
Abstract
Background
In humans there are epidemiological data suggesting a protective effect of Helicobacter pylori (H. pylori) infection against the development of autoimmune diseases and in addition, there are laboratory data illustrating H. pylori’s ability to induce immune tolerance and limit inflammatory responses. Thus, numerous observational studies have examined the association between H. pylori infection and inflammatory bowel disease (IBD) with various results.
Objective
We performed a meta-analysis of available studies to better define the association of H. pylori infection and IBD.
Methods
Medical literature searches for human studies were performed through September 2014, using suitable keywords. In each study the risk ratio (RR) of H. pylori infection in IBD patients vs controls was calculated and pooled estimates were obtained using fixed- or random-effects models as appropriate. Heterogeneity between studies was evaluated using Cochran Q test and I2 statistics, whereas the likelihood of publication bias was assessed by constructing funnel plots.
Results
Thirty-three studies were eligible for meta-analysis, including 4400 IBD patients and 4763 controls. Overall 26.5% of IBD patients were positive for H. pylori infection, compared to 44.7% of individuals in the control group. There was significant heterogeneity in the included studies (Q = 137.2, df (Q) =32, I2 = 77%, p < 0.001) and therefore the random-effects model of meta-analysis was used. The obtained pool RR estimation was 0.62 (95% confidence interval (CI) 0.55–0.71, test for overall effect Z = –7.04, p < 0.001). There was no evidence of publication bias.
Conclusion
The results of this meta-analysis showed a significant negative association between H. pylori infection and IBD that supports a possible protective benefit of H. pylori infection against the development of IBD.
Introduction
Inflammatory bowel disease (IBD), including ulcerative colitis (UC) and Crohn’s disease (CD), is a significant, growing global health burden.1–3 In recent decades, many developing countries have seen a dramatic rise in the incidence of IBD.2–4 It is speculated that improved access to a cleaner environment and the resulting decreased incidence of common childhood infections may be contributing to this rise by altering susceptibility to certain diseases with an autoimmune component, such as IBD.5,6 Thus, according to this speculation, microbial infections during childhood may protect from IBD.
Helicobacter pylori is a bacterium that causes chronic gastritis and consequently mainly peptic ulcer disease and to a less extent, mucosa-associated lymphoid tissue (MALT) lymphoma and gastric cancer in infected individuals.7,8 The inflammatory response of the gastric mucosa is mainly attributed to the stimulation of the host’s immune system caused by the bacterium. This results in a T helper type 1 (Th1) response and elevated levels of Th1 cytokines.9–11 As a consequence, products of the local immune reactions may migrate to extra-gastric sites and this may explain the link between H. pylori infection and a variety of extra-gastric diseases, including autoimmune disorders.12,13 However, epidemiological data exist that suggest a protective effect of H. pylori infection against the development of some diseases with an autoimmune component, such as asthma, most probably by H. pylori’s ability to induce immune tolerance and limit inflammatory responses.14,15 The mechanism underlying this protective role of H. pylori infection is thought to be differential expression of local mucosal inflammatory response, which may elicit a systemic release of cytokines, which in turn may downregulate systemic immune responses and suppress autoimmunity.
Triggered by the above, numerous studies have examined the association between H. pylori infection and IBD. However, the published literature is diverse. Thus, many studies have reported that the prevalence of H. pylori infection is lower in patients with IBD compared to controls, whereas this has not been confirmed by other studies. This prompted us to further investigate this association by performing a meta-analysis in which we pooled the results of all existing relevant studies.
