
Abstract
Background
Probe-based confocal laser endomicroscopy (pCLE) provides microscopic imaging during an endoscopic procedure. Its introduction as a standard modality in gastroenterology has brought significant progress in management strategies, affecting many aspects of clinical care and requiring standardisation of practice and training.
Objective
This study aimed to provide guidance on the standardisation of its practice and training in Barrett’s oesophagus, biliary strictures, colorectal lesions and inflammatory bowel diseases.
Methods
Initial statements were developed by five group leaders, based on the available clinical evidence. These statements were then voted and edited by the 26 participants, using a modified Delphi approach. After two rounds of votes, statements were validated if the threshold of agreement was higher than 75%.
Results
Twenty-six experts participated and, among a total of 77 statements, 61 were adopted (79%) and 16 were rejected (21%). The adoption of each statement was justified by the grade of evidence.
Conclusion
pCLE should be used to enhance the diagnostic arsenal in the evaluation of these indications, by providing microscopic information which improves the diagnostic performance of the physician. In order actually to implement this technology in the clinical routine, and to ensure good practice, standardised initial and continuing institutional training programmes should be established.
Keywords
Introduction
Confocal laser endomicroscopy (CLE) has emerged in the past 10 years, with the aim to overcome the inherent limitations of endoscopic sampling techniques and to provide both the endoscopist and the pathologist with a wider diagnostic arsenal, the ultimate goal being to rationalise and optimise subsequent patient management.
Two CLE systems have been developed: an endoscope-integrated system and a probe-based system. The endoscope-integrated confocal laser endomicroscopy system (eCLE) was developed first by Optiscan and integrated into a specific endoscope (EC3870K; Pentax, Tokyo, Japan). In this case, the confocal imaging module is integrated into the tip of a high-resolution endoscope. Although several important proof-of-concept studies have been published using eCLE, this system is no longer commercially available. The probe-based confocal laser endomicroscopy (pCLE) system has been developed by Mauna Kea Technologies (Cellvizio®; Mauna Kea Technologies, Paris, France). This technology uses a separate unit outside the endoscope, which emits the laser required for the imaging (laser scanning unit or LSU). The laser is directed to the mucosa through a bundle of optical fibres in a small probe (Confocal Miniprobe). The tip of this miniprobe consists of a set of lenses enabling the confocal imaging with the appropriate depth and resolution. This miniprobe can be introduced through the working channel of any endoscope, including the latest high-definition (HD) scopes, to visualise the tissue at a microscopic level at the same time as the macroscopic imaging. Depending on the organ and on the indication, several miniprobes are available, with different specifications to address the needs of each endoscopic procedure (field of view, depth of imaging and lateral resolution). Both of these endomicroscopy technologies provide microscopic cellular imaging with different properties. While eCLE provides a resolution of 0.8 microns and variable depth of focus between 0 and 250 microns, pCLE provides a resolution of up to 1 micron. Each confocal miniprobe has an appropriate static imaging depth. However, pCLE provides a faster video-rate scanning of 12 images per seconds, while eCLE can generate only one image per second. Confocal miniprobes are compatible with any endoscope, including cholangioscopes, and can be inserted into various accessories, as catheters during endoscopic retrograde cholangiopancreatography (ERCP) and needles for the assessment of solid or cystic lesions during endoscopic ultrasound-guided fine needle aspiration (EUS-FNA).
The introduction of CLE as a standard modality in gastroenterology has brought significant progress in management strategies, affecting many aspects of clinical care and requiring the standardisation of practice and training. The technology appears in the American Society for Gastrointestinal Endoscopy (ASGE) guideline, addressing the role of endoscopy in the evaluation and treatment of patients with biliary neoplasia. 1 This guideline mentions CLE as a useful tool in differentiating benign from malignant biliary strictures.
With the implementation of physician payment in the United States (US) and ongoing coverage efforts, standardisation of training modalities and subsequent practice in a ‘routine care’ setting is essential. In 2012, in the US, specific reimbursement (current procedural terminology (CPT)) codes were created for the use of CLE in upper gastrointestinal (GI) endoscopy applications and facility payment was determined. Physician payment was defined more recently through the established process of the Relative value scale Update Committee of the American Medical Association (AMA RUC), based on the evaluation of the relative value unit to reflect the cognitive efforts corresponding to the procedure. It turns out that CLE is associated with one of the highest relative value units in interventional endoscopy.
This document reports the suggested roles and uses of pCLE for the evaluation and treatment of GI lesions by endoscopists, from a consensus of experts. It aims to provide guidance to pCLE users and to other interested parties on the standardization of practice and to suggest recommendations on training and credentialing. These recommendations will evolve with the development of further clinical evidence and with technical evolutions.
Methods
A modified Delphi process was used to develop the consensus statements. This method consists of successive voting steps, during which each participant gives his or her opinion on each statement, independent of the other panellists.
