forty-seven percent of patients reported GERD symptoms immediately before endoscopy; the most frequent symptom was heartburn.
Esophagitis (mainly mild to moderate) was present in 154 (12.4%) patients. According to the LAC, 96 patients (66%) were Grade A, 34 (25%) were Grade B, 13 (10%) were Grade C, and 11 (8%) were Grade D. H. pylori was evaluated in 248 patients and infection was present in 108 (43.5%) (Table 1). Hiatal hernia was strongly associated with esophagitis: 22% of patients with hiatal hernia had the condition, compared with only 7% of the patients without hernia.
Univariate analysis: Demographic, clinical and treatment variables according to the presence/absence of esophagitis
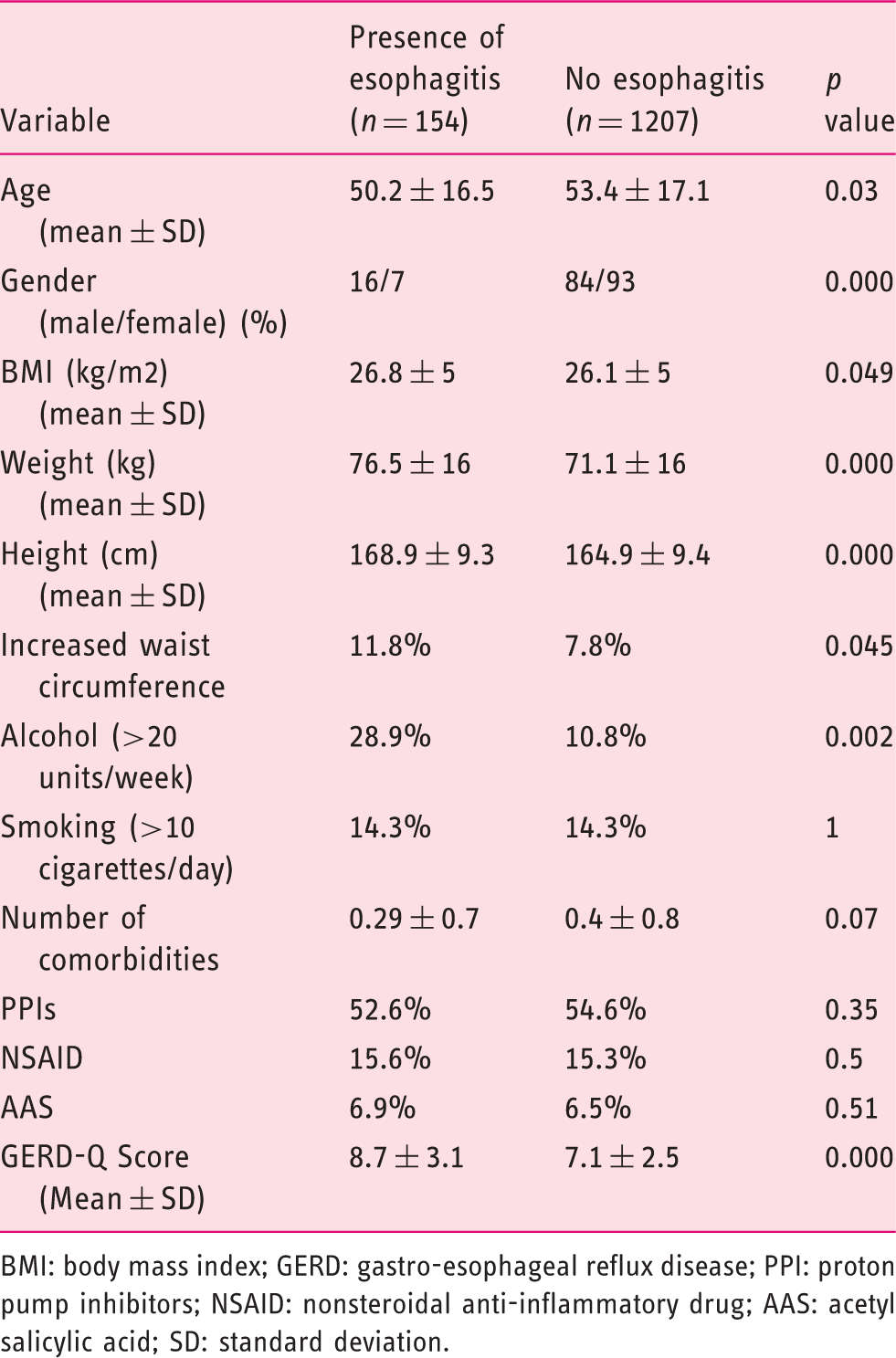
BMI: body mass index; GERD: gastro-esophageal reflux disease; PPI: proton pump inhibitors; NSAID: nonsteroidal anti-inflammatory drug; AAS: acetyl salicylic acid; SD: standard deviation.
