
Abstract
Background
We previously reported the techniques and usefulness of simultaneous combined balloon-occluded retrograde transvenous obliteration (B-RTO) and partial splenic embolization (PSE), based on the hypothesis that concomitant PSE can diminish the increase in portal venous pressure after B-RTO.
Objective
After experiencing more cases and performing longer-term follow-up, we re-evaluated the efficacy of simultaneous combined B-RTO and PSE for gastric fundal varices (GVs).
Methods
We performed B-RTO in 36 consecutive patients treated for GVs from 2005 to 2013. Twenty-three patients underwent simultaneous combined B-RTO and PSE (Group 1) and 13 underwent B-RTO monotherapy (Group 2). The outcomes were retrospectively evaluated.
Results
There were no significant differences in baseline characteristics between the two groups except that the splenic volumes were larger in Group 1 than 2. B-RTO was technically successful in 21 of 23 patients (91.3%) in Group 1 and in 12 of 13 patients (92.3%) in Group 2. In all patients with ruptured GVs (six in Group 1 and five in Group 2), complete hemostasis was obtained by B-RTO. Exacerbation of esophageal varices was significantly less frequent in Group 1 than 2 (p = 0.0017).
Conclusion
Concomitant PSE with B-RTO may contribute to prevention of the exacerbation of esophageal varices after B-RTO.
Keywords
Introduction
In patients with portal hypertension, the prevalence of gastric fundal varices (GVs) is approximately 30%, which is lower than the prevalence of esophageal varices (EVs).1–3 The reported rate of bleeding in patients with GVs is 3% to 30%.4–7 Rupture of GVs is associated with a higher mortality rate (45%–50%) than rupture of EVs because patients with GVs have more blood flow through the gastrorenal shunt (GRS). Balloon-occluded retrograde transvenous obliteration (B-RTO) is currently widely used in Japan for the treatment of GV.8–11 Its use is gradually increasing in other countries such as the United States,12–14 where transjugular intrahepatic portosystemic shunt (TIPS) placement is currently the standard treatment for GVs. 15 The reported rate of GV rebleeding is significantly lower after B-RTO than after TIPS placement 16 or endoscopic intervention, 17 but B-RTO results in increased portal venous pressure (PVP), which may cause enlargement of EVs.18,19 We previously reported on the efficacy and safety of simultaneous combined B-RTO and partial splenic embolization (PSE) for GVs 20 based on the hypothesis that concomitant PSE can diminish the increase in PVP after B-RTO. After experiencing more cases and performing longer-term follow-up, we re-evaluated the efficacy of simultaneous combined B-RTO and PSE for GVs in the management of portal hypertension with respect to preventing EV exacerbation.
Patients and methods
Patients
We performed B-RTO in 36 consecutive patients treated for GVs at a single institute from 2005 to 2013. Twelve patients had ruptured GVs; eight were treated emergently and four electively. The remaining 24 patients with unruptured GVs were treated prophylactically. Patients were eligible for prophylactic B-RTO if they had GVs with the red color sign, 21 increasing GV size, refractory hepatic encephalopathy due to GRS, and no renal failure. We additionally performed PSE combined with B-RTO in 23 patients (Group 1) with ambiguous indications such as splenomegaly or thrombocytopenia. The remaining 13 patients were treated with B-RTO monotherapy (Group 2). All patients gave informed consent for treatment after a physician had explained the advantages and risks of the procedures. This was not a randomized prospective study; the clinical data were obtained and analyzed retrospectively. The study was approved by the ethics committee of Niigata City General Hospital. The study protocol conformed to the ethics guidelines of the 2008 revision of the Declaration of Helsinki.
B-RTO
GRS was diagnosed by computed tomography (CT) and transarterial portography via the splenic or superior mesenteric artery. An 8-Fr long cobra-shaped (S-one sheath; Terumo Clinical Supply Co., Gifu, Japan) or shepherd hook-shaped (Asato; Medikit, Tokyo, Japan) sheath introducer was advanced to the left renal vein via the right internal jugular or right femoral vein, respectively. A 5.2-Fr catheter with a 9-mm-diameter balloon or 6-Fr catheter with a 20-mm-diameter balloon (Selecon MP Catheter; Terumo Clinical Supply Co.) was advanced through the sheath introducer into the GRS in a retrograde fashion (Step 1). Balloon-occluded retrograde transvenous venography (B-RTV) was performed to identify shunts and their inflowing and outflowing vessels. The stepwise injection method, 22 selective coil embolization of the minor accessory draining veins, 22 and/or the down-grading method 23 was used to down-grade the target shunt vessels to a relatively simple Grade 1 or 2 according to Hirota’s classification 3 (Step 2). Under temporary balloon occlusion, contrast medium was injected via the balloon catheter to confirm stagnation of variceal flow for ≥10 minutes and to evaluate the required volume of sclerosing solution (Step 3). In patients undergoing combined therapy, PSE was performed as described below during temporary occlusion (Step 4). When stagnation of the contrast medium was confirmed, the same volume (10–40 ml) of 5% ethanolamine oleate with iopamidol (EOI) was injected and remained stagnant in the vessels with overnight balloon occlusion (Step 5). The catheter was removed after the overnight occlusion (Step 6). To prevent renal dysfunction secondary to hemolysis caused by EOI, human haptoglobin (4000 units) was administered prior to injection of EOI. All procedures were performed by the same hepatologists.