For each topic, a group leader was responsible for drafting the initial versions of the statements, taking into account the corresponding available clinical evidence. All other invited participants comprised a group of advanced CLE users. All the participants had to fulfil the following three criteria: (i) use pCLE in their endoscopy unit for at least two years prior to participation in the consensus process; (ii) have published or communicated in international meetings on CLE applications; (iii) agree to review literature, at least in one segment of expertise (i.e. BE, biliary…) and participate in the voting process. After each step of voting, the group leaders reviewed the statements and edited them, before a new round of voting, until the consensus was achieved. The method is summarised in Figure 1 and detailed thereafter.
Methodology workflow.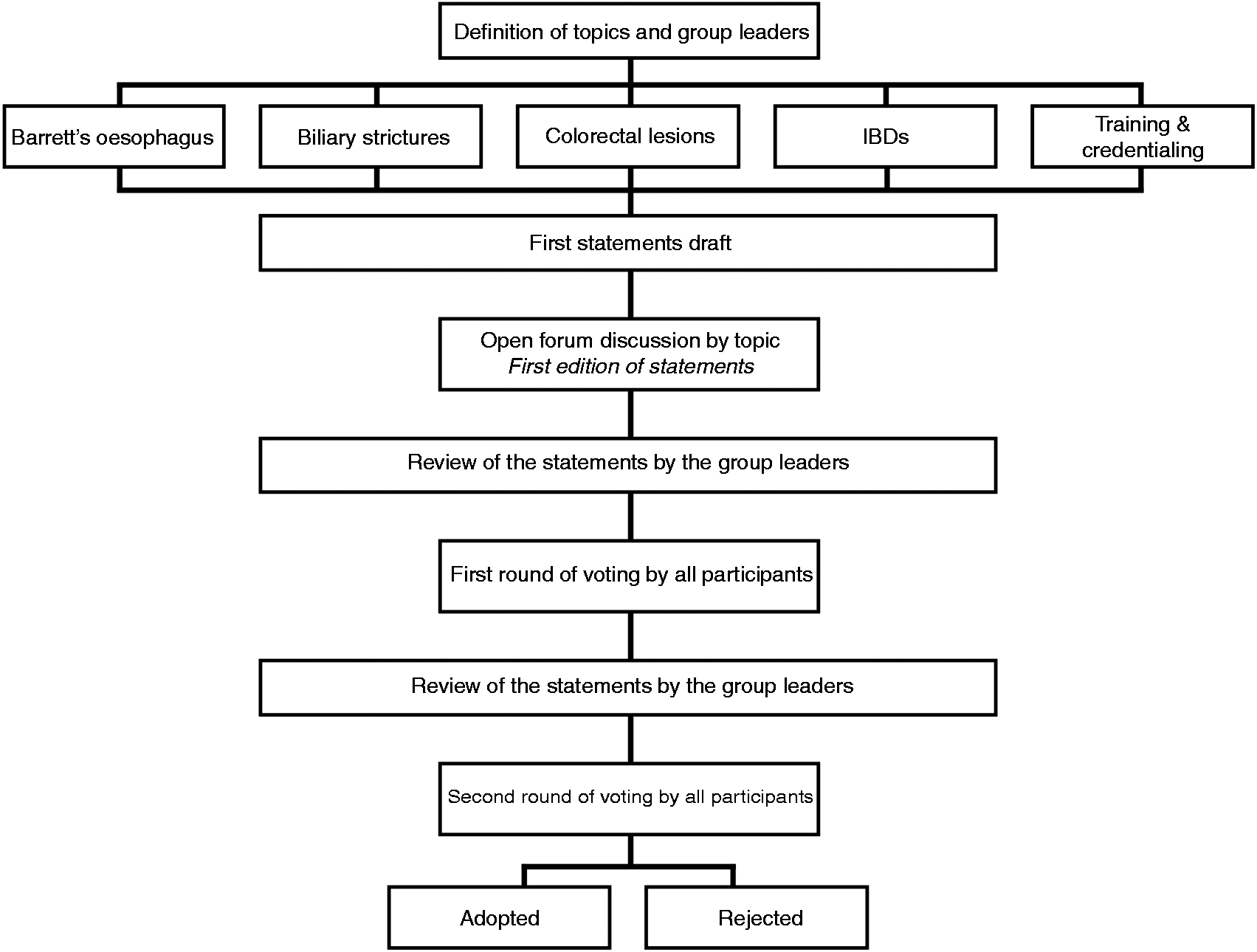
General design of the study
Four indications were chosen for evaluation in the consensus report: Barrett’s oesophagus (BE) (group leader: KKW), biliary strictures (group leader: DCL), colorectal lesions (group leader: SKS) and inflammatory bowel diseases (IBD) (group leader: HN). Those topics were selected based on the available clinical evidence and the reported potential impact of CLE on patient management. As for most new imaging technologies, the implementation of standardised training and credentialing programmes is crucial to optimise the use of this technique and to ensure safe, relevant and efficient practice. Accordingly, training and credentialing was assessed as the fifth topic in this consensus report (group leader: HB). However, as this last consensus was not based on clinical evidence grading, these statements have been reported as an appendix.
Classifications used in the voting process
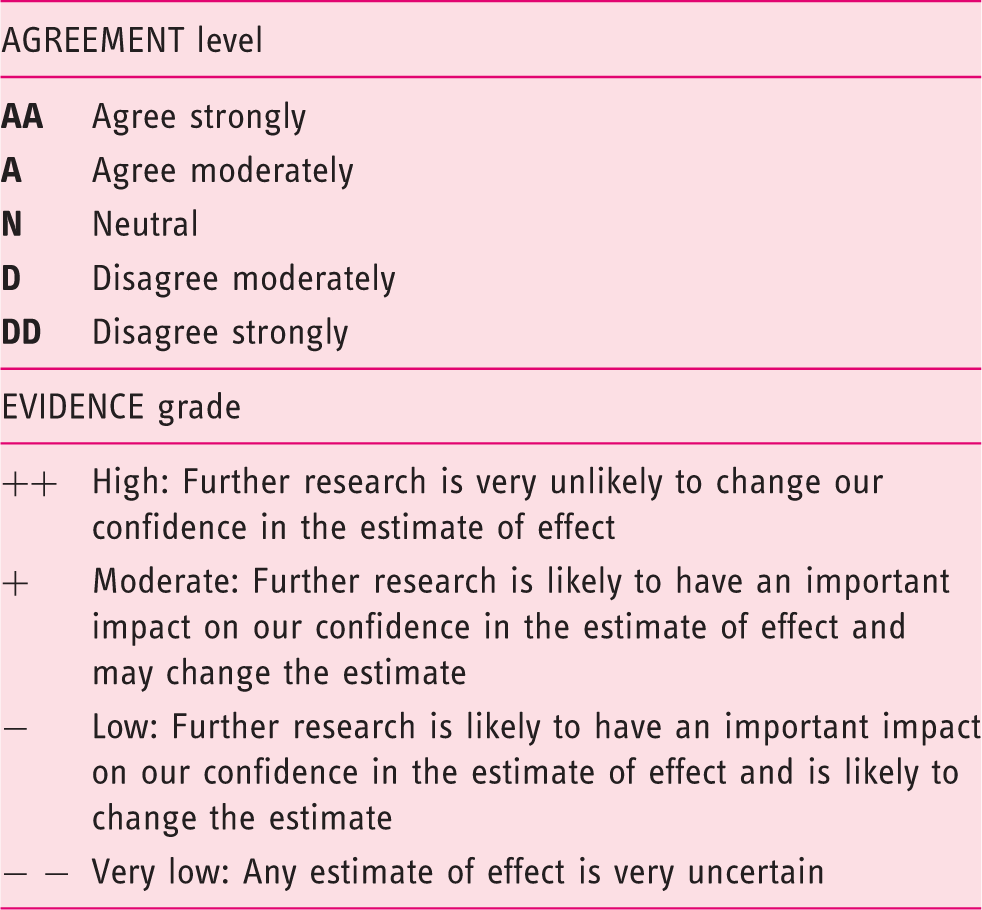
Assessment of the opinion and level of evidence
At the beginning of the consensus process, both techniques of CLE (i.e. eCLE and pCLE) were commercially available and the generic term ‘CLE’ was used for the development of statements and during the successive voting steps. However, at the time this article was written, eCLE was no longer commercially available and, following the editor’s request, the authors focused their manuscript mainly on pCLE (i.e. the only method available in practice). Nevertheless, important proof-of-concept studies or trials performed with eCLE were quoted anytime the authors considered these results as relevant for practice, especially for IBD. In this report, the generic term CLE was kept for the description of the statements as well as for generic terms, while comments rather refer to the specific technique used in original works, either pCLE or eCLE.
With respect to the literature review itself, different sources were used, including PubMed and Web research. As this report is based on the current level of evidence and practice, the authors chose not to ignore unpublished data such as communications presented during congresses, especially when abstracts were available (mainly on pCLE). The group leaders suggested a first list of references, and during the vote sessions, all 26 participants had the possibility to suggest and highlight new references to be included in the report.
Statistical analysis
Voting results were collected and divided into two groups. A statement was adopted if at least 75% of the votes agreed strongly or moderately, regardless of the grade of evidence. In all other cases, the statements were rejected.
Results
Overall results
Among the 26 experts, 20 experts expressed their opinion on BE, 16 on biliary strictures, 16 on colorectal lesions, eight on IBD and 22 on training and credentialing. Among a total of 77 statements, 61 were adopted (79%) and 16 were rejected (21%). The level of agreement and the grade of evidence for each statement are reported in Figure 2.
Diagrammatic representