
Abstract
Background
Due to the high mortality and morbidity rates of esophagectomy, endoscopic mucosal resection (EMR) is increasingly used for the curative treatment of early low risk Barrett’s adenocarcinoma.
Objective
This retrospective cohort study aimed to assess the prevalence of lymph node metastases (LNM) in submucosal (T1b) esophageal adenocarcinomas (EAC) in relation to the absolute depth of submucosal tumor invasion and demonstrate the efficacy of EMR for low risk (well and moderately differentiated without lymphovascular invasion) EAC with sm1 invasion (submucosal invasion ≤500 µm) according to the Paris classification.
Methods
The pathology reports of patients undergoing endoscopic resection and surgery from January 1994 until December 2013 at one center were reviewed and 54 patients with submucosal invasion were included. LNM were evaluated in surgical specimens and by follow up examinations in case of EMR.
Results
No LNM were observed in 10 patients with sm1 adenocarcinomas that underwent endoscopic resection. Three of them underwent supplementary endoscopic eradication therapy with a median follow up of 27 months for patients with sm1 tumors. In the surgical series two patients (29%) with sm1 invasion according to the pragmatic classification (subdivision of the submucosa into three equal thirds), staged as sm2-3 in the Paris classification, had LNM. The rate of LNM for surgical patients with low risk sm1 tumors was 10% according to the pragmatic classification and 0% according to Paris classification.
Conclusion
Different classifications of the tumor invasion depth lead to different LNM risks and treatment strategies for sm1 adenocarcinomas. Patients with low risk sm1 adenocarcinomas appear to be suitable candidates for EMR.
Keywords
Introduction
En bloc esophagectomy, which has been shown to result in better survival for each stage of esophageal adenocarcinoma, 1 is still a major surgical procedure associated with a considerable risk of morbidity and mortality, 2 and requires a high standard of skills and experience. Endoscopic mucosal resection (EMR) offers an attractive alternative to the removal of early esophageal adenocarcinoma given the lower risk of lymph node metastases (LNM) compared with squamous cell carcinoma. 3 It also allows for complete histopathological assessment and indirect assessment of the presence of LNM, since the depth of tumor invasion has been shown to correlate strongly with the rate of LNM in adenocarcinoma. 4
It has to be noted that with EMR the depth of submucosal resection is not well controlled and this poses certain limitations. To overcome this problem, most studies have therefore evaluated surgical resection specimens to assess submucosal (sm) invasion depth instead of EMR specimens. Dividing the submucosa into three equal thirds (pragmatic classification) is considered a reliable subclassification of the submucosa only in surgical specimens. On the other hand, the Paris classification for columnar epithelial tumors of the esophagus defines sm1 invasion as tumor extension into the first 500 µm of submucosal layer and thereby differentiates sm1 from sm2-3 esophageal adenocarcinomas. 5
Some studies have attempted to stratify patients into low and high risk groups for LNM and feasibility of EMR based on histopathological features of the EMR specimen.6–8 Poor tumor differentiation and lymphovascular invasion (LVI) always designate a patient to a high risk group, independent of tumor invasion depth. Vieth et al. consider all submucosal cancers to be “high” risk, 8 while Manner et al. regarded invasion of the upper submucosal third in conjunction with the absence of LVI and good to moderate tumor differentiation as features of “low” risk adenocarcinoma.6,7 In recent literature a growing number of researchers share the view that endoscopic therapy for esophageal adenocarcinomas is justified only for selected “low” risk cases.9,10
The primary aim of this study was to assess the prevalence of lymph node metastases in submucosal esophageal adenocarcinomas (T1b) in relation to the absolute depth of submucosal tumor invasion. We further sought to demonstrate both the efficacy of EMR for low risk sm1 adenocarcinomas and the impact of various definitions of sm1 invasion on subsequent clinical management and LNM involvement.
Methods
Patients
The pathology reports of all patients who underwent surgery or EMR for adenocarcinoma of the distal esophagus or the gastroesophageal junction (GEJ) at Erasmus Medical Center during the period from January 1994 until December 2013 were reviewed. Only patients with submucosal invasion were included. Patients with mucosal adenocarcinomas only or tumor invasion beyond the submucosa were excluded. In the event of neoadjuvant chemotherapy or radiotherapy, patients were excluded because of the potential impact on prognosis and survival. Evidently, patients could not be included when adequate slides or pathology blocks were unavailable for review (Figure 1).
Flowchart of patients with T1b tumors that underwent review of their medical records and pathological review of their EMR and surgical specimens. EAC, esophageal adenocarcinoma; T1b, submucosal tumors; T1a, intramucosal tumors; sm, submucosal invasion.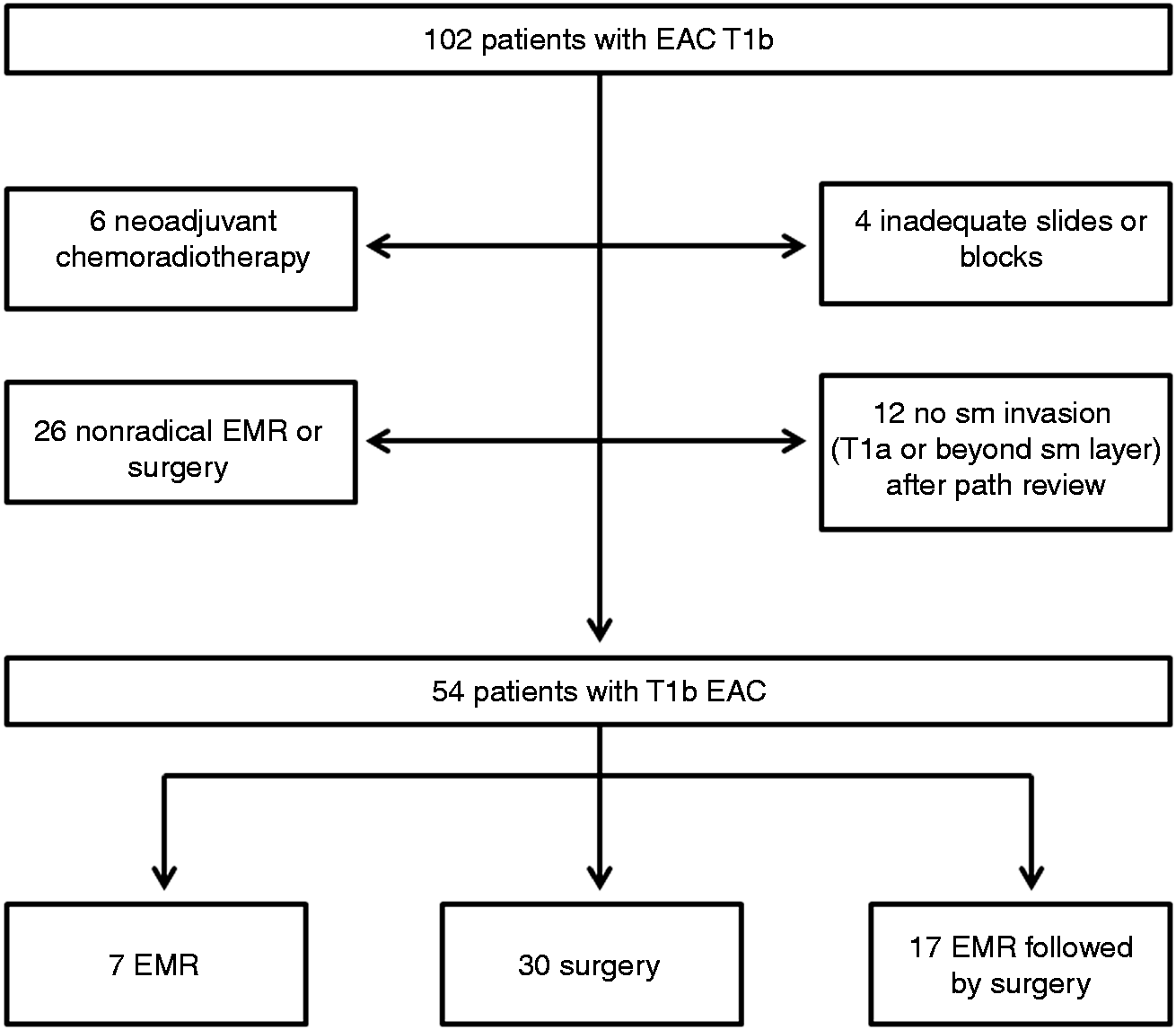
In case of tumor positive vertical resection margins after EMR, the specimen could not be evaluated with regard to the depth of infiltration. If such patients underwent subsequent surgical resection, the surgical specimen was used for assessment of tumor invasion depth and the presence of LNM.