Methods
Identification of studies and data extraction
We searched the PubMed, MEDLINE and Embase databases through September 2014 to identify all relevant English-language medical literature for human studies using the following key words or Medical Subject Headings (MeSH) terms: Helicobacter pylori AND (inflammatory bowel disease OR ulcerative colitis OR Crohn’s disease). In detail, the following search items were used: (“helicobacter pylori” (MeSH Terms) OR (“helicobacter” (All Fields) AND “pylori” (All Fields)) OR (“helicobacter pylori” (All Fields) OR (“h pylori” (All Fields)) AND ((“inflammatory bowel diseases” (MeSH Terms) OR (“inflammatory” (All Fields) AND “bowel” (All Fields) AND “diseases” (All Fields)) OR “inflammatory bowel diseases” (All Fields) OR (“inflammatory” (All Fields) AND “bowel” (All Fields) AND “disease” (All Fields)) OR “inflammatory bowel disease” (All Fields)) OR (“colitis, ulcerative” (MeSH Terms) OR (“colitis” (All Fields) AND “ulcerative” (All Fields)) OR “ulcerative colitis” (All Fields) OR (“ulcerative” (All Fields) AND “colitis” (All Fields)) OR (“crohn disease” (MeSH Terms) OR (“crohn” (All Fields) AND “disease” (All Fields)) OR “crohn disease” (All Fields) OR (“crohn’s” (All Fields) AND “disease” (All Fields)) OR “crohn’s disease” (All Fields)). In addition we performed a full manual search of all review articles and published editorials and retrieved original studies. Data were extracted independently from each study by two of the authors (T.R. and J.P.G) by using a predefined form, and disagreements were resolved by discussion with a third investigator and consensus. The work was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 16
Selection criteria
Inclusion and exclusion criteria were defined before the commencement of the literature search; thus, eligible studies were included in this meta-analysis if they met all the following criteria: (1) published as full article, (2) include data for retrieval on the association between H. pylori infection and IBD and (3) H. pylori infection was confirmed by serology and/or histology and/or urea breath test (UBT) and/or rapid urea test (RUT) and/or culture. Studies that did not meet the aforementioned criteria and duplicate publications were excluded. When two papers reported the same study, the publication that was more informative was selected.
Statistical analysis
The risk ratio (RR, 95 % confidence intervals (CIs)) was used to describe the ratio of the probability of the H. pylori infection occurring in IBD patients vs the controls. Thus in each study the RR of H. pylori infection in IBD patients vs controls was calculated and then pooled estimates were obtained using the fixed-model (Mantel and Haenszel) method, 17 unless significant heterogeneity was present or if the design of the studies was considered to be different enough, in which case the random-effects model was applied (DerSimonian and Laird method 18 ). Heterogeneity between studies was evaluated with the Cochran Q-test 19 and it was considered to be present if the Q-test provided a p value of less than 0.10. 20 In addition I2 statistic was used to measure the proportion of inconsistency in individual studies that could not be explained by chance, with I2 > 50% representing substantial heterogeneity. 21 We also performed a cumulative meta-analysis to examine whether the association between H. pylori and IBD changed over time. 22 Forest plots were constructed for visual display of individual study RR. Data, in various formats, i.e. as dichotomous (number of events) or computed effect sizes, were meta-analyzed by choosing the most suitable data entry option for the meta-analysis software used (Comprehensive Meta-Analysis, version 2; Biostat Inc, Englewood, NJ, USA).
Sensitivity analyses/publication bias
In the presence of significant statistical heterogeneity, apart from the random-effects model, we performed sensitivity analyses to evaluate the consistency of our results. Firstly, to evaluate any possible excessive influence of a single study, we examined whether the exclusion of this study substantially altered the magnitude or heterogeneity of the summary estimate. This was achieved by repeating the meta-analyses with exclusion of each individual study one at a time, to assess the overall effect of the exclusion on the pooled RRs. 22 Secondly, as different study designs and populations may incorporate different biases, we performed subgroup analyses, stratifying by factors that could potentially influence the results. These factors were established a priori to the analysis. Where needed, we further explored heterogeneity by performing meta-regression analyses (method of moments). 23 The likelihood of publication bias was assessed by constructing funnel plots, which were obtained by plotting the log RRs vs SE of individual studies. 24 Their symmetry was estimated by Egger’s regression test and the Begg and Mazumdar adjusted rank correlation test,25,26 whereas the adjustment for publication bias, i.e. calculation of the number of studies missing from the meta-analysis, was estimated using Duval and Tweedie’s nonparametric “trim and fill” rank-based method. 27
Results
Descriptive assessment and study characteristics
A flowchart describing the process of study selection is shown in Figure 1. Out of 468 titles initially generated by the literature searches, 33 studies, from various countries, remained eligible for meta-analysis.28–60 Some studies contained separate data on UC and CD and therefore in the 33 meta-analyzed studies there were in total 50 sets of data (22 on UC and 28 on CD) comparing H. pylori infection in patients and controls. The main characteristics of the papers eligible for meta-analysis are shown in Table 1. They were conducted in different parts of the world and contained a total of 4400 IBD patients and 4763 controls.
Flow diagram of the studies identified in this meta-analysis. The main characteristics of the included studies IBD: inflammatory bowel disease; IBS: irritable bowel syndrome; CD: Crohn’s disease; UC: ulcerative colitis; UBT: urea breath test; RUT: rapid urea test; UK: United Kingdom; US: United States.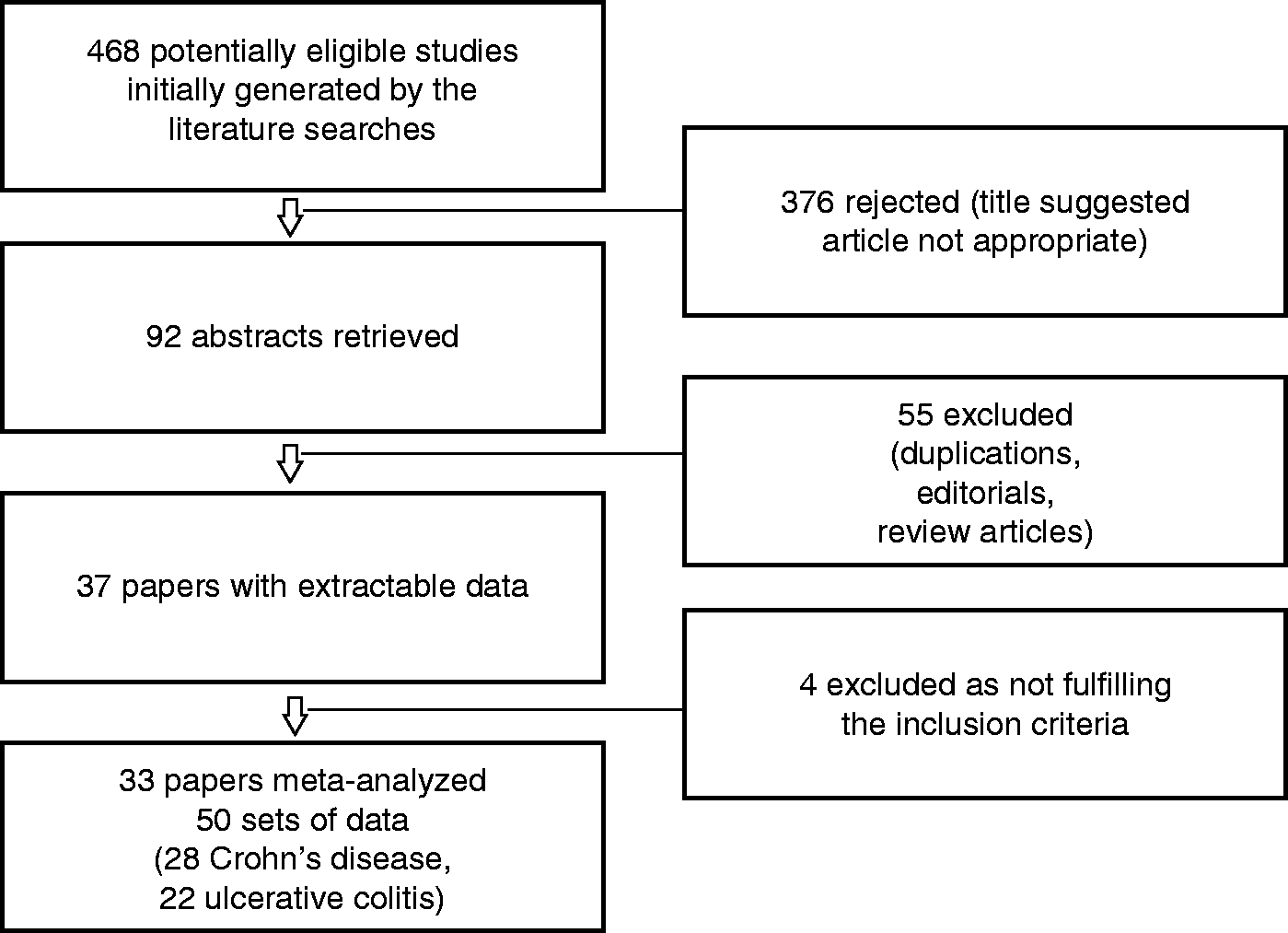

H. pylori prevalence in IBD patients vs controls
In the 33 eligible for meta-analysis studies, in the IBD group, overall 1168/4400 patients were positive for H. pylori infection (26.5%, 95% CI (25.2–27.8)), compared to 44.7% (43.3–46.1) of individuals in the control group (2129/4763). There was significant heterogeneity in the included studies (Q = 137.2, degree of freedom (df) (Q) = 32, I2 = 77%, p < 0.001) and therefore the random-effects model of meta-analysis was used. The obtained pool RR estimation was 0.62 (95% CI (0.55–0.71), test for overall effect Z = –7.04, p < 0.001)) (Figure 2(a)). There was no evidence of publication bias as judged by the construction of funnel plot and estimation of its symmetry (p = 0.15, by the Egger’s regression test) (Figure 2(b)).
(a) Forest plot showing individual and pooled RRs (95% CIs) in studies comparing Helicobacter pylori prevalence in IBD patients and controls. (b) Funnel plot of all studies included in the meta-analysis. RR: risk ratio; CI: confidence interval; IBD: inflammatory bowel disease.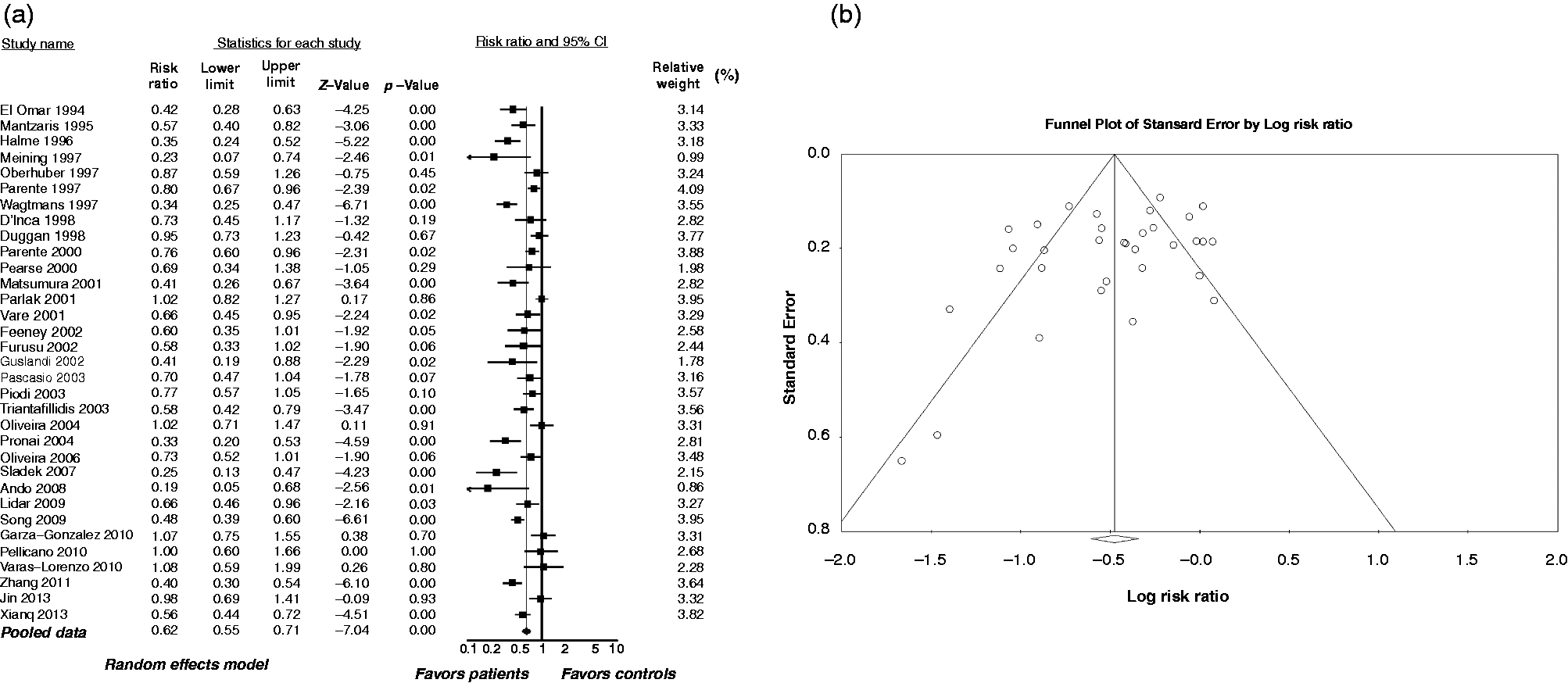
Subgroup analyses/sensitivity analyses
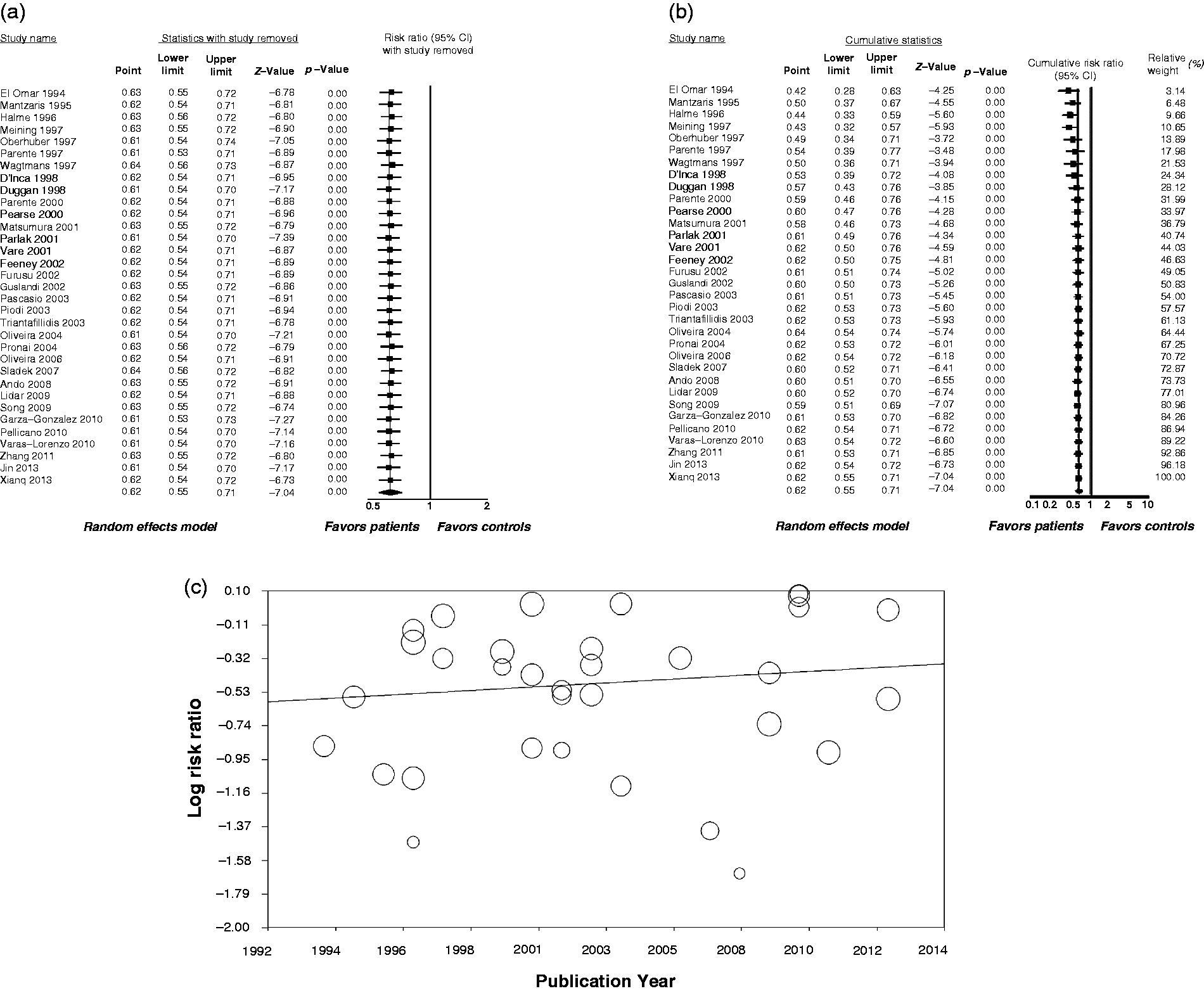
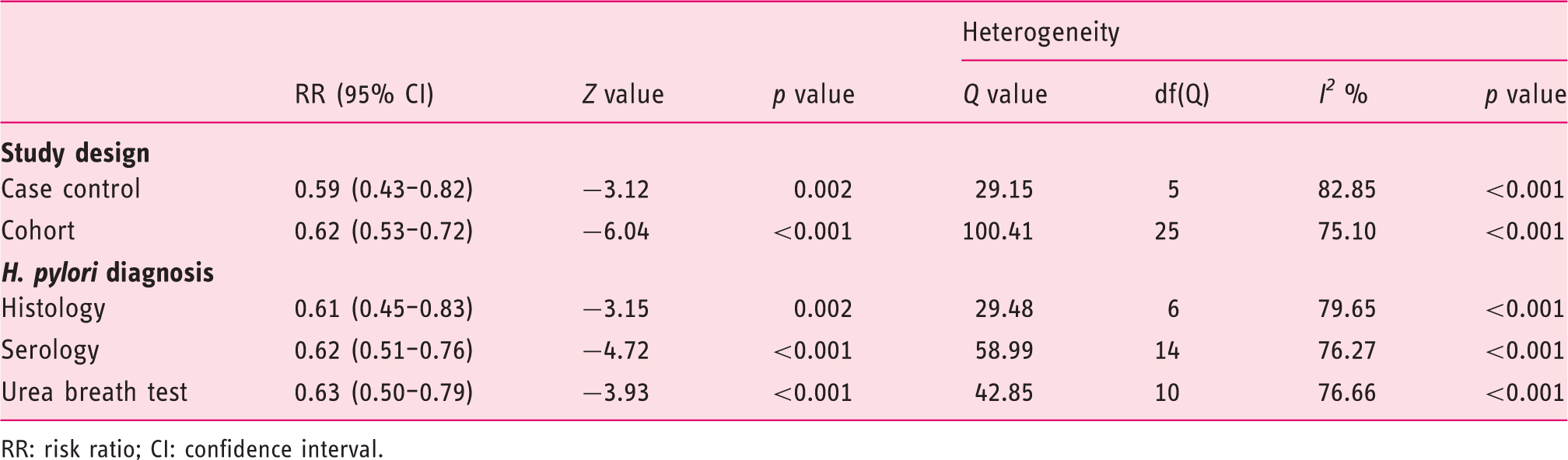
Due to significant heterogeneity, apart from using the random-effects model, subgroup analyses were performed. Thus, we grouped by stratifying for disease, i.e. meta-analyzing separately 28 sets of data for CD and 22 for UC (Figure 3). These subgroup analyses showed significant results for both diseases, with a trend toward a greater effect for CD (0.38 (0.31–0.47), Z = −8.98, p < 0.001) when compared to UC (0.53 (0.42–0.67), Z = −5.39, p < 0. 001). However, there was significant heterogeneity in the included studies for both diseases; CD: Q = 66.67, df (Q) = 27, I2 = 59.5%, p < 0.001 and UC: Q = 55.33, df (Q) = 21, I2 = 62%, p < 0.001. In an attempt to further explore the observed heterogeneity, we stratified data based on the study design (cohort vs case control) and H. pylori diagnosis (serology vs UBT vs histology) (Table 2). However, none of these subgroup analyses were able to account for the observed heterogeneity. As different study designs and populations may incorporate different biases, except for grouping for the aforementioned diseases, study design and method of H. pylori diagnosis, further sensitivity analyses were performed. Thus, exclusion of any study did not considerably alter the magnitude of the summary estimate (Figure 4(a)). In addition, the results of the cumulative meta-analysis of studies, ordered by the year of publication (Figure 4(b)), were consistent over the years. Finally, the meta-regression analysis evaluating the regression of publication year on log risk ratio, showed no significant results (z = −0.48, p = 0.63) (Figure 4(c)).
Forest plot showing individual and pooled RRs (95% CIs) in studies (grouped by disease, i.e. CD and UC) comparing the Helicobacter pylori prevalence in patients and controls. RR: risk ratio; CI: confidence interval; CD: Crohn’s disease; UC: ulcerative colitis. (a) Exclusion sensitivity plot showing the effect of exclusion of any study on the magnitude of the summary estimate. (b) Cumulative meta-analysis of studies ordered by year of publication. (c) Meta-regression analysis showing regression of publication year on log risk ratio. Circles represent each study in the meta-analysis, and the size of the circle is proportional to study weighting. Sub-group analyses by stratifying the data according to study design and method of Helicobacter pylori diagnosis RR: risk ratio; CI: confidence interval.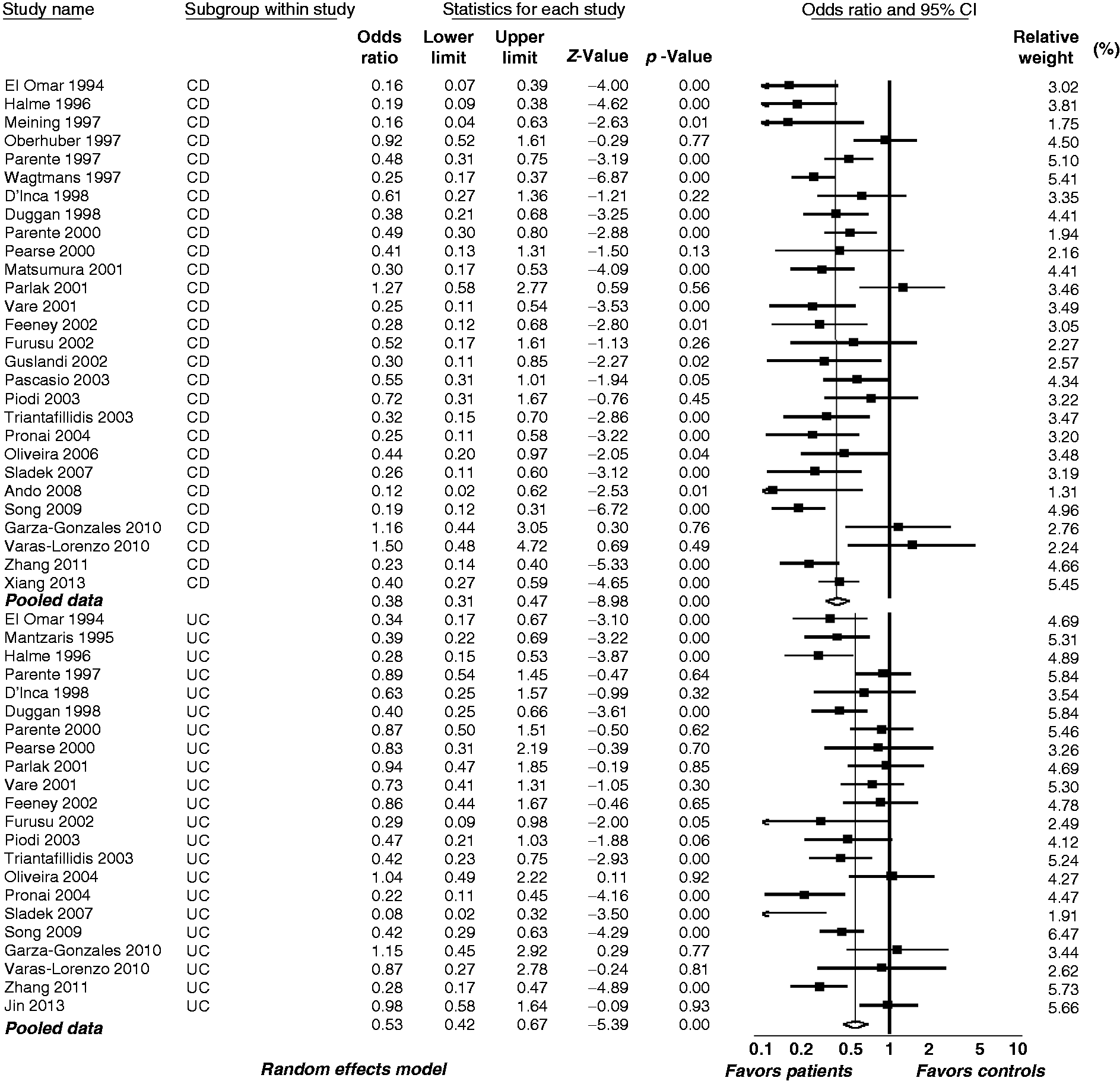
Discussion
H. pylori infection is acquired early in childhood and if not treated is carried throughout life. Epidemiological data show that IBD is more prevalent in areas with lower rates of H. pylori infection and suggest a possible protective effect of H. pylori infection against IBD and some diseases with an autoimmune component such as asthma.14,15,61 In parallel, there is a steady rise in the incidence of IBD in H. pylori endemic regions that may correspond to the beginning of anti-H. pylori therapy for peptic ulcer disease. 2
All the above piqued research interest and triggered numerous observational studies examining the relationship between H. pylori infection and IBD. This meta-analysis pooled all data from eligible relevant studies and showed a statistically significant inverse relationship between H. pylori infection and IBD (both CD and UC), which may suggest a possible protective effect of H. pylori against the development of IBD. These results confirmed an earlier study that pooled the data of studies published up to March 2009. 62 In addition our results are also in agreement with those of a recent large study 63 that examined whether the prevalence of H. pylori is lower among IBD patients compared with non-IBD individuals based on material from surgical pathology and concluded that these findings may open new avenues to study the pathogenesis of IBD.
In attempting to explain the negative association between H. pylori infection and IBD, the possibility that the treatment previously given against IBD is responsible for the lower prevalence of H. pylori infection in IBD patients remains a controversial subject. Thus, the aspect that treatment with drugs, such as sulfasalazine, could be responsible for H. pylori eradication and lower H. pylori prevalence in IBD patients has been raised by some authors. 28 However, others did not support this notion as treatment with sulfasalazine or any other medical therapy (i.e. 5-aminosalicylic acid (5-ASA), steroids, thiopurines, antibiotics) had no influence on H. pylori prevalence.30,36,44,54 Furthermore, it seems that even newer therapeutic modalities, such as anti-tumor necrosis factor (TNF) treatment, have no influence on H. pylori status in IBD patients. 64
Nonetheless, the notion that the immunomodulatory properties of H. pylori may confer protection against allergic and chronic inflammatory disorders has been addressed and recently reviewed.65,66 Toward this notion there is laboratory evidence illustrating H. pylori’s role in the regulation of the immune system. Thus, a proposed model of H. pylori’s effect on host immune regulation is that H. pylori, through its interaction with dendritic cells (DCs), is able to upregulate regulatory T-cells leading to decreased production of proinflammatory cytokines. In more detail, H. pylori has been associated with increased gastric mucosal expression of Foxp3 (a T-regulatory cell marker) altering the host immunologic response away from the inflammatory Th1/Th17 pathway.67–71 Furthermore, in mice evidence has emerged proving protective effects of H. pylori infection against Salmonella typhimurium-induced colitis. 72 Thus in co-infection with both bacteria, H. pylori suppressed Salmonella-specific Th17 responses in the cecum, reducing cecal inflammation. These protective effects were attributed to increased levels of interleukin (IL)-10 in the mesenteric lymph nodes of co-infected mice as opposed to Salmonella-only-infected mice, suggesting that this regulatory cytokine modulates the differentiation and/or activity of Th17 cells. In addition it is speculated that the protective effect of H. pylori on colitis may be associated with H. pylori’s chromosomal DNA, which in mice, through a high ratio of immunoregulatory to immunostimulatory sequences, is capable of preventing sodium dextran sulfate-induced experimental colitis. 73 Nonetheless it must be stressed that whether H. pylori DNA is indeed a relevant factor in the protection against IBD remains to be elucidated in more detail, since data showing protection by live bacterial infection in IBD models, other than acute Salmonella-induced colitis, are currently not available.
The consistency of the results over the years, as shown in the cumulative meta-analysis of studies ordered by the year of publication and the lack of publication bias, strengthens the results of this meta-analysis. However, despite the random-effects model used and the sensitivity analyses performed, the persisting significant heterogeneity found among the studies may call the results into question. An additional drawback is that the possible role of confounders, which could influence the results, was not adequately addressed in the studies involved. For example, low socioeconomic status could be a strong common confounder and perhaps the real cause for both the higher H. pylori prevalence and the lower IBD prevalence observed. In fact the prevalence of both may not be truly associated, and it should be stressed that epidemiological studies and meta-analyses based on epidemiological studies can only suggest associations, but not establish cause-effect relationships.
In the future, in order to overcome problems that may contribute to significant heterogeneity, relevant prospective studies should address all the related confounders, stratifying by factors that could potentially influence the results, such as the method of H. pylori diagnosis, method of IBD diagnosis, study origin and study population age. Ideally, controls who are age- and sex-matched to the IBD group should be selected from the same area as the IBD group, tested for H. pylori by the same method and in addition in both IBD and control groups previous H. pylori treatment should be taken into account. Most important, H. pylori testing should be conducted at the time of IBD diagnosis, i.e. in patients naïve for IBD treatment, which potentially could influence H. pylori status. Furthermore, in H. pylori-positive patients the presence of cagA should be considered, as it is claimed that the possible protective effects of H. pylori against other autoimmune diseases come from cagA-positive strains.74,75 The mechanism underlying the inverse association between cagA-positive H. pylori strains and the lower incidence of autoimmune disease has yet to be defined. However, it has been suggested that the intense host immune responses to cagA-positive H. pylori strains may further alter Th1- and Th2-type immune responses with subsequent induction of immunoregulatory lymphocytes. 74
In conclusion, the results of this meta-analysis support a protective effect of H. pylori infection against the development of IBD. However, the heterogeneity among studies may limit the value of these results. Therefore, further prospective studies examining the precise role of H. pylori and its eradication in the development of IBD may be necessary, taking into account the role of confounders such as environmental factors.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.