PSE
PSE (Step 4) was performed while checking retention of the contrast medium in the shunt vessels (Step 3). A 5-Fr catheter was advanced via the right femoral artery to the splenic or celiac artery, and arterial portography was performed before B-RTV. For about 10 minutes during Step 3, a 2.2- to 2.7-Fr coaxial microcatheter was advanced to the hilum of the spleen or to more peripheral splenic vessels. Under fluoroscopic guidance, the splenic arteries were embolized using gelatin sponge pieces cut into approximately 3-mm cubes and immersed in iopamidol. Digital subtraction splenic arteriography was performed as needed to confirm the area of splenic infarction until approximately 60% to 90% of the spleen was infarcted.
The area of splenic infarction and formation of a clot in the target shunt vessels were confirmed by CT four to seven days after the procedure. The percentage of splenic infarction was calculated by comparing the area of unenhanced splenic parenchyma with the area of the whole spleen tracing on the DICOM viewer (Aquarius NET; TeraRecon Inc, Tokyo, Japan) using reconstructed images with 2-mm-thick slices.
Representative case
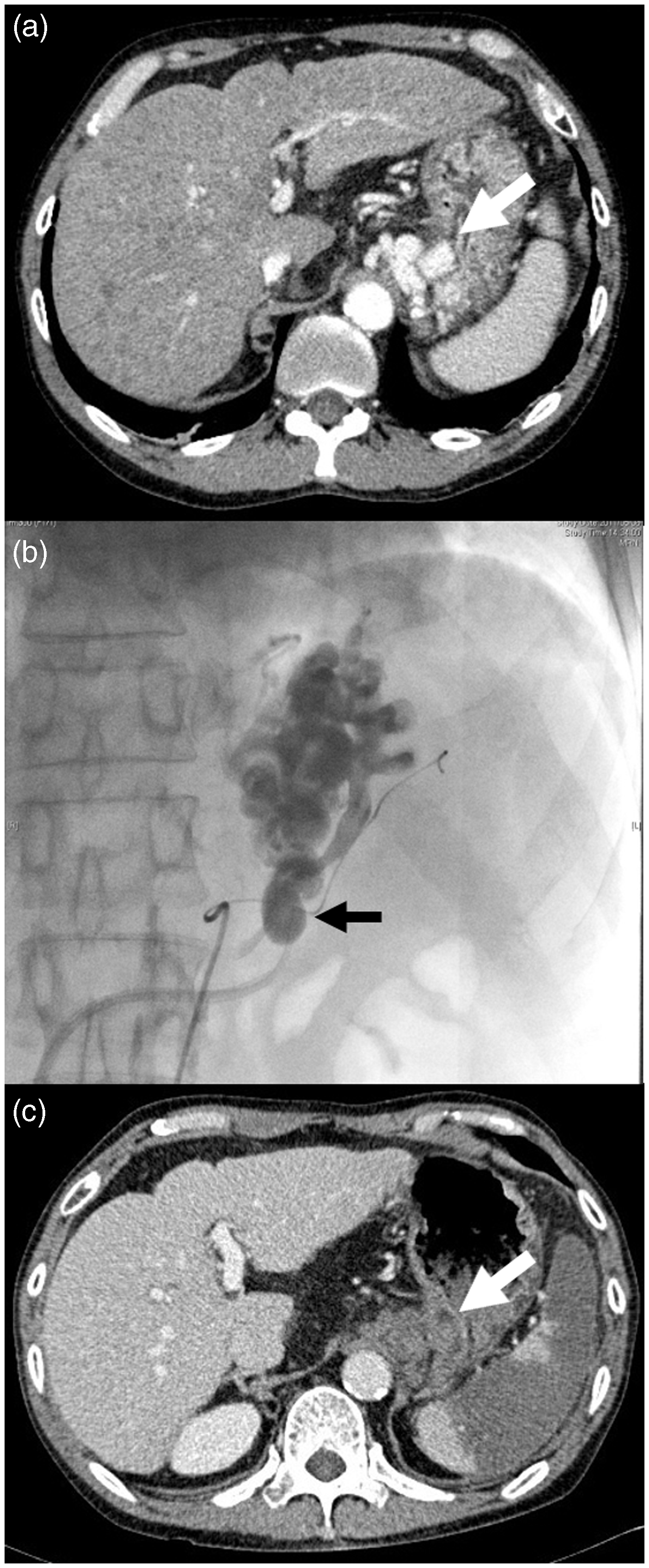
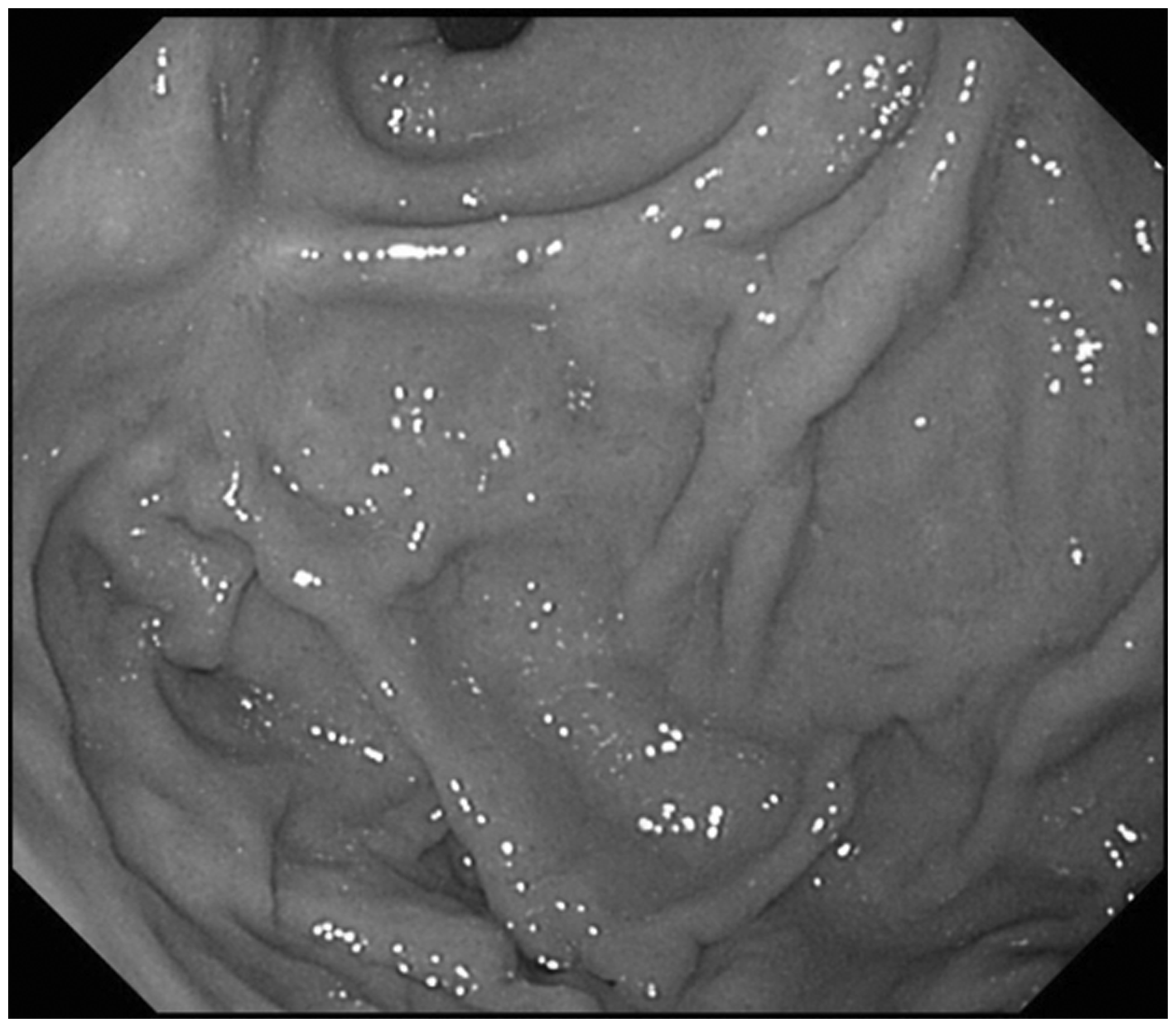
A 60-year-old man with alcoholic liver cirrhosis was admitted because of hematemesis. Emergent endoscopy showed GV with a red plaque, indicating rupture (Figure 1(a)). The hemorrhagic point on the GV was endoscopically ligated to achieve primary hemostasis (Figure 1(b)). Contrast-enhanced CT showed the GV protruding into the gastric lumen and GRS (Figure 2(a)). Simultaneous combined B-RTO and PSE was performed as soon as possible (Figure 2(b)). One week later, repeat CT showed the blood clot in the GV extending to the GRS and the development of splenic infarction (Figure 2(c)). The patient was discharged 15 days after the procedure without complications. Follow-up endoscopic examination after three months showed disappearance of the GV (Figure 3).
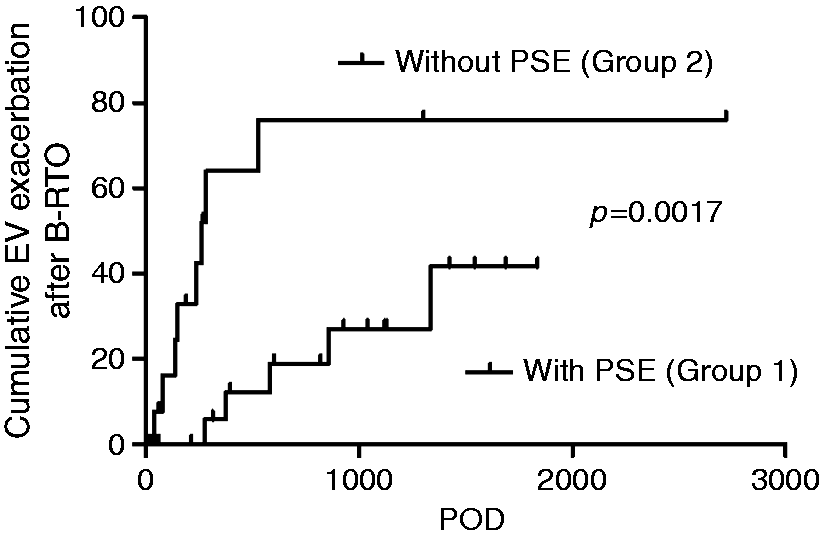
Sixty-year-old man with hematemesis. (a) Emergent endoscopic examination, showing nodular gastric fundal varices with a red plaque of blood clot (arrow). (b) Endoscopic variceal ligation achieved primary hemostasis. Sixty-year-old man with hematemesis. (a) Preprocedure dynamic computed tomography showing gastric fundal varices protruding into the lumen of the stomach (white arrow) and the left gastric vein as an inflow vessel. (b) Partial splenic embolization using gelatin sponge pieces and overnight balloon-occluded retrograde transvenous obliteration using 5% ethanolamine oleate with iopamidol. The position of the inflated balloon is indicated by the black arrow. (c) Dynamic computed tomography after one week showing thrombosis from the left gastric vein via the gastric varices (white arrow) to the gastrorenal shunt. The partially infarcted area of the spleen is also shown. Three months after combined balloon-occluded retrograde transvenous obliteration and partial splenic embolization, the gastric varices had disappeared. Cumulative frequency of exacerbation of esophageal varices (EV) after balloon-occluded retrograde transvenous obliteration (B-RTO) with or without partial splenic embolization (PSE). Exacerbation of EVs was significantly less frequent in Group 1 than in Group 2 (p < 0.0017). In Group 2, most exacerbations of EVs occurred within one year after B-RTO. Group 1: Simultaneous combined B-RTO and PSE. Group 2: B-RTO monotherapy.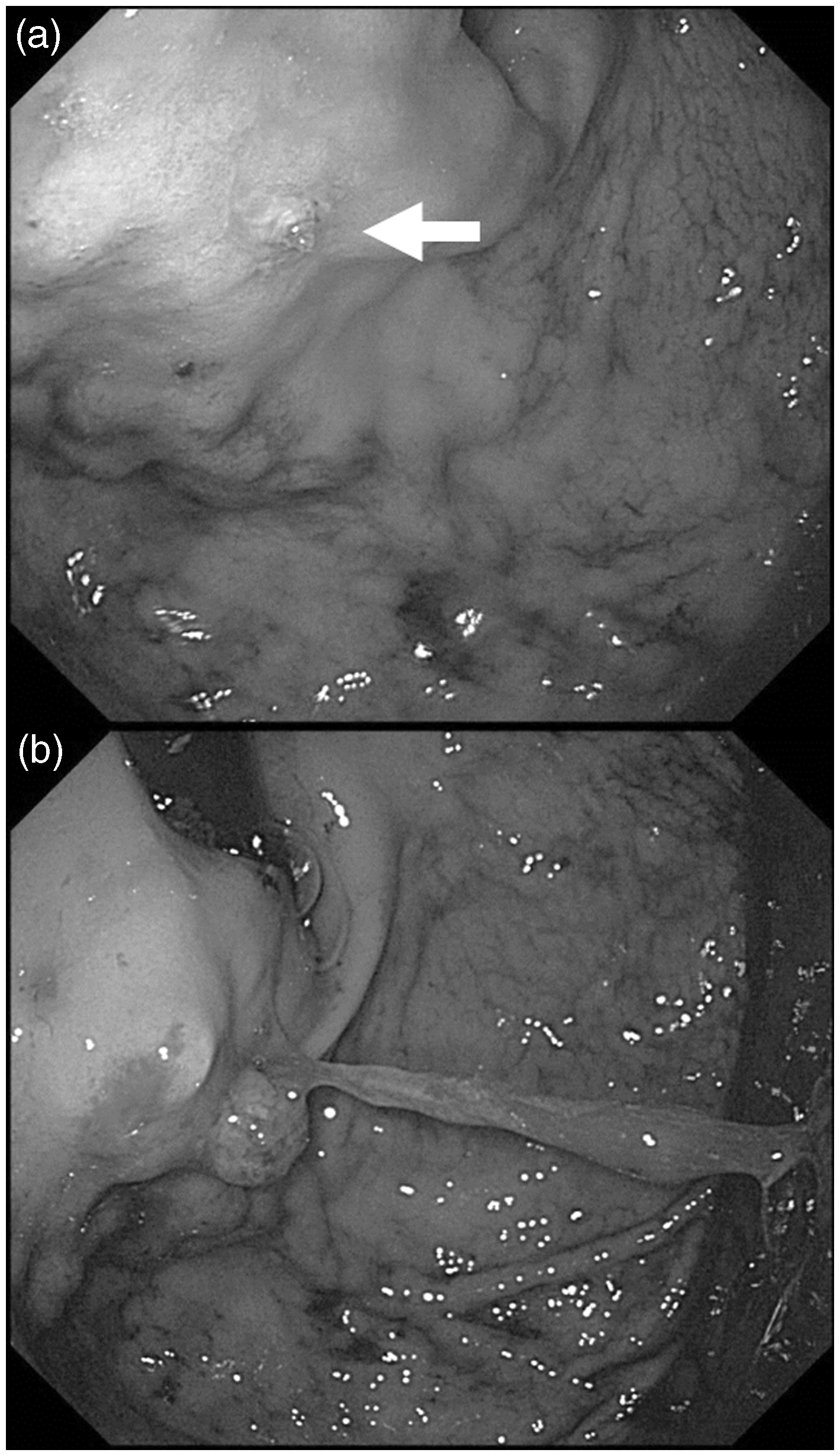
Endpoints of this study
The patients’ baseline characteristics and the status of EVs and GVs were compared between the two groups. The Child-Pugh score was used as the index of hepatic functional reserve for comparison between before and about eight weeks after B-RTO. Hirota’s B-RTV grade 3 was used as an indicator of technical difficulties associated with B-RTO. We evaluated the technical success rate of B-RTO, procedure time, length of postoperative hospital stay, and exacerbation of EVs after B-RTO. Technical success of B-RTO was defined as complete embolization of the GRS and disappearance of the GV. The procedure time was defined as the time from induction of local anesthesia for vascular puncture to leaving the angiography room on the first day (Step 5 of B-RTO). Endoscopic examinations were performed at about two, six and 12 months after B-RTO. During the subsequent follow-up, endoscopic examinations were performed as needed every six to 12 months. Exacerbation of EV was defined as progression of more than one degree in the variceal form or red color sign according to the guidelines of the Japanese Society for Portal Hypertension. 21
Statistical analysis
Statistical analyses were performed using GraphPad Prism 5 statistical software (GraphPad Software Inc, La Jolla, CA, USA). Data are shown as mean ± standard deviation. The chi-squared test and extended Fisher’s exact test were used to compare the frequencies of factors in the contingency tables, and the paired t-test was used to compare pre- and postprocedural data. Nonparametric data were compared between the two groups using the Mann-Whitney U test or Kruskal-Wallis test, and Dunn’s multiple comparisons test was used to compare data among subgroups. Survival curves were estimated using the Kaplan-Meier method and the statistical significance of differences between curves was analyzed using the log-rank test. In all analyses, p < 0.05 was considered statistically significant.