Initial evaluation and management
Patients were initially evaluated in Erasmus Medical Center with standard and high resolution endoscopy at a later date and endoscopic ultrasound (EUS) to assess the depth of infiltration and lymph node involvement. Biopsies were obtained and EUS with fine needle aspiration (FNA) was performed in the case of a suspicious lymph node to exclude LNM. In the latter case, additional CT scanning was also performed.
Surgical excision of adenocarcinoma was decided for patients with cancer invading the submucosal layer, lesions deemed too large for endoscopic resection and in case of suspected or proven lymph node involvement. If a patient refused to undergo surgical excision or was unfit for surgery, EMR was performed. Patients with mucosal cancers and elevated lesions without endoscopic signs of invasive features usually underwent EMR, which was introduced in 1999 in the Erasmus Medical Center.
Endoscopic resection
Patients underwent endoscopic resection either with “capped-EMR” or with multiband mucosectomy (MBM).
All specimens were retrieved and pinned down on cork without any attempt to reconstruct the lesions. In piecemeal resections, the pathologist evaluated only the vertical margins, while the lateral margins were already endoscopically estimated.
Histological evaluation
Resected specimens were fixated (8% formaldehyde), step-sectioned by 2–5 mm intervals (EMR and surgical resection specimens respectively), cut in 4 µm thick slides, and stained with hematoxylin and eosin (H-E).
All slides were revised and evaluated by two independent gastrointestinal pathologists, according to the latest World Health Organization (WHO) classification. The deepest levels of invasion of the tumor in the submucosa (sm levels 1–3) and the total width of the sm were measured. In cases where the lamina muscularis mucosae (mm) was duplicated, submucosal invasion was calculated under the deepest layer of mm (true lamina muscularis mucosae). 11 In the surgical resection specimens without residual tumor after EMR, the total width of the sm was measured above the Squamo-columnar junction. The mean value of three measurements in three different slides is reported. Additionally, features such as presence of LVI, tumor size and differentiation grade (classified as good [G1], moderately [G2], and poorly differentiated [G3] adenocarcinoma in accordance with the WHO classification 2010), lymph node status (in the surgical specimens), and vertical margin (in the EMR specimens) were evaluated. The vertical margins in the EMR specimens were measured in the central region of the slides, because at that point the artifacts due to the surgical procedure were less visible or absent. In case of EMR followed by surgery, the deepest level of tumor invasion in either specimens determined the T stage of the tumor. Specimens (surgical or EMR) in which the deepest tumor front could not be properly revised were excluded.
Subsequent management
Further treatment was tailored for each patient depending on the histopathological analysis of the EMR specimen, the biopsy results from residual Barrett’s mucosa and fitness for surgery. Patients were treated surgically in case of non-radical EMR, G3 tumors, and lymphovascular or submucosal invasion.
Endoscopic eradication therapy using argon plasma coagulation (APC), photodynamic therapy (PDT), radiofrequency ablation (RFA), and stepwise EMR was applied to the rest of the patients when there were residual suspicious for neoplastic lesions, high grade dysplasia (HGD) or residual areas of Barrett’s mucosa.
Follow up
Follow up data were obtained from reviewing patients’ medical records. The date of recurrence, death and last follow up were noted. Follow up time was calculated from the date of first medical procedure, either surgery or EMR, to date of death or date of the most recent clinical, endoscopic or radiologic investigation. Patients were followed up after a complete EMR, every 3–6 months during the first year and annually thereafter. Follow-up investigations included endoscopy with high-resolution endoscopes and biopsies in residual Barrett’s mucosa. An EUS examination was included to assess lymph-node status. In case of missing follow up data, the general practitioner was contacted for additional information.
Outcome of the study
The primary outcome of the study was the occurrence of LNM. This was assessed by examining the presence or absence of LNM in surgical resection specimens whenever available and by follow-up during which time CT scan and/or EUS with or without FNA were performed on indication. In our study low risk adenocarcinomas are defined as tumors with G1-2 differentiation and no LVI.
Statistical methods
The data were analyzed descriptively by using absolute and relative frequencies, means, ranges, minimum and maximum values. The interquartile range (IQR) and median were used to describe data with a skewed distribution.
Results
The study population consisted of 54 patients with a T1b adenocarcinoma. Seven patients had undergone only EMR, 17 patients underwent first EMR and subsequent surgery mainly because of the submucosal tumor invasion, and 30 patients underwent surgery only. Transthoracic excision was performed in five patients, while trans hiatal resection was carried out in 42 of the 47 patients. The median number of resected lymph nodes was 12, ranging from 3 to 28, which is the recommended minimum LN count for a greater than 90% staging sensitivity. 12 The capped-EMR technique was used in 19 patients and the MBM technique in 5 patients.
Histopathological analysis of EMR specimens
The width of the submucosal layer in EMR specimens ranged from 400 µm to 4180 µm with a median of 1715 µm (IQR 1017.5–2262.5 µm). The infiltration depth in sm1 adenocarcinomas ranged from 30 µm to 400 µm with a median of 85 µm (IQR 52.5–210 µm). Sm2-3 tumor invasion was observed in 14 patients with depth of infiltration ranging from 560 µm to 2910 µm with a median of 970 µm (IQR: 705–1232.5 µm).
Outcome-histopathological analysis of patients that underwent EMR and subsequent surgery
Histopathology of patients that underwent EMR followed by surgery
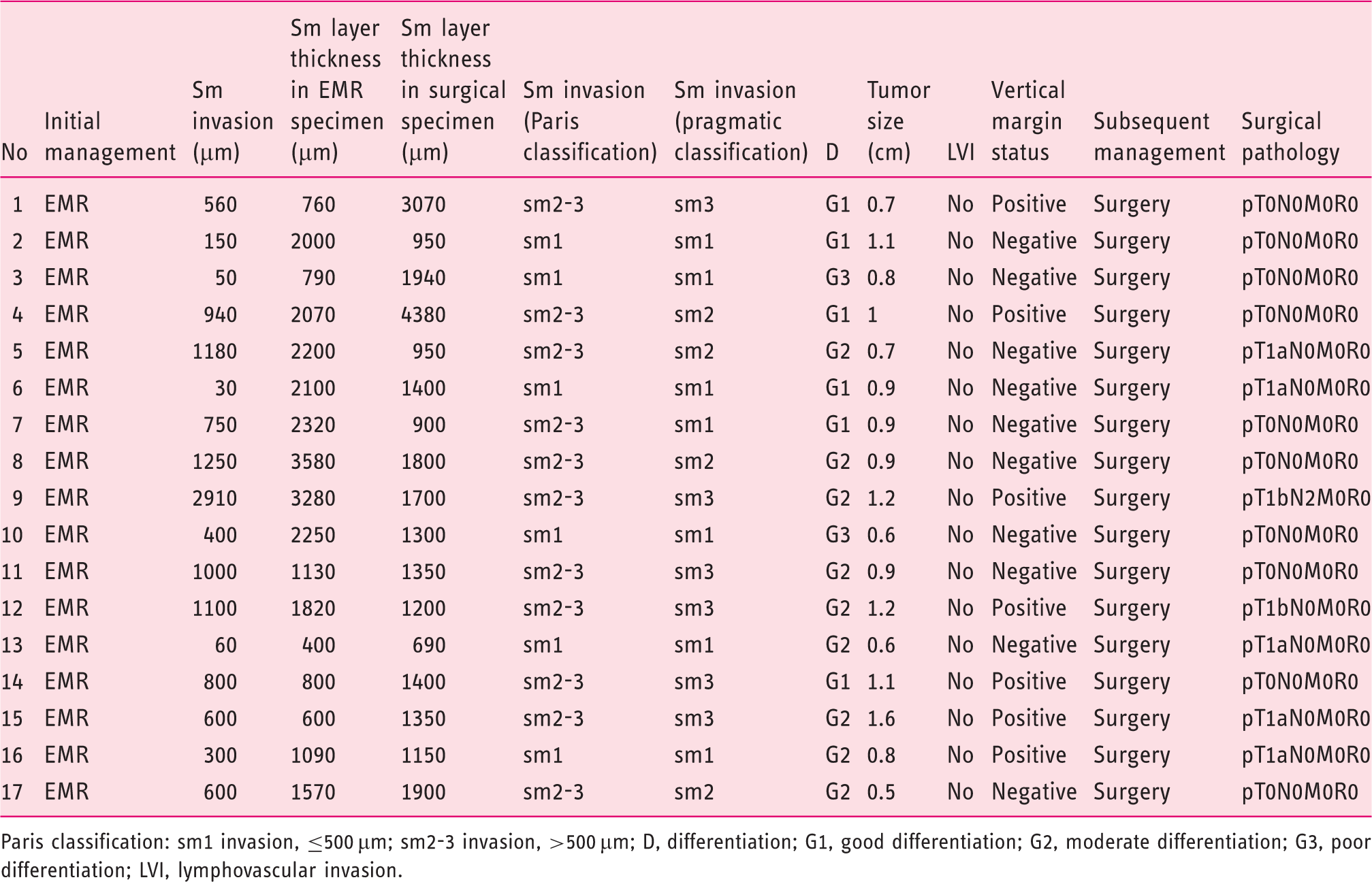
Paris classification: sm1 invasion, ≤500 µm; sm2-3 invasion, >500 µm; D, differentiation; G1, good differentiation; G2, moderate differentiation; G3, poor differentiation; LVI, lymphovascular invasion.