Factors predicting esophagitis in the multivariate logistic regression model

GERD: gastro-esophageal reflux disease; CI: confidence interval.
Discussion
The results of this observational, cross-sectional study suggest that esophagitis and severe esophagitis are currently infrequent endoscopic diagnoses in this southern European country. This is the first evaluation of the factors related to esophagitis in a large sample of Spanish patients (>1300 patients) undergoing upper gastrointestinal endoscopy. Assessing a population as large as this one in a southern European setting can provide valuable epidemiological data on the factors influencing esophagitis; it is known that genetic differences, differences in H. pylori prevalence and lifestyle factors like obesity can influence the prevalence of GERD in different geographical contexts. 27 At present, however, the reasons for the variability of its prevalence are still not fully understood. 27
In this regard, among the factors identified in other studies,2,14 we found male gender, GERD-Q score, weight and alcohol consumption to be positively associated with the presence of esophagitis. Our results corroborate those of previous studies.2,13,14,24,28
A recent study assessing the value of the GERD-Q found an association between higher GERD-Q scores and higher proportions of patients with reflux esophagitis. 24 However, the same study found that a low score could not rule out the possibility of reflux esophagitis, and also that a high score cannot exclude the possibility of upper gastrointestinal malignancies. These findings suggest that though GERD-Q may be used to diagnose GERD, endoscopy is still needed for some patients in populations with a high prevalence of upper gastrointestinal malignancies, like the Chinese. 24 Based on this finding and on our results, we think that further studies should be performed in the Spanish population to assess the exact correlation between GERD-Q score and the presence of esophagitis, in order to validate the questionnaire as a diagnostic tool for use in routine clinical practice.
Other risk factors such as male gender, increased weight and higher alcohol consumption were also associated with the presence of esophagitis, as already reported in other populations.2,13,28 However, we did not find an association with smoking status.
We stress the strong association found between esophagitis and high alcohol consumption, as already reported in other populations in which (as in Spain) routine alcohol consumption is widespread.29,30 It is known that consumption of large amounts of alcohol can promote regurgitation of acid into the esophagus and therefore cause GERD symptoms. Most individuals who experience alcohol-related health problems are not addicted to alcohol, but present with a hazardous pattern of alcohol consumption. 29 As a result, both alcohol consumption and hazardous alcohol drinking should always be considered as risk factors for esophagitis.
Interestingly, our study failed to find any significant relationship between NSAID use and esophagitis. NSAID use is known to induce gastroduodenal ulcers and erosions, but our results corroborate previous studies 31 that found that NSAIDs did not play an important role in the pathogenesis of erosive esophagitis.
The incidence of severe grades of esophagitis (C and D) was lower than in other studies.27,32 Fifty percent of patients were receiving a PPI before endoscopy; this high rate of PPI use may have been the reason for the low number of endoscopic lesions. It has already been reported that patients with persistent dyspepsia treated with a PPI have fewer endoscopic abnormalities than patients with dyspepsia receiving H2-receptor antagonists and those receiving no therapy. For patients with partial symptom relief, PPI therapy may mask the endoscopic findings, most probably reducing the prevalence and the severity of esophagitis in the patients receiving PPI. So, many of the esophagitis observed should be considered refractory cases not responding to PPI. It has been suggested that the interruption of PPI for some weeks before endoscopy may improve its diagnostic sensitivity,16,27 but this affirmation remains largely unproven.
The widespread use of PPIs, along with the confounding by indication bias, 33 might also explain why, unlike previous studies,11,16 we did not find a significant protective effect of PPIs for esophagitis.
Among the strengths of the present study are its large sample size and its prospective, multicenter design. Further research is now required in subgroups of Spanish patients, especially in areas where the use of PPIs is lower. A limitation of the study was that, as H. pylori testing was not mandatory, we were unable to adequately investigate the role of the infection in the development of esophagitis. Assessment of risk factors for Barrett’s esophagus in Spanish patients also deserves further research.
Nevertheless, our study provides relevant data on the prevalence and risk factors associated with esophagitis, and has important clinical implications for the assessment of the risk of esophagitis in routine clinical practice in Spanish patients. We conclude that esophagitis is infrequent in the Spanish population, and that severe esophagitis is rare. Male gender, GERD-Q score, weight increase and high alcohol consumption are the main risk factors for esophagitis in our setting.
Footnotes
Acknowledgments
We thank all the participating investigators for their contribution to this study. We also thank Michael Maudsley for his help with the English.
Funding
This work was supported by an unrestricted grant from Astra-Zeneca. CIBERehd is funded by the Instituto de Salud Carlos III.
Conflicts of interest
Xavier Calvet has received grant funding and fees for lectures from: MSD, Abbvie, Vifor-Pharma, Shire and Pfizer. The other authors have nothing to declare.