Results
Baseline characteristics of the patients in the two groups (Table 1)
Baseline characteristics of patients in each group
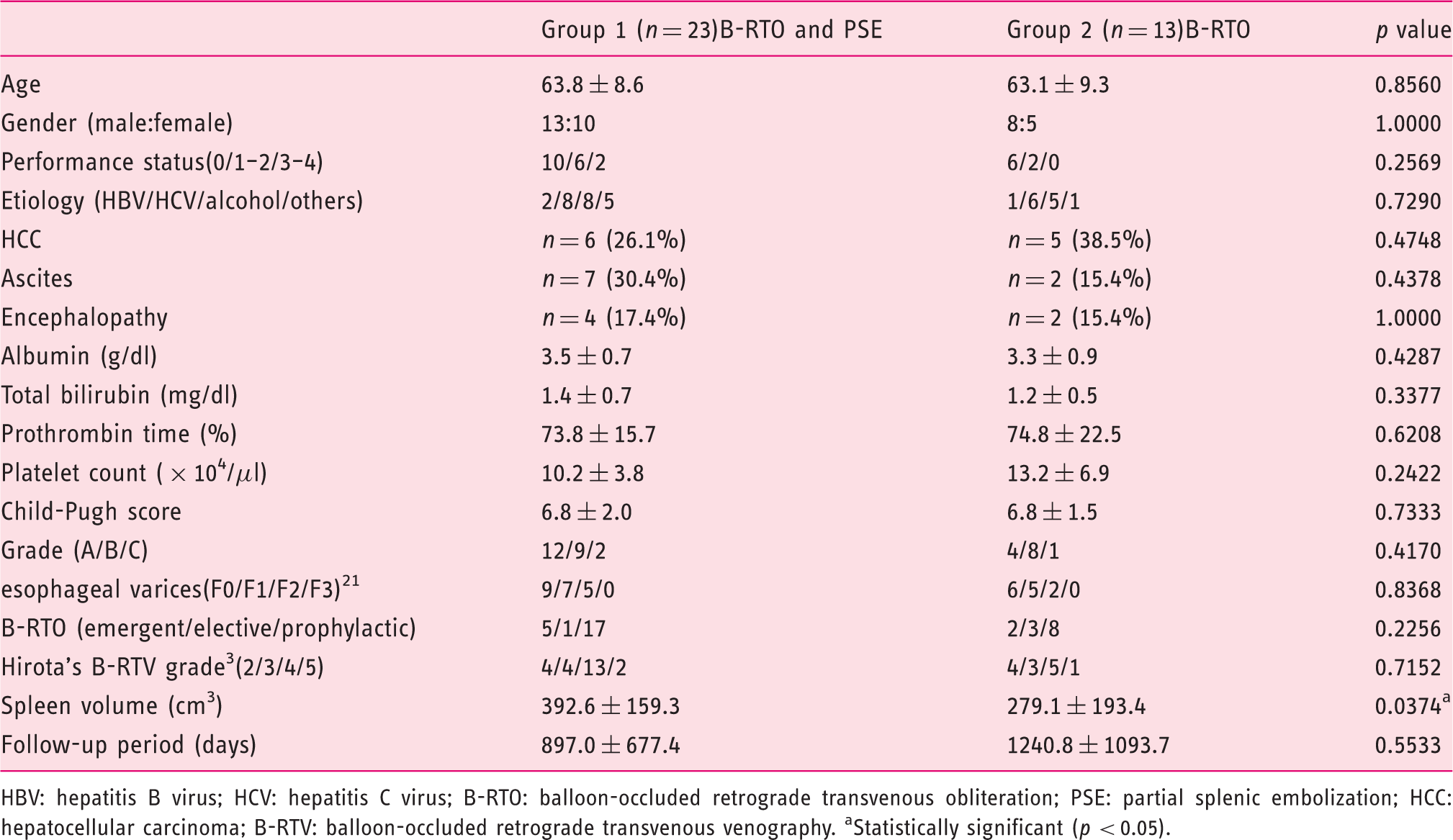
HBV: hepatitis B virus; HCV: hepatitis C virus; B-RTO: balloon-occluded retrograde transvenous obliteration; PSE: partial splenic embolization; HCC: hepatocellular carcinoma; B-RTV: balloon-occluded retrograde transvenous venography. aStatistically significant (p < 0.05).
