
Abstract
Background
Non-adherence to medication in patients with inflammatory bowel disease (IBD) is a challenging problem which is often overlooked or under-estimated by the physician or denied by the patient. We aimed to examine if re-phrasing the wording of the question used by the physician could help in revealing more patients who are non-adherent, and for whom appropriate counseling may be instituted.
Methods
A cross-sectional questionnaire-based study of IBD patients treated in a tertiary center was conducted. Patients received a questionnaire detailing their treatments and disease course, as well as their perceptions about disease. Two forms of questions about adherence were deliberately placed in two separate parts of the questionnaire: One was ‘are you taking your medications regularly as prescribed?’ (Standard question), and the second, more emphatic question, was ‘how often does it happen that you miss a drug dosing?’ (Re-phrased question). The rate of non-adherence disclosed by each of these questions was compared. Sensitivity, specificity and predicative values were computed for each question against the conventional definition of non-adherence as taking of less than 80% of prescribed medication doses disclosed by any of the methods. Predictors of non-compliance and of denying non-compliance were also explored.
Results
Overall, 165 patients were included (49% female, mean age 33.7 ± 12.7 SD, median age 30 years, 29.6% with ulcerative colitis, 62.4% with Crohn’s disease). Upon questioning, 50 (30.3%) of the patients admitted to non-adherence in the last month when asked by the emphatic re-phrased question format, compared with only 10 patients (6%) reporting non-adherence when asked directly by the standard question (OR 7.4, 95%CI 3.6–15.2, p < 0.001). Thus, a ‘Do you take your medicine regularly’ question format disclosed only 20% of genuinely non-compliant patients and had 16% sensitivity and 98.2% specificity for revealing non-adherence (PPV 80%, NPV 72.9%) compared with the reference re-phrased question. The leading cause for non-adherence was skepticism about drug efficacy or safety (20.5%), followed by vacation or weekend (15%), problems with prescription or pharmacy (13.5%) and forgetfulness (10%). No single demographic or clinical factor correlated with non-adherence. The only factor which correlated with higher probability for non-adherence was biological and combination treatment.
Conclusion
Non-compliance with treatment is much more common than patients admit. Asking patients how often does it happen that they miss a drug dosing is a simple, practical tool which performs significantly better in disclosing non-adherence compared with asking patients if they take their medication as they should.
Introduction
“Compliance”, “adherence”, “persistence” and “concordance” are terms related to the sub-optimal taking of medicine by patients. The term “adherence” is now more commonly used, as it represents a more positive attitude and interpretation of patient behavior.1,2
Adherence is defined as the extent to which patients are able to follow the recommendations for prescribed treatments. Patients may use more or less than the prescribed treatment or use their medication at the wrong time.1,3
Non-adherence with medication is a challenging problem with multiple causes related to the medication, to the patient and/or to the physician. Regardless of the reason, non-adherence has been shown to result in increased morbidity and mortality in several disease states, as well as increased health care costs.4–6
Inflammatory bowel disease (IBD) is a chronic condition with no clear etiogenesis and therefore with no definite curative treatment. Hence, chronic medical therapy is the cornerstone in controlling symptoms and achieving remission. On the other hand, IBD represents a high-risk situation for non-adherence owing to its chronicity and relapsing and remitting nature. Therapeutic relationship, as well as individual clinical and psycho-social characteristics influence adherence to medication.7,8 Data from IBD studies showed that non-adherent adults are more likely to experience a disease flare than their adherent counterparts. 2 Given the pervasive nature of non-adherence in IBD, population assessment and intervention are critical.2,6–14
Previous studies assessing overall adherence to treatment among patients with IBD reported variable non-adherence rates ranging between 7% and 72%, with most studies reporting that 30–45% of patients were non-adherent.14,15 However, the optimal means for assessing non-adherence are as yet undefined. Diverse tools and questionnaires have been developed with the aim of accurate assessment of non-adherence,16–19 but the agreement between these questionnaires is often imperfect. Moreover, their applicability in daily practice is questionable in the setting of a busy IBD clinic, where physicians may often resort to a simple single question of “are you taking the drugs as prescribed” or similarly phrased inquiry. Thus, there is dire need for simple measures to increase the accuracy of non-adherence assessment, in a manner applicable for the clinician in daily practice.
Therefore, we aimed to examine if simple re-phrasing of the wording of the question used by the physician could help in revealing more patients who are non-adherent, for whom appropriate counseling may be instituted. Secondary aims were to characterize factors predictive of treatment non-adherence and predictive of its denial.
Methods
Data acquisition
This was a cross-sectional questionnaire-based study of IBD out-patients treated in a tertiary center. All patients gave an informed consent and the study was approved by the institutional ethics committee.
All participants received a questionnaire inquiring about prescribed treatments and adherence, medication, doses, schedules, demographic information, disease behavior, duration and severity, and beliefs and standpoints regarding medication, disease and treatment.
Two forms of questions about adherence were deliberately placed in two separate parts of the questionnaire, so as to reduce potential carry-on effect. One was “are you taking your medications regularly as prescribed?” (Standard question), and the second, more emphatic, question was “how often does it happen that you miss a drug dosing?” (Re-phrased question). The rate of non-adherence disclosed by the standard question was compared with the rate disclosed by the re-phrased question. Non-adherence was conventionally defined as taking less than 80% of prescribed medication doses, 20 disclosed by follow-up questions after either of the two screening questions modes, and this rate was a priori defined as the reference for computation of sensitivity, specificity and positive and negative predictive values (PPV, NPV). For biologics, we defined a skipped infusion and/or a delay in receiving an intravenous infusion of over 7 days as a missed dose.21–23 For sub-cutaneous biologics, a skipped injection and/or delay of over 3 days in injecting the drug was considered as a missed dosing. 21 Predictors of non-compliance and of denying non-compliance were additionally explored by analyzing the association of co-variants with non-compliant behavior. The questionnaire underwent content validated by three additional IBD experts.
Statistical analysis
Variables were analyzed using student t-test for continuous variables and chi square test for categorical variables. Odds ratio and 95% confidence intervals (CI) were computed for all variables compared. Variables that were found to be statistically different on uni-variable analysis with a p-value ≤0.1 were incorporated into the multivariable analysis using a backwards logistic regression model. All statistics were performed using MedCalc software (version 12.2.1.0, Mariakerke, Belgium). A two-tailed p < 0.05 was considered statistically significant.
Results
Rates of non-adherence
Patients Characteristics.
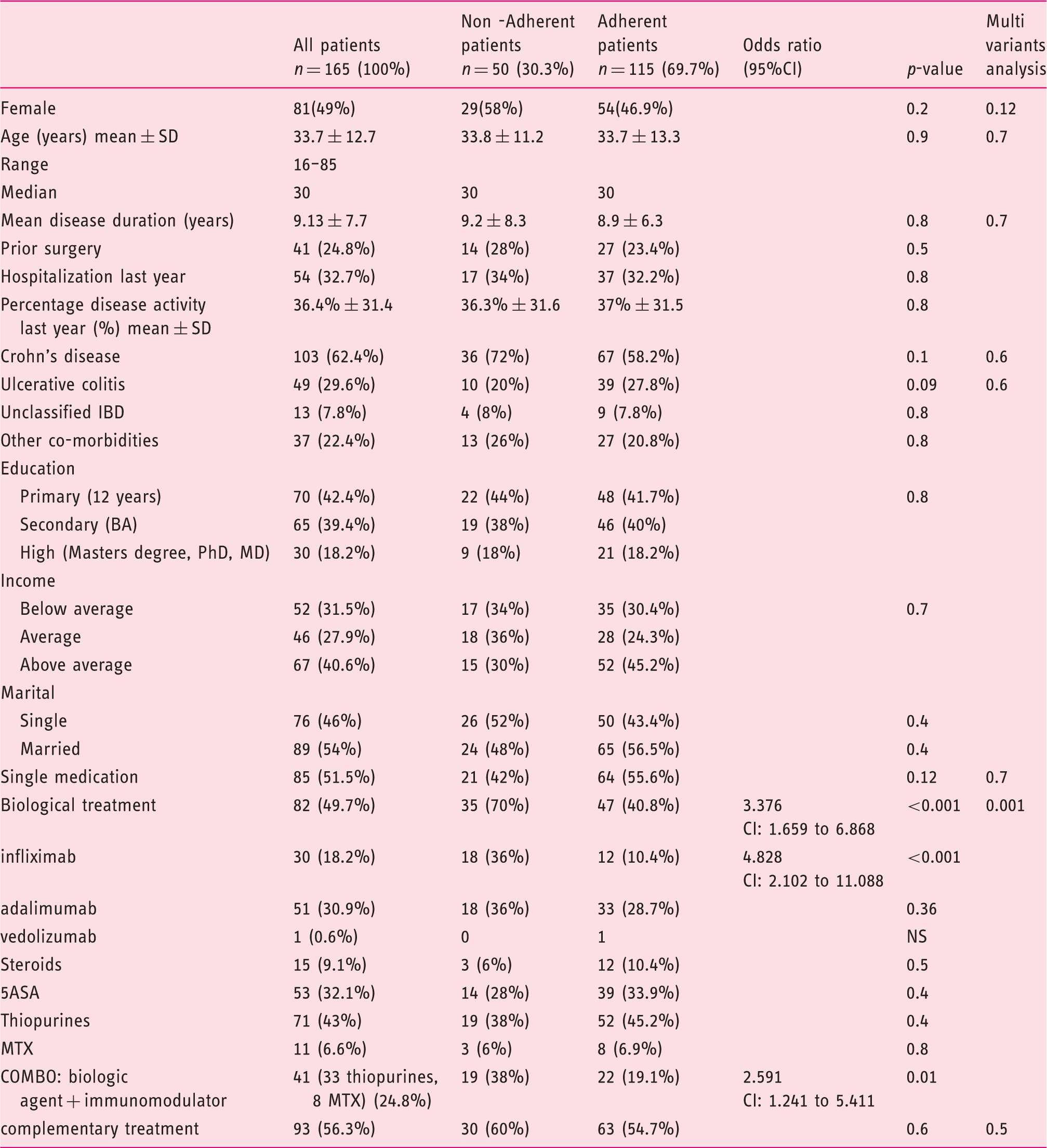
Upon questioning, 96 of the patients (58.18%) admitted to non-adherence in the last month when asked by the emphatic re-phrased question format. Of these, 50 (30.3%) were actually not adherent, that is, taking less than 80% of drug dosing revealed by answers to subsequent questioning. This rate was significantly higher compared with only 10 patients (6%) admitting to non-adherence when asked directly by the standard question (OR 7.4, 95%CI 3.6–15.2, p < 0.001). Upon computation, the question: “Do you take your medicine regularly” was found to disclose merely 20% of genuinely non-compliant patients, and had only 16% sensitivity and 98.2% specificity for revealing non-adherence (PPV 80%, NPV 72.9%) compared with 100% sensitivity and 60% specificity for the re-phrased question wording (PPV 52.8% NPV 100%).
Non-adherence was found to be present in patients taking the entire spectrum of drugs. In particular, out of 82 patients receiving biologic agents (infliximab, adalimumab, vedolizumab), 35 (42.6%) were found non-adherent. Interestingly, non-adherence rates with infliximab were higher than with adalimumab (66% and 29.4%, respectively, p < 0.001). Non-adherence rate for thiopurines was 26.7% and for 5-ASA 26.4%.
Causes of non-adherence
Main reasons for non-adherence.
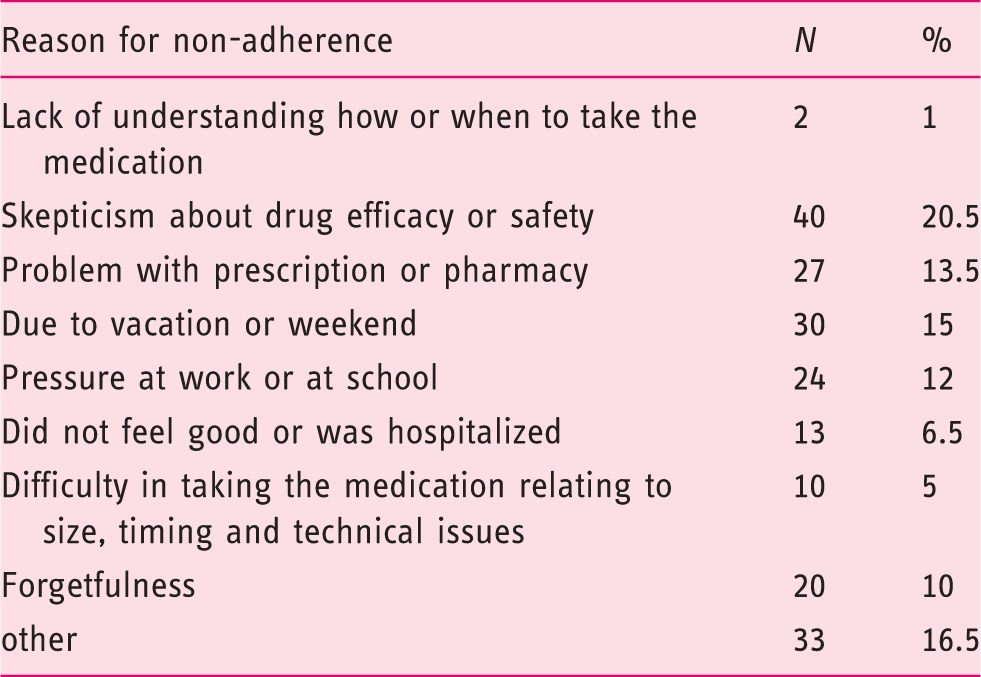
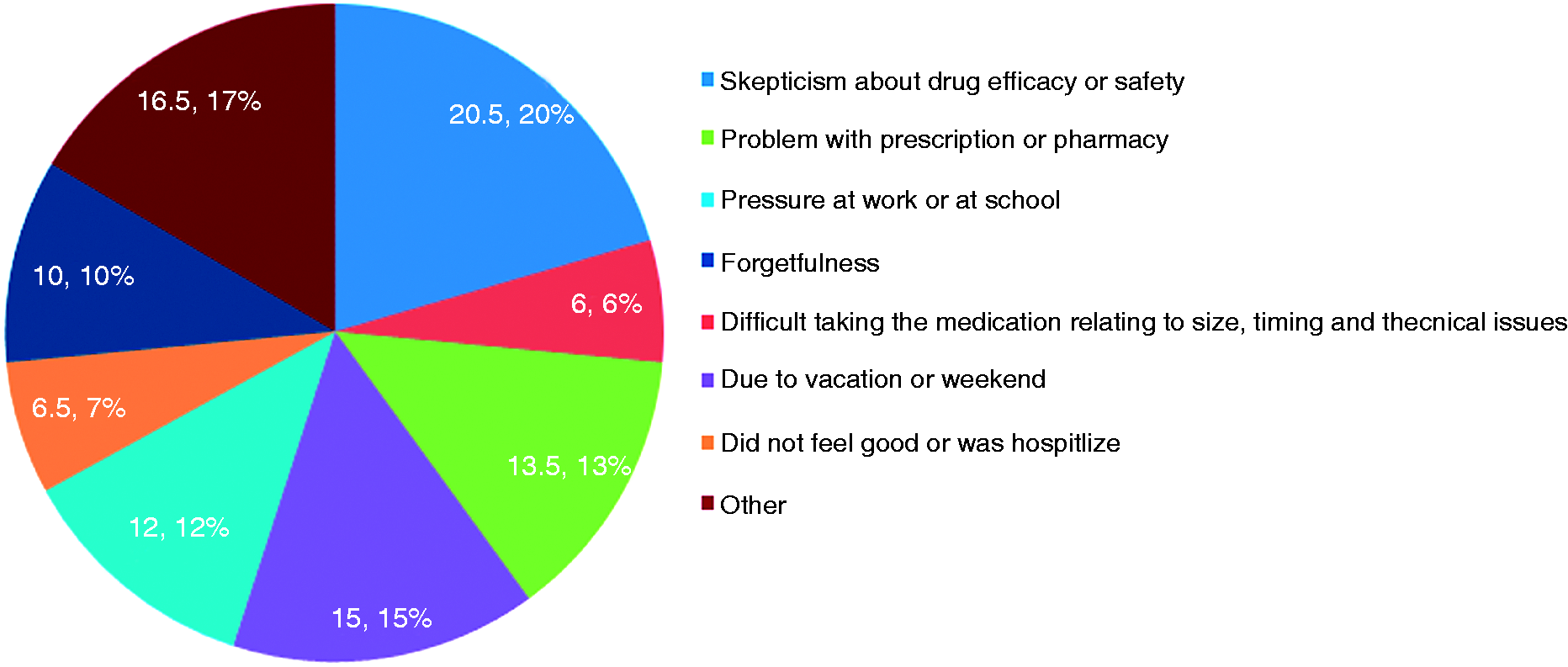
Causes for non-adherence.
We found that more than half of the patients, 93(56.3%) tried complementary medical treatments, 30(32.2%) of whom were non-adherent with the conventional treatment. Complementary medical treatment was not associated with tendency for non-adherence. A non-adherent patient was as likely to receive complementary treatment/s as adherent patients. The most common complementary treatments used were acupuncture, goat and camel milk and turmeric (curcumin). No other single demographic factor correlated with non-adherence behavior.
The only factor that correlated with higher probability of non-adherence was the use of biological therapy or combination biologic-immunomodulator treatment, with an odds ratio of 4.8 (Table 1).
Predictors of denying non-adherence
We finally attempted to analyze the sub-group of non-adherent denier patients (n = 42, the group who denied non-adherence by the standard question but disclosed non-adherence when inquired by the re-phrased question). Interestingly, patients whose reason for non-adherence was skepticism about drug efficacy or side-effects tended to conceal their non-adherence behavior in response to the standard question to a higher degree than patients with other reasons for non-adherence (14/42 (33%) versus 6/42 (14.2%), respectively, p = 0.045 OR 3.0 CI 95%). No other specific factors or demographic characteristics correlated with this behavior except biologic treatment. Non-adherent denier patients were more likely to be treated with biologic agent (88% vs. 36.5%, p < 0.0001 OR 12.8 CI 95%).
Discussion
Non-adherence to treatment is known to be under-estimated and often deliberately concealed by patients from their doctors. Similar to previous studies, we found high rates of non-adherence among IBD patients, rates which were increased by using an emphatic questioning format.
There are multiple tools and questionnaires for assessing non-adherence to medications.16–18 None of these has been established as gold standard for assessing non-adherence, and agreement between these different tools remains an area of debate.16,19 Moreover, most of these questionnaires remain useful predominantly as research tools, since their time-consuming nature precludes them from being employed in daily practice in an IBD clinic. 18 Thus, physicians inquiring about patients’ adherence may often do so by a single question, commonly in the form of “Are you taking your medications as prescribed?” or some variation thereof. We hypothesized that this common phrasing of the question may put patients in a more defensive state of mind which may be less permissive for volunteering the true scope of non-adherence. Based on our clinical experience, we further hypothesized that re-phrasing the question as “How often does it occur to you that you miss a drug dosing?” may be perceived to be more lenient and emphatic, thereby increasing the inclination to truthfully disclose data on non-adherence. Indeed, we found that the re-phrased question resulted in significantly higher odds for disclosing non-adherence compared with the standard question. We deliberately avoided employing a standardized adherence questionnaire, reasoning that none of these tools was decisively shown to be the gold standard for disclosing the accurate magnitude of non-adherence. Thus, our aim was to merely compare the rate of non-adherence disclosed by two simple, practical and short questions that can be readily used in the clinical settings. As such, our results showed that “How often does it happen that you missed a drug dosing?” was a question that performed much better than the standard question. Since no third tool was used, it is impossible to know the true sensitivity and specificity of the emphatic question. However, we did compare these two questions with the non-adherence rate as conventionally defined by less than 80% intake of medications, 20 and disclosed by follow-up queries after either of these two question formats, thereby increasing the internal validity of the findings. This analysis showed a much higher sensitivity of the re-phrased question compared with the standard conventional question, making it preferable as a practical screening question phrasing to be used by physicians for disclosing non-adherence among their IBD patients. Following this screening question, a positive response can then be further explored and confirmed by additional questioning or diagnostic tools. Numerous varying factors have been suggested to be associated with non-adherence in IBD patients, but no specific demographic factors correlating with non-adherent behavior were found.6–8,11–16
Younger age and employment status were statistically significantly associated with non-adherence in multiple studies. 16 Higher education level and younger age were associated with non-adherence in another study. 10 Another recent study showed that non-adherence was more frequent in young females followed-up by general practitioners and no difference was found with respect to educational status or type of IBD. 11 In another study, adherence was significantly higher among non-smoking patients. Adverse drug effects strongly contributed to non-adherence.10–13 However, a comprehensive review concluded that demographic, clinical and treatment variables were not consistently associated with non-adherence, as opposed to psychological distress, patients’ beliefs about medications, and doctor–patient discordance, which were associated with non-adherence. 14
Our results are congruent with these later observations as we could not identify education, age, socio-economic status or other demographics to be associated with non-adherence. The only factor which correlated with higher probability of non-adherence was biological and/or combination treatment. Interestingly, we found that skepticism about treatment efficacy or safety was the leading cause for non-adherence in our study. Strikingly, we found that “skeptical” patients were significantly more likely to “hide” non-adherence behavior from their physician (as gauged by a “deceptive” negative answer to a direct first question about adherence to therapy).
To the best of our knowledge, this is the first time a correlation has been shown between a specific individual’s belief and/or judgment of the treatment and his/her tendency to conceal non-adherence from the treating physician. If corroborated, this finding may prove useful for physicians in directing efforts for better education of patients regarding treatment efficacy and safety, as well as for more diligent monitoring of adherence in at-risk patient sub-groups.
Forgetfulness was also a major and common reason for non-adherence in our study, similar to findings in several previous studies.12,13 A study in a cohort of IBD patients found that 43% of patients occasionally forget to take their medication; however, only 7.5% of them did it voluntary. This raises the need for effective methods to assist in medication routine and methods to simplify prescription and pharmacy–patient–physician interaction.
Oral azathioprine was the drug with the poorest compliance in previous studies, with non-adherence rates reaching 25% of the total prescribed doses. Similar rates were found in our study, but in our study biologic drugs had the poorest compliance rate. This is reminiscent of findings of a recent retrospective study which reported that fewer than one-third of patients remained adherent to their scheduled maintenance infliximab regimen, as opposed to previous reports.12,17,21
Several limitations of our study should be acknowledged, including the modest size of the cohort and the fact that we relied solely on self-reported questionnaires along with the absence of a gold standard for medication adherence. Our study strengths are the diversity of patients from real-life experience, with almost 100% data acquisition from all patients.
In conclusion, non-adherence to medication is a common problem shared by all groups of patients and is more common than patients admit. Patients who are skeptical about the safety and/or efficacy of their prescribed medication are particularly likely to conceal non-adherence upon questioning.
Asking patients how many times they happen to miss medication is a simple pragmatic tool which performs significantly better as a practical clinical screening tool for disclosing non-adherence, as compared with asking patients if they take their medication as they should. Further studies are needed to develop short, practical and accurate tools for evaluating non-adherence in daily clinical practice.
Footnotes
Acknowledgements
TE participated in designing the study and in data acquisition, data analysis and manuscript drafting. SBH conceived the study, participated in data interpretation and in critical revision of the manuscript. TE, GB and NL participated in data acquisition and analysis. RE participated in data interpretation and in critical revision of the manuscript.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.