Outcome of patients that underwent only EMR
Histopathology and outcome of patients that underwent only EMR
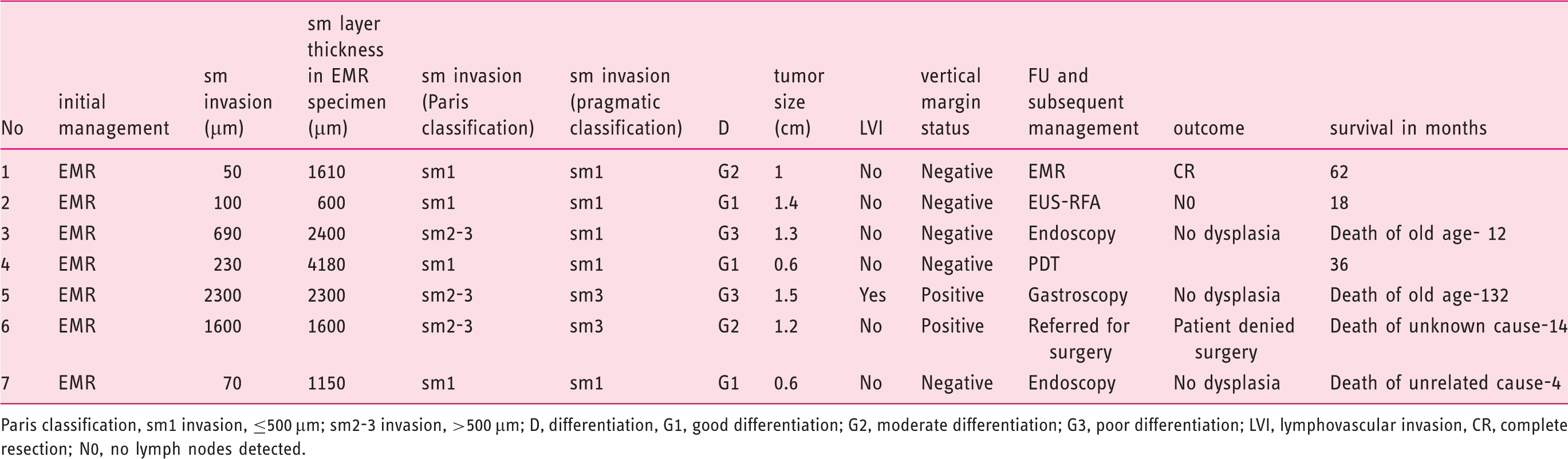
Paris classification, sm1 invasion, ≤500 µm; sm2-3 invasion, >500 µm; D, differentiation, G1, good differentiation; G2, moderate differentiation; G3, poor differentiation; LVI, lymphovascular invasion, CR, complete resection; N0, no lymph nodes detected.
Among sm1 patients, RFA and PDT were applied in two after EMR with complete eradication of Barrett’s mucosa. A complementary EMR was performed for the remaining patient who had a suspicious lesion, which proved to be HGD. One patient with sm1 invasion (T1sm1 G1) had a follow up endoscopy which showed complete eradication of dysplasia and metaplasia, but died of a tumor unrelated cause 4 months later. Unfortunately no imaging or autopsy findings are available for this patient. Two of the patients with sm2-3 tumors died of other causes 12 and 132 months after EMR, while one patient with sm2-3 neoplasia died of an unknown cause 14 months later.