Effectiveness of combined therapy
B-RTO was technically successful in 33 of 36 patients (91.7%): 21 of 23 (91.3%) in Group 1 and 12 of 13 (92.3%) in Group 2. In all patients with ruptured GVs (six in Group 1 and five in Group 2), complete hemostasis was obtained by B-RTO. In cases of failed B-RTO, it was difficult to simplify the GRS route by selective embolization of the accessory draining vessels. In all cases of successful B-RTO, the GRS was well embolized and the GVs disappeared. The mean procedure time was not significantly different between Groups 1 and 2 (124.3 ± 54.9 vs. 142.7 ± 48.7 minutes, respectively; p = 0.2623). The mean proportion of splenic infarction was 76.8% ± 14.2%, resulting in a significant increase in the platelet count from 10.2 ± 3.8 × 104/µl before the procedure to 19.5 ± 7.6 × 104/µl at one month after the procedure (p < 0.0001). There were no cases of procedure-associated transient thrombocytopenia caused by disseminated intravascular coagulation. The mean injected volume of 5% EOI was significantly smaller in Group 1 than in Group 2 (17.4 ± 5.4 vs. 26.6 ± 9.5 ml, respectively; p = 0.0118). The decrease in the Child-Pugh score was used as an index of the improvement in hepatic functional reserve. The Child-Pugh score decreased significantly in Group 1 (from 6.8 ± 2.0 to 5.7 ± 1.3, p = 0.0217), but did not decrease significantly in Group 2 (from 6.8 ± 1.5 to 6.2 ± 1.4, p = 0.2308).
No recurrence or bleeding of the GVs was seen during the observation period of 1021.1 ± 852.4 days. Bleeding of the EVs was not seen during this same observation period except for one patient with rapid progression of a portal vein tumor thrombus from hepatocellular carcinoma more than four years after B-RTO. In Group 1, the EV exacerbation rate was 5.9% at one year, 18.9% at two years, and 27.0% at three years. In Group 2, the EV exacerbation rate was 64.0% at one year, 76.0% at two years, and 76.0% at three years. The cumulative frequency of exacerbation of EVs after B-RTO was lower in Group 1 than in Group 2 (p = 0.0017) (Figure 4). In Group 2, most exacerbations of EVs occurred within one year after B-RTO. In contrast, exacerbation of EVs during the first year was infrequent in Group 1.
Safety of combined therapy
The postprocedural complications and length of hospital stay were compared between the two groups. The most serious complication was splenic abscess formation, which occurred in two patients (8.7%) in Group 1. One of these patients was a 75-year-old woman with a performance status of 4 who had refractory hepatic encephalopathy and hypertrophic cardiomyopathy. She had a satisfactory initial postoperative course but suddenly died of a splenic abscess 10 days after the procedure. Unfortunately, her postprocedural antibiotic therapy had been discontinued early. The other patient was a 49-year-old woman who developed a splenic abscess because of over-embolization of the spleen (94.4%). She improved after long-term antibiotic therapy and percutaneous aspiration of the abscess. Symptomatic ascites and/or pleural effusion occurred in four patients (17.4%) in Group 1 and five patients (38.5%) in Group 2 (p = 0.2347). Portal and splenic venous thrombosis occurred in two patients (8.7%) in Group 1 and was successfully treated with danaparoid sodium. Minor complications included fever of >38℃ (13.0% in Group 1 vs. 38.5% in Group 2, p = 0.1072) and abdominal pain (21.7% in Group 1 vs. 7.7% in Group 2, p = 0.3854), which were well controlled with nonsteroidal anti-inflammatory medication.
The early mortality rate (six weeks postoperatively) in Group 1 was 12.5% (three of 24 patients), and that in Group 2 was 0.0%. One patient with a GV rupture who already had severe circulatory failure and metabolic acidosis died of hepatic failure the next day despite successful hemostasis by B-RTO and PSE. Another patient who died was the above-mentioned patient who developed a splenic abscess. The remaining patient died of rapidly progressive hepatocellular carcinoma one month after B-RTO and PSE.
The mean length of postoperative hospital stay was not significantly different between Groups 1 and 2 (12.7 ± 4.0 vs. 13.7 ± 6.5 days, respectively; p = 0.4660).
