
Abstract
Introduction
Patients with inflammatory bowel disease suffer from various symptoms, impairing their quality of life and often affecting psychosocial issues. This may lead to the need for additional psychological care. This study investigated patients’ subjective need for integrated psychosomatic support and psychotherapy and indicators for it.
Materials and methods
This is a cross-sectional multicentre study in Austrian inflammatory bowel disease patients who were in routine care at 18 inflammatory bowel disease outpatient clinics. Patients filled in an anonymous, validated questionnaire (Assessment of the Demand for Additional Psychological Treatment Questionnaire, ADAPT) assessing the need for psychological care. The Assessment of the Demand for Additional Psychological Treatment Questionnaire gives two separate scores: the need for integrated psychosomatic support and for psychotherapy. In addition, health-related quality of life and the use of complementary and alternative medicine as well as clinical and sociodemographic variables were queried. Multivariable regression analysis was performed to estimate the effect of the previously mentioned variables on the need for additional psychological care.
Results
Of 1286 patients, 29.7% expressed a need for additional psychological care, 19.6% expressed a need for integrated psychosomatic support and 20.2% expressed a need for psychotherapy. In the multivariable analysis, the two strongest indicators for the need for both types of psychological care were the use of complementary and alternative medicine (for integrated psychosomatic support: odds ratio = 1.64, 95% confidence interval 1.13–2.39, p = 0.010; for psychotherapy: odds ratio = 1.74, 95% confidence interval 1.20–2.53, p = 0.004), and a low health-related quality of life score (for integrated psychosomatic support: odds ratio = 0.95, 95% confidence interval 0.94–0.96, p < 0.001; for psychotherapy: odds ratio = 0.96, 95% confidence interval 0.94–0.97, p < 0.001).
Discussion
About 30% of the Austrian inflammatory bowel disease patients expressed a need for integrated psychosomatic support and/or psychotherapy. The most important indicators for this need were the use of complementary and alternative medicine and low quality of life.
Key summary
What is already known?
Despite ongoing improvement of treatment options, patients may not respond to treatment or may develop side effects. Due to this burden of disease, patients may also suffer from psychological symptoms, such as depression. In our previous study in 2008, we found that 31% of patients with inflammatory bowel disease expressed a subjective need for psychological interventions.
What are the significant and/or new findings of the study?
Despite improvements in therapy, around 30% of patients with inflammatory bowel disease express a subjective need for psychological interventions. This subjective need for psychological interventions is associated with complementary and alternative medicine use and low quality of life.
Introduction
Inflammatory bowel diseases (IBD) are lifelong diseases that often cause impaired quality of life (QoL). 1 Patients suffer from various physical symptoms, such as abdominal pain, diarrhea and urgency of bowel movements, leading to significant restriction of daily life activities. Despite ongoing improvement of treatment options, patients may not respond to treatment or may develop side effects. Due to this burden of disease, its often unpredictable course, symptom-related embarrassment and concealment, patients may also suffer from psychological symptoms, such as anxiety, depression, stress and fatigue, which have a negative impact on their QoL. 2 These negative moods and major life events can influence the course of the disease. 3 Because of such high levels of psychological and emotional distress, many patients seek complementary and alternative therapies, as well as psychosomatic and psychotherapeutic treatment.4–6 A positive effect on the QoL has been reported, especially for psychotherapy and mind-body interventions. 5
In a previous study in 2008 we found that 31% of patients with IBD expressed a subjective need for psychological interventions in at least one of two dimensions, namely the need for integrated psychosomatic support and the need for psychotherapy. 6 This finding may have been influenced by the fact that these patients were followed at a tertiary centre where a specialist psychosomatic outpatient clinic was offered. Apart from this, improved clinical treatment options may have changed the outcome and therefore the psychological and emotional distress over the last decade as well. 7 Thus the present study aimed to investigate if (a) the subjective need for psychological interventions has changed over the last decade, (b) if the previous result can be generalized to a large multicentre cohort of Austrian IBD patients and (c) to elaborate factors associated with such a need.
Patients and methods
Study population and data collection
This is a part of a project of the Austrian IBD Study Group and was performed as a cross-sectional study with 18 participating Austrian outpatient clinics specializing in the treatment of patients with IBD. The main aim of the study was to examine the prevalence and indicators of complementary and alternative medicine (CAM) use among IBD patients. The present study is a sub-analysis of that project. Materials and methods have been described in detail previously in a manuscript on the use of CAM.8, 9 Briefly, consecutive adult patients over 18 years of age with an established diagnosis of IBD (based on clinical, endoscopic, histological and radiological criteria according to European Crohn’s and Colitis Organization (ECCO) guidelines)10, 11 attending specialized IBD outpatient clinics were included. Patients were asked to fill in an anonymous German-language questionnaire booklet that was handed out during routine outpatient visits and returned by the patient on the same day. Each patient could take part in this survey only once. Patients were recruited between May 2014 and July 2015. The study was approved by all responsible local ethics committees (Medical University of Vienna, 16 July 2014). Because the study was performed by using an anonymous questionnaire, no written informed consent was obtained from each patient. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution’s human research committee.
Part one of the questionnaire included questions concerning socio-demographic characteristics (age, gender, partnership, educational level, household income and residential area) and IBD-related data (disease subtype, disease duration, medical and surgical treatments and ever having perianal fistulas).12–15 Part two included the Short Inflammatory Bowel Disease Questionnaire (SIBDQ), the Assessment of the Demand for Additional Psychological Treatment Questionnaire (ADAPT) and the international questionnaire to measure use of CAM in German (ICAM-G) (see in the following).
The SIBDQ is a well-known validated 10-item questionnaire to assess health-related QoL.16–18 Its total score ranges from 10–70: 10 indicating the worst and 70 the best QoL. A score greater than 50 was considered as a good QoL. 19
The ADAPT assesses the need for additional psychological care as subjectively perceived by the patient.7, 20 It was developed by a multidisciplinary board including physicians, psychologists, patients and relatives in an iterative process primarily elaborating 12 items that are to be answered on visual analogue scales from 0–100 (see Appendix). It has proven construct validity, reliability and responsiveness. 7 Factor analysis finally revealed two distinct dimensions including 10 items concerning the need for psychological care: the need for integrated psychosomatic support (ADAPT-IPS) and the need for psychotherapy (ADAPT-PT). 20 Integrated psychosomatic support is intended as empathic counselling by physicians specializing in IBD with additional psychological training, which is integrated into clinical care and focuses on psychological and social issues of IBD patients. In contrast, psychotherapy was defined as solely psychological treatment in a psychotherapy office and setting. The ADAPT-IPS score is calculated as mean of the items 3–6, the ADAPT-PT score is calculated as the mean of items 7–12 (item 7 to be inverted, i.e., 100 – response to question seven). Both scales give values from 0–100, higher scores signifying a greater need. To indicate patients with a need, a cut-off of 70 in each dimension of the ADAPT questionnaire was calculated previously by taking the mean scores + 2 standard deviations of IBD patients who scored low on the hospital anxiety and depression scale.
The ICAM-G is a standardized, German-language questionnaire about CAM use in detail within the previous 12 months.21, 22 The ICAM questionnaire was developed to measure standardized CAM use and its German translation was validated and assessed. 22
Statistical analysis
Data analysis was performed using SAS version 9.4 software (SAS Institute Inc., Cary, NC, USA). Descriptive statistics such as frequencies, percentages, medians and interquartile ranges were used to describe each variable.
The variables ‘need for integrated psychosomatic support’ (ADAPT-IPS) and ‘need for psychotherapy’ (ADAPT-PT) were defined as the sum of items 3–6 and items 7–12 of the ADAPT questionnaire, respectively 20 and grouped by a cut-off of 70 points (<70 vs ≥70) into two binary variables standing for ‘no need’ and ‘need’ for psychological intervention.
Multivariable analysis was performed to elaborate independent associated factors for ADAPT-IPS and ADAPT-PT. Variable selection for multivariable analysis was based on previous research and literature. 23 The following variables were considered for multivariable analysis: gender, residential area grouped into four regions (‘West’ (Vorarlberg, Tyrol), ‘Middle’ (Salzburg, Upper Austria), ‘East’ (Vienna, Lower Austria, Burgenland), ‘South’ (Carinthia, Styria)), educational level (‘primary school, compulsory school’, ‘secondary-school graduates’, ‘secondary academic schools, university degree’), age at inclusion, CAM use within the previous 12 months, SIBDQ, medical treatment (steroids, immunosuppressants, biologics) and duration of disease.