Histopathological analysis of surgical specimens
Histological outcome of surgical resection specimens in the patients who underwent only surgery
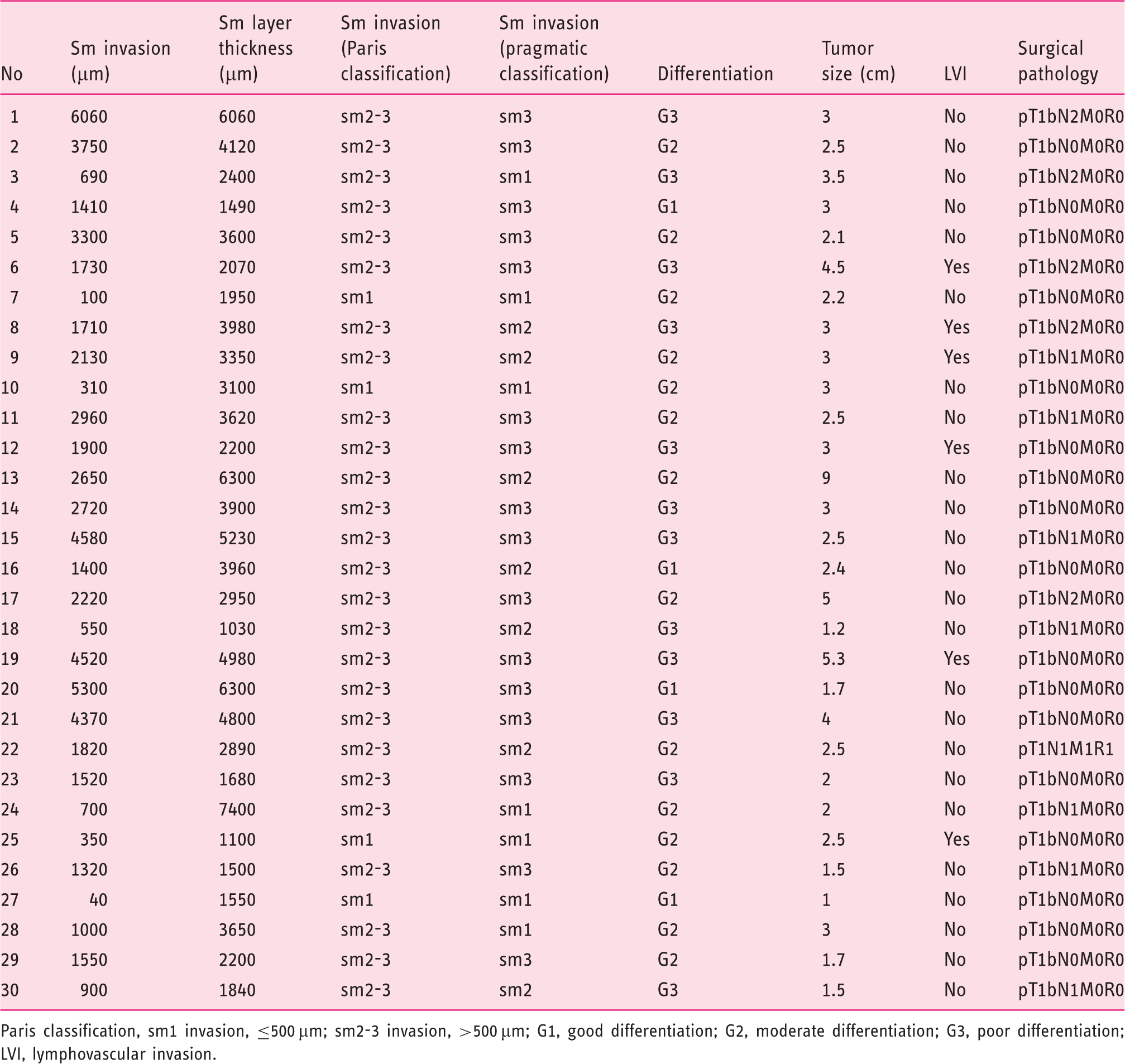
Paris classification, sm1 invasion, ≤500 µm; sm2-3 invasion, >500 µm; G1, good differentiation; G2, moderate differentiation; G3, poor differentiation; LVI, lymphovascular invasion.
Twenty-three patients presented sm2 and sm3 tumors according to the pragmatic classification with a median tumor infiltration depth of 2130 µm (IQR 1535–3525 µm); all had tumor infiltration beyond 500 µm into the submucosa and thus according to the Paris classification were classified into the sm2-3 group. LNM was observed in 11 of the 23 of patients (48%) with sm2 and sm3 tumors. If a subdivision to sm2 and 3 was made, 5 of the 7 patients with sm2 tumors (71%) and 6 of the 16 patients with sm3 tumors (38%) had LNM. The median number of resected lymph nodes per patient was 11 (IQR 7–14).
Discussion
The high rates of morbidity and mortality in elderly patients, 13 and the poor quality of life after esophagectomy, 14 have prompted clinicians to search for expanded but safe indications for EMR, in particular in the case of sm1 adenocarcinomas. The present study demonstrates the efficacy of EMR for low risk sm1 adenocarcinomas and assesses the impact of various definitions of sm1 invasion (Paris and pragmatic classification) on subsequent clinical management and LNM involvement.
Manner et al. and Herrero et al. suggest that it is safe to rely on endoscopic resection in case of sm1 invasion in patients with low risk adenocarcinomas, which are defined as tumors with G1-2 differentiation and no LVI. Manner et al. showed that 87% of patients had a complete endoluminal resection with 84% long term remission, while Herrero et al. found no LNM even in sm2-3 adenocarcinomas, both in surgical specimens and during a follow up period of 26 months after EMR.7,15 Likewise, we did not observe LNM in 10 patients with T1b sm1 adenocarcinomas that underwent EMR, while two of them are high risk patients having G3 adenocarcinomas. Median follow up after EMR for our patients with sm1 tumors was 27 months (IQR 14.5–42.5 months). Six patients had surgery after EMR with no LNM, three patients had supplementary endoscopic eradication therapy and one patient died of other causes after having undergone two follow-up endoscopies negative for dysplasia. The absence of LNM strongly suggests that EMR is a safe and effective treatment modality in low risk T1b sm1 adenocarcinomas.
Definitions of the extent of the first submucosal layer vary in different studies which renders generalization of conclusions impossible. Most studies have used a pragmatic approach of subdividing the sm layer in three equal parts.7,8 This was decided because the exact measurement in microns of the depth of infiltration was considered to be highly variable and affected by the artifactual shrinkage due to fixation. 8 Indeed, Ancona et al. reported that the base of an endoscopically resected sample shrinks both due to cauterization damage and due to the effect of the muscularis mucosae making the submucosa wrinkle. 9 Artifactual shrinkage cannot be avoided and the extent of shrinkage cannot be predicted or measured. Importantly, the pragmatic classification is inadequate in its ability to define the exact depth of tumor infiltration because in most cases the complete submucosal layer is not included in the EMR specimen. In our opinion, it is logical to follow the widely accepted Paris classification, which if adopted more widely, offers a reliable comparison of results among different studies.
Peters et al. emphasized the inaccuracy of the pragmatic-practical classification considering the discrepancies they found between absolute measurements of tumor invasion in micrometers and practical measurements based on subdivision of the sm layer. In their series, cancers classified as sm2 had a small absolute submucosal penetration depth of only 120 and 200 micrometers. 16 In our study, two patients with sm1 tumors according to pragmatic classification are staged as sm2-3 tumors according to the Paris classification. Importantly, different classifications of sm involvement amount to totally different management strategies, if endoscopic resection is to be regarded as the treatment of choice for low risk sm1 adenocarcinomas and surgical resection for lesions extending beyond sm1. The rate of the class divergence for the same patient amounts to 8% for EMR patients in the present study, but could be higher depending on the level of tumor invasion in relation to the resected part of the submucosa. Because even a few microns of tumor invasion may dramatically alter the assumed risk for lymph node metastases and hence the choice for endoscopic or surgical treatment, pathological assessment and reporting should be standardized.
Lymph node positivity in sm1–3 depth of infiltration in surgical specimens: results in the literature
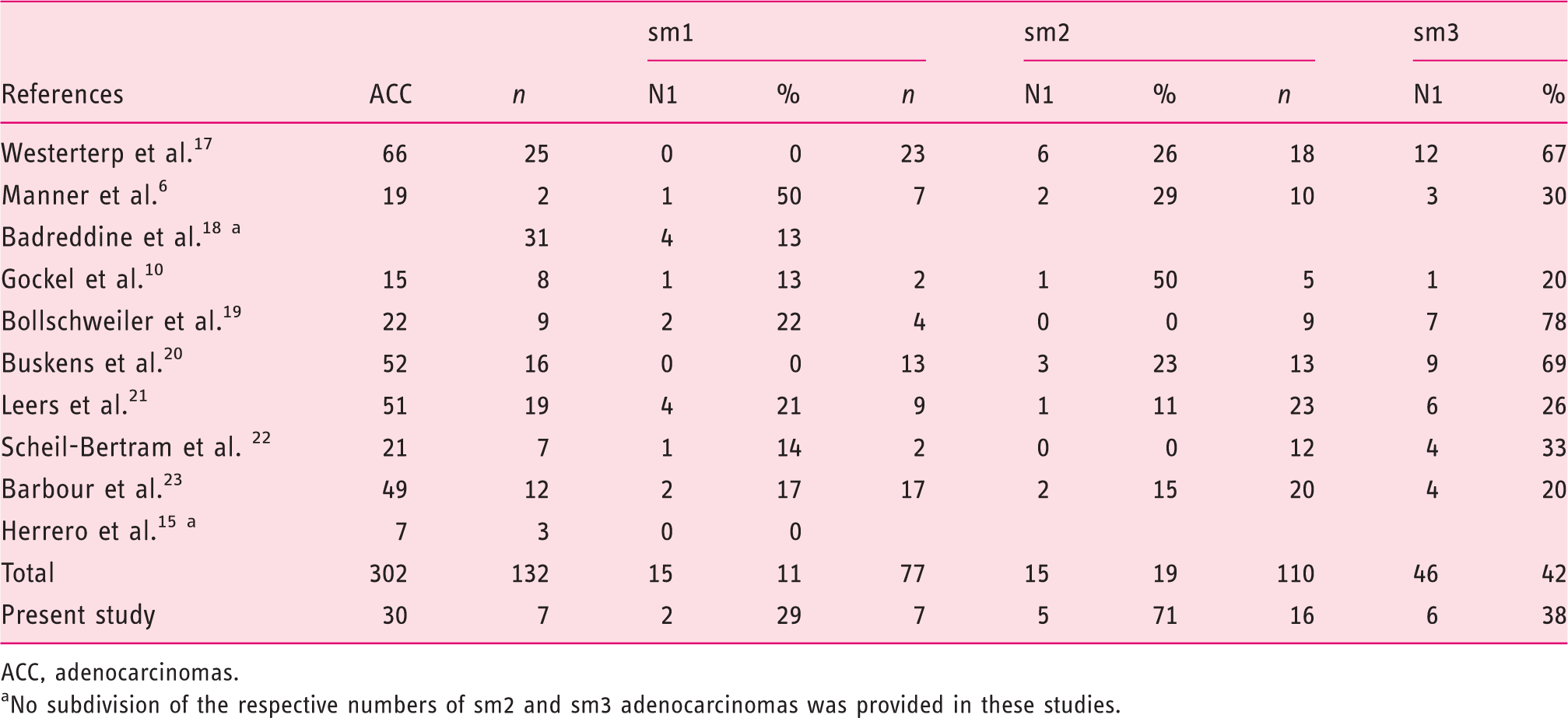
ACC, adenocarcinomas.
No subdivision of the respective numbers of sm2 and sm3 adenocarcinomas was provided in these studies.
Rate of LNM for surgically treated patients with sm1 EAC according to Paris and pragmatic classification and risk of histological parameters

LNM; lymph node metastases, sm; submucosal invasion, EAC; esophageal adenocarcinoma.
Including patients that underwent EMR before surgery.
Due to the retrospective nature of our analysis, it was not possible to control for specimen slicing and preparation of histologic slides, which limited the assessment of the deepest tumor margin. While surgical resection specimens are routinely cut in 5-mm slices, endoscopic resection specimens are routinely cut in 2-mm slices, making it possible defining more precisely the areas with the deepest infiltration. This fact renders any correlation between LNM risks in EMR and surgical patients difficult, a problem already highlighted by Herrero et al. 15 Another limitation of this study is the inability to completely exclude the presence of LNM in patients who did not underwent esophagectomy after EMR. The limited median follow up period of 18 months and the relative inaccuracy of EUS for the diagnosis of LNM, do not allow to conclude with absolute certainty that LNM are truly absent.
There is little doubt that early recognition of early esophageal cancer will lead to an increase in the detection and treatment of sm1 adenocarcinomas. The decision for endoscopic or surgical treatment of sm1 adenocarcinomas should be based on reliable classification of the tumor invasion depth. The pragmatic approach of subdividing the sm layer in three equal parts is unreliable due to the fact that the submucosal layer often is not fully included in EMR resection specimens. However, patients with low risk tumors (G1/G2 tumors with no LVI) and less than 500 µm tumor invasion depth into the submucosa appear to be suitable candidates for endoscopic therapy with excellent clinical outcome. Therefore, the key requirement for proper patient selection and management is uniform and standardized assessment and reporting of histopathological examinations of EMR specimens.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.