Discussion
In Japan, B-RTO has been used for more than 20 years to stop active GV bleeding or prophylactically prevent GV bleeding.1–4 Application of prophylactic interventions such as B-RTO is controversial. GV rupture is a fatal condition. The patient with GV rupture is not able to survive if not transported to a highly advanced medical institution immediately. In this study, one patient died because of a delay in arrival at our hospital despite successful hemostasis by B-RTO and PSE. Prophylactic treatment is regarded as an effective treatment in Japan, but it is rarely performed in Western countries. 24 We recognize that differences in treatment policies among countries may be associated with differences in health care insurance, medical malpractice systems, and patient expectations of care. 20 In all of our patients with ruptured GVs, complete hemostasis was obtained by B-RTO. B-RTO is highly effective for the treatment of GVs, and there were no cases of GV recurrence after successful B-RTO in this study. In contrast, TIPS placement is the mainstay of treatment for GVs and EVs in Western countries. 15 TIPS placement is a rational treatment for reduction of the PVP; however, the GV rebleeding rate is relatively high. Additionally, the mortality rate after this intervention is relatively high because of serious complications such as hemobilia, sepsis, cardiac failure, hepatic failure, and others. 25 Endoscopic glue (n-butyl-2-cyanoacrylate) injection has also been widely performed, 26 especially in cases of acute bleeding. 27 B-RTO is highly effective in the eradication of GVs. In several studies, B-RTO was superior to TIPS placement and endoscopic interventions for GVs.16,17,27–31 However, B-RTO blocks the GRS, which is a high-flow portosystemic shunt, resulting in increased PVP. Deterioration of EV due to increased PVP after B-RTO is a major issue in the long-term management of these patients.18,19 Starting in 2005, we performed concomitant PSE in some patients undergoing B-RTO to lower the PVP by decreasing the splenic venous flow. We measured the shunt venous pressure as a surrogate measure of PVP in patients who underwent combined therapy and found that the elevation in the shunt venous pressure due to temporary occlusion of the gastrorenal drainage vein with a balloon was diminished. 20 Furthermore, the frequency of exacerbation of EVs after B-RTO was significantly reduced by combining PSE with B-RTO. The results of this study confirm the effectiveness of this treatment strategy over a longer-term follow-up period. The hepatic functional reserve improved more in the combined B-RTO/PSE group than in the B-RTO monotherapy group. We believe that increased portal vein blood flow after B-RTO leads to improvement in the hepatic functional reserve.19,32 However, our results show that combining PSE with B-RTO was more effective than B-RTO monotherapy. The increase in portal vein blood flow after B-RTO is mainly due to increased splenic venous blood flow, without a substantial increase in hepatopetal mesenteric venous blood flow. We speculate that the hepatopetal mesenteric venous blood flow increases after the splenic venous blood flow is decreased by PSE, resulting in improvement of the hepatic functional reserve.
Unfortunately, we found no previous reports proposing a hypothesis similar to our speculation. It would be interesting to measure the blood flow in the portal system using Doppler ultrasonography before and after B-RTO with or without PSE.
We would like to determine when it is beneficial to add PSE to B-RTO. Several studies have demonstrated the usefulness of temporary balloon occlusion of the splenic artery during B-RTO.33,34 We speculate that decreasing the splenic blood flow by PSE results in a reduction of the diameter of the shunt vessel. In our experience, addition of PSE helped to achieve successful B-RTO in some cases in which it was difficult to simplify the route of the GRS. The lower volume of 5% EOI required for the combined procedure also indicates that a reduced splenic blood flow may have a favorable effect on the outcome after B-RTO. We consider that the performance of PSE after B-RTO is not therapeutically rational. Chikamori et al. 35 reported the detailed hemodynamic effects of combined PSE and B-RTO when PSE was performed about two weeks before B-RTO. This may be a good method for collecting data. We performed simultaneous combined B-RTO and PSE to avoid prolonging the hospital stay and to avoid performing two separate invasive procedures.
Two unexplained results were obtained in this study. First, the mean procedure time in Group 1 was slightly shorter than that in Group 2. Because we perform PSE during the intermission of the B-RTO procedure in Step 3, additional time is not required to perform PSE. Furthermore, improvements in technical skill with case accumulation contribute to shortening of the procedure time. Second, the mean length of the postoperative hospital stay in Group 1 was slightly shorter than that in Group 2. This may be explained by the fact that there were slightly more patients with postoperative ascites in Group 2, resulting in delayed discharge. However, the procedure time and length of postoperative hospital stay were not significantly different between Groups 1 and 2.
This study is limited by its retrospective and nonrandomized design. However, GV is a relatively rare condition that may require emergent treatment, and it is difficult to perform a prospective, randomized study of patients with GVs. Further accumulation of clinical data, including multicenter reports of patient outcomes, will help to determine the optimal therapeutic procedures for GVs.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.