The associations between the previously mentioned variables and the ‘need for integrated psychosomatic support’ and ‘need for psychotherapy’ were modelled by two logistic regression models in SAS. The effects of the variables are shown as odds ratios (OR) and corresponding 95% confidence intervals (CI). The significance level was set at 5%. The p values are to be interpreted exploratorily and have not been adjusted for multiple testing.
Results
Sociodemographic and clinical characteristics
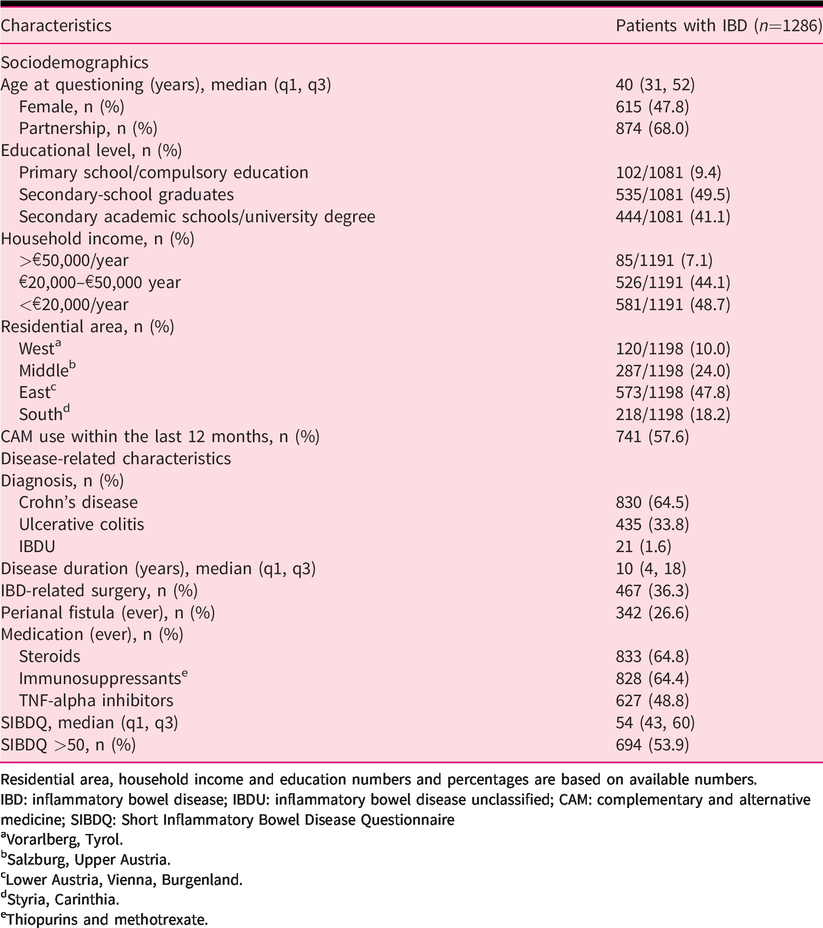
During the study period, 1338 out of 1605 IBD patients (return rate 83.4%) completed the questionnaire. A total of 52 patients did not specify their disease entity, so that 1286 patients remained for further analysis. Patient characteristics are summarized in detail in Table 1.
Sociodemographic and clinical characteristics of 1286 patients with IBD.
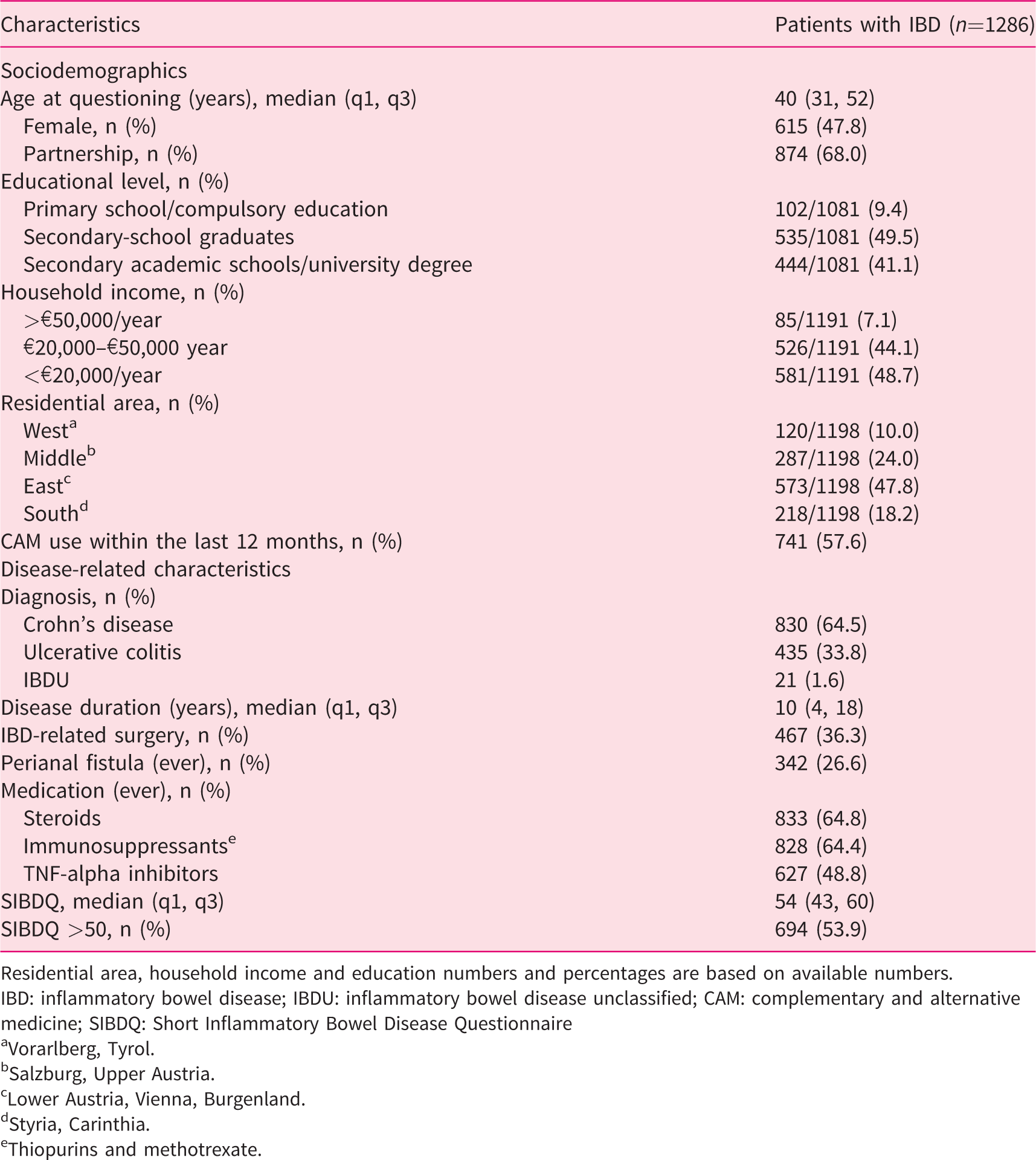
Residential area, household income and education numbers and percentages are based on available numbers.
IBD: inflammatory bowel disease; IBDU: inflammatory bowel disease unclassified; CAM: complementary and alternative medicine; SIBDQ: Short Inflammatory Bowel Disease Questionnaire
aVorarlberg, Tyrol.
bSalzburg, Upper Austria.
cLower Austria, Vienna, Burgenland.
dStyria, Carinthia.
eThiopurins and methotrexate.
The need for integrated psychosomatic support and psychotherapy in IBD patients
Complete responses to all questions in the ADAPT questionnaire were available for 1099 patients (85%). Of the 1099 patients, 326 (29.7%) expressed a need for additional psychological care as indicated by a score ≥70 in at least one of the two dimensions of the ADAPT questionnaire. Overall, 215 patients (19.6%) had an ADAPT-IPS score ≥70, 222 patients (20.2%) had an ADAPT-PT score ≥70 including 111 patients who had a score ≥ 70 in both dimensions (10.1%).
Table 2 shows the numerical median scores of the ADAPT-IPS and ADAPT-PT depending on sociodemographic and clinical variables.
Scores of the ADAPT-IPS and ADAPT PT in relation to sociodemographic and clinical variables (univariate analysis).
The results are given as median (Q1; Q3).
ADAPT: Assessment of the Demand for Additional Psychological Treatment Questionnaire; IPS: integrated psychosomatic support; PT: psychotherapy; CAM: complementary and alternative medicine; IBDU: unclassified inflammatory bowel disease; IBD: inflammatory bowel disease; SIBDQ: Short Inflammatory Bowel Disease Questionnaire.
aWest: Vorarlberg, Tyrol.
bMiddle: Salzburg, Upper Austria.
cEast: Lower Austria, Vienna.
dSouth: Styria, Carinthia.
The univariate analysis revealed several differences concerning the ADAPT-IPS and ADAPT-PT scores when the study population was categorized by sociodemographic and clinical variables (see Table 2). The largest differences in ADAPT-IPS scores were noticed between geographic Austrian residential areas, household income, CAM use in the preceding year, QoL as measured by the SIBDQ and age at diagnosis. The ADAPT-IPS score was also considerably higher among patients with unclassified IBD (IBDU) in comparison with Crohn's disease and ulcerative colitis; however, the number of patients with IBDU was very low.
The largest differences concerning ADAPT-PT scores were noticed with respect to educational level, age at questioning, gender, CAM use in the preceding year, QoL as measured by the SIBDQ, age at diagnosis and disease duration. Further differences were noticed with respect to steroid use and anti-TNF therapy.
Logistic regression models
The regression model for ADAPT-IPS revealed that the use of CAM within the last 12 months and reduced SIBDQ were strong and independent indicators for the need for integrated psychosomatic support (Table 3). The OR for CAM use was 1.64 (95% CI 1.13–2.39; p = 0.010) and for reduced SIBDQ 0.95 (95% CI 0.94–0.96; p < 0.001). Furthermore, age at inclusion was positively associated with the need for integrated psychosomatic support with an OR of 1.02 (95% CI 1.00–1.03; p = 0.046) for a 10-year increase in age.
Logistic regression models for indicators for the need for integrated psychosomatic support (ADAPT-IPS) and psychotherapy (ADAPT-PT) in patients with inflammatory bowel disease.
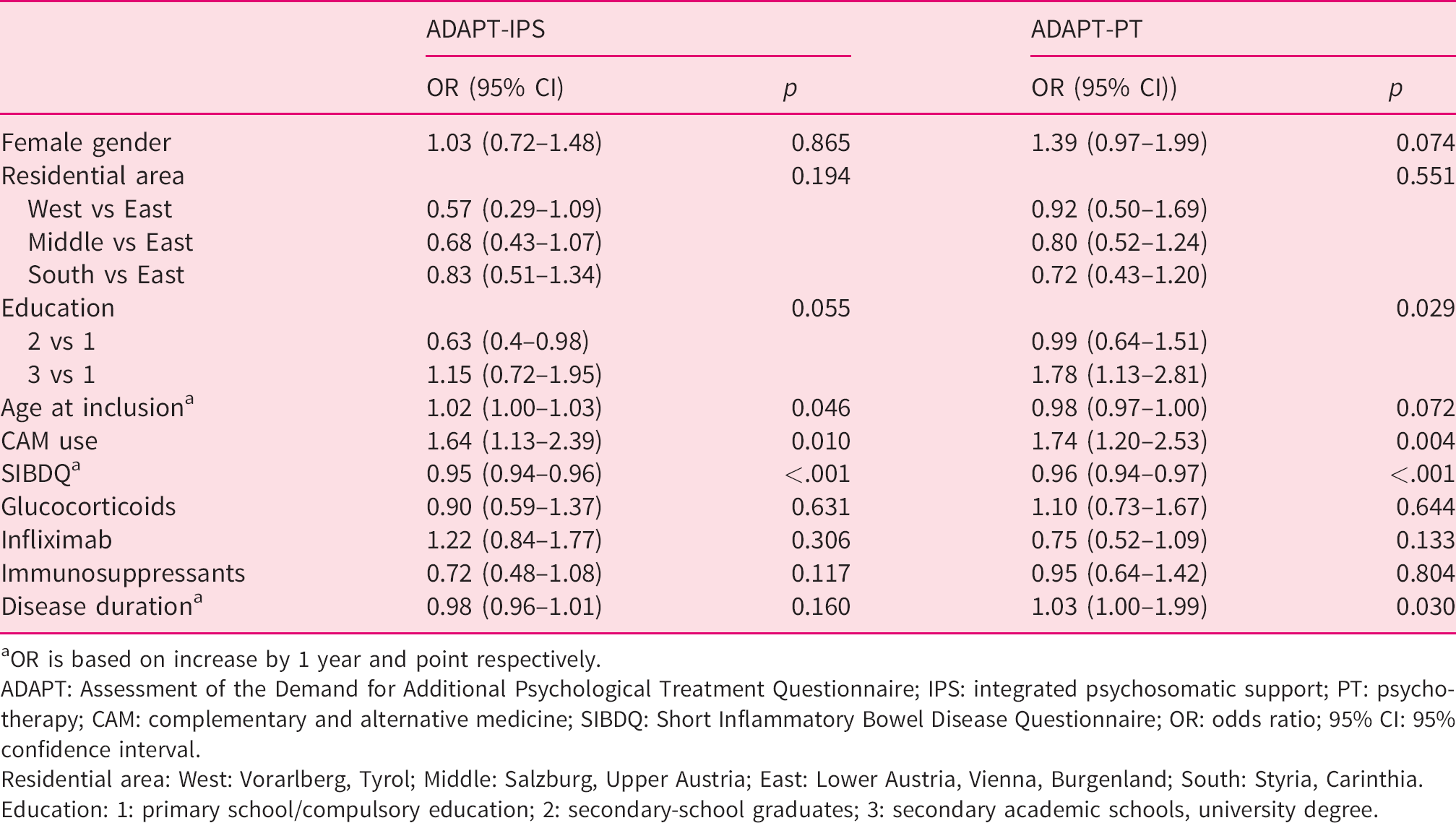
aOR is based on increase by 1 year and point respectively.
ADAPT: Assessment of the Demand for Additional Psychological Treatment Questionnaire; IPS: integrated psychosomatic support; PT: psychotherapy; CAM: complementary and alternative medicine; SIBDQ: Short Inflammatory Bowel Disease Questionnaire; OR: odds ratio; 95% CI: 95% confidence interval.
Residential area: West: Vorarlberg, Tyrol; Middle: Salzburg, Upper Austria; East: Lower Austria, Vienna, Burgenland; South: Styria, Carinthia.
Education: 1: primary school/compulsory education; 2: secondary-school graduates; 3: secondary academic schools, university degree.
The regression model for ADAPT-PT revealed that again both CAM use within the last 12 months (OR 1.74, 95% CI 1.20–2.53; p = 0.004) as well as reduced SIBDQ (OR 0.96, 95% CI 0.94–0.97; p < 0.001) were strong and independent indicators of the need for psychotherapy (Table 3). In addition, university education (OR 1.78, 95% CI 1.13–2.81; p = 0.029) as well as disease duration (based on increase by 1 year) (OR 1.03, 95% CI 1.00–1.99; p = 0.030) were also indicators of such a need.
Discussion
The present study revealed that almost a third of patients with IBD expressed a subjective need for additional psychological care. About 20% each of all patients expressed this need for IPS and PT, respectively.
This is in agreement with our previous study in 2008.6, 7 However, because patients in that study were recruited at one specialist IBD outpatient clinic of a tertiary university hospital we cast doubt on the generalizability of these data. The present study was designed as an anonymous multicentre study also including patients from IBD outpatient clinics outside university hospitals. Nevertheless, this study almost exactly equalled our previous results, where 31% of patients expressed a need for psychological care. Most recently, Klag et al. described a need for psychotherapy in 47% of patients, which is even higher than in our study. 24 However, in the latter study, which also used the ADAPT questionnaire, the cut-off to indicate a need was set at a lower threshold.
This is an interesting finding, because therapy has achieved significant improvement over the last decade with increasing use of effective biological and immunosuppressive therapies. 25 Early initiation of biological therapy has been shown to improve outcomes, 26 although there are conflicting data in this respect, too.27, 28 For example, the introduction of anti-TNF therapy has not always yielded the expected declines in intestinal resection rates. 29 This may in part have contributed to a delayed start of effective treatment and a negative selection of the worst patients. Because modern therapies have significantly improved patient management in general, one would therefore expect the psychological burden of IBD would also have decreased. Nevertheless, this does not seem to be the case and the need for psychological care seems to be constantly high. The question is why?
Psychological comorbidities such as anxiety and depression are common in IBD and have remained stable over recent decades despite progress in medical care.30,31 This may serve as one possible explanation why the need for psychological care has not changed. In the present study the logistic regression models revealed that the need for psychological care was mainly associated with use of CAM and low QoL, but not with the course of IBD, as indicated by immunosuppressive therapy. At least in young IBD patients, the relationship between low QoL and the prevalence of anxiety and depression has been clearly shown. 32 This was associated with negative illness perception especially for emotional representation. It therefore seems conceivable that a status such as a low QoL associated with negative illness perception, anxiety and depression would promote a subjective need to address this burden through a psychological approach.
Concerning the association between the use of CAM and the need for psychological care, the motives for the use of CAM may provide some explanation. These motives can mainly be divided into ‘pull factors’ such as holistic beliefs, natural medicine and positive experiences on the one hand and ‘push factors’ such as failed patient-doctor relationship, distrust and disappointment in conventional medicine on the other. 33 In particular, low satisfaction with patient-doctor interaction, length of visits and the specialists’ attitudes was shown to be associated with the use of CAM. 34 Thus the association between the need for psychological care and the use of CAM may be seen as the desire for a more dedicated and empathetic interaction between patient and doctor on an equal footing. Because doctors’ time is often limited, specialist nurses could help to close this gap and cover some of the need for an empathetic care to strengthen a reliable and robust relationship between the patient and the healthcare system in general.
There are some further aspects that are of interest with respect to the need for psychological care in IBD. One further explanation for this phenomenon may be related to coping. Depending on the coping style, coping with IBD may be associated with greater depression and functional disability, independent of symptom severity, which may promote the subjective need for additional psychological care. 35 Another possible explanation for the high need for psychological care in IBD may be provided by subjective attribution. Up to 59% of IBD patients assume a psychological background of IBD, which may possibly promote the IBD patient’s need to discuss this potential background. 2
The present study has several strengths and some weaknesses. One strength is the large number of patients and the multicentre design. This represents an important aspect, because patients were recruited from different levels of healthcare facilities from all Austrian regions, providing a high degree of generalizability. The second strength is the anonymity of the questionnaire, which gives a high likelihood of honest answers and unprettified results and may be a unique characteristic of this study as the usage of CAM is more likely to be hidden when talking to a physician. However, this might also be seen as a weakness, because the anonymity made it impossible to link self-reported data from the questionnaires with clinical data from chart review. In addition, queries to complete unanswered questions could not be made. This in turn did not allow us to include any clinical activity scores and therefore we had to rely on the SIBDQ score instead. Another weakness might be that patients were only recruited by specialized IBD physicians. We decided to recruit only these patients, due to the fact that specialized IBD physicians are the ones who are interested in conducting such a study. Nevertheless, our patients come from all over Austria and are not only treated in large tertiary centres, but also in secondary healthcare facilities and even in a doctor’s office itself.
For future studies, it could be extremely interesting to include a control group. In our first study back in 2008, we compared IBD with rheumatoid arthritis (RA). The study revealed that the subjective need for integrated psychosomatic support or psychotherapy was twice as high in IBD patients compared with RA patients. This difference was attributed to a different psychological status of IBD patients and not the diagnosis itself, as IBD patients seem to have a higher anxiety. 7
In conclusion, we found that patients with IBD have a high need for either integrated psychosomatic support, psychotherapy, or both. This need seems to be constant over recent decades despite the efforts of improving therapies. Our finding of a high need can be generalized due to a multicentre population and is mainly associated with a low QoL and use of CAM. For future resource allocation, this finding should be considered to meet the patients’ needs with the aim of reducing the burden of IBD and improving targeted healthcare use.
Supplemental Material
sj-pdf-1-ueg-10.1177_2050640620946874 - Supplemental material for Use of complementary and alternative medicine and low quality of life associate with the need for psychological and psychotherapeutic interventions in inflammatory bowel disease
Supplemental material, sj-pdf-1-ueg-10.1177_2050640620946874 for Use of complementary and alternative medicine and low quality of life associate with the need for psychological and psychotherapeutic interventions in inflammatory bowel disease by Maximilian Kutschera, Thomas Waldhör, Hans Peter Gröchenig, Thomas Haas, Heimo Wenzl, Pius Steiner, Robert Koch, Thomas Feichtenschlager, Gerald Eckhardt, Andreas Mayer, Andreas Kirchgatterer, Othmar Ludwiczek, Reingard Platzer, Pavol Papay, Johanna Gartner, Harry Fuchssteiner, Paul-Gerhard Peters, Gerhard Reicht, Gabriele Moser, Clemens Dejaco, Harald Vogelsang, Christian Primas, Gottfried Novacek and Wolfgang Miehsler in United European Gastroenterology Journal
Footnotes
Author contributions
MK, TW, GN and WM made substantial contributions to the conception and design of the study. HPG, GN, TH, HW, PS, RK, TF, GE, AM, AK, OL, RP, PP, JG, HF, PGP, GR, CP and HV made substantial contributions to recruitment. MK, GN, WM, CD and TW made substantial contributions to the acquisition, analysis and interpretation of data. MK, TW, GN, and WM drafted the manuscript and all authors have critiqued and revised it. All authors approved the submission.
Acknowledgements
Special thanks to Dr Corina Güthlin from the Johann Wolfgang Goethe University/Frankfurt am Main for providing us with the German version of the ICAM questionnaire. The manuscript was linguistically reviewed by David Westacott. Use of the Short Inflammatory Bowel Disease Questionnaire, written by Dr Jan Irvine et. al., was made under licence from McMaster University, Hamilton, Canada.
Ethics approval
The study was approved by all responsible local ethics committees. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution’s human research committee.
Conference presentation
This work was presented in part as a poster at the ECCO Congress, February 2020.
Informed consent
The patients were informed about the study and were asked to fill in the questionaire voluntarily. A written informed consent was not applicable since the questionnaire was anonymous.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Thomas Haas has served as a speaker/consultant/advisory board member for Abbvie, MSD, Takeda, Janssen, Atro Pharma and Sandoz. Andreas Mayer served as a speaker/consultant/advisory board member for Abbvie, MSD, Takeda, Astro Pharma, Janssen. Pius Steiner has served as a speaker/consultant/advisory board member for Abbvie, MSD, Janssen, Pfizer and Falk. Harry Fuchssteiner has served as a speaker/consultant/advisory board member for Abbvie, MSD, Takeda, Janssen and Astro Pharma. Gerald Eckhardt has served as a speaker/consultant/advisory board member for Abbie, MSD, Takeda, Janssen and Astro Pharma. Gerhard Reicht has served as a speaker/consultant/advisory board member for Abbvie, MSD, Takeda, Janssen and Astro Pharma. Pavol Papay has served as a speaker/consultant/advisory board member for Abbvie, MSD, Takeda, Pfizer, Janssen and Dr. Falk Pharma. Johanna Gartner has served as advisory board member for Merck/Janssen. Reingard Platzer has served as a speaker/consultant/advisory board member for Abbvie, MSD, Takeda, Janssen and Astro Pharma. Robert Koch has served as a speaker/consultant/advisory board member for Abbvie, Astro Pharma, Hospira, Janssen, Merck, MSD, Pfizer, Sandoz and Takeda. Thomas Feichtenschlager has served as a speaker/consultant/advisory board member for Abbvie, MSD, Takeda, Pfizer and Janssen. Paul-Gerhard Peters has served as a speaker/consultant/advisory board member for Abbvie, MSD, Takeda, Pfizer, Janssen and Roche Pharma. Gabriele Moser has been on the advisory boards of Allergan and Almirall, she has received grants to the Medical University of Vienna by Abbvie, Vifor, Almirall, Merck, Falk, Bayer, Yakult, Sanova, Danone, Emonta and Montavit and she has been on the speakers bureaus for Falk, Peri Consulting, Henrich Communication, Milton Erickson Institut Austria, Wirtschaftskammer Austria and Gebro. Clemens Dejaco has served as a speaker/consultant/advisory board member for Abbvie, Astro Pharma, Bayer, Falk Pharma GmbH, Janssen, MSD, Pfizer, Takeda and Vifor. Christian Primas has served as a speaker/consultant/advisory board member for Abbvie, SD, Takeda, Janssen, Merck, Ferring, Astro Pharma. Harald Vogelsang has received a consultant and/or lecture fee from Abbvie, Amgen, Astro, Bristol-Myers Squibb, Falk, Ferring, Gilead, Janssen, MSD, Pfizer and Takeda. Gottfried Novacek has served as a speaker/consultant/advisory board member for Abbvie, MSD, Takeda, Janssen, Sandoz, Pfizer, Astro Pharma, Falk Pharma GmbH, Ferring and Vifor. Wolfgang Miehsler has served as a speaker/consultant/advisory board member for Abbvie, MSD, Takeda, Janssen, Sandoz, Falk Pharma GmbH and Ferring. The other authors have no conflicts of interest to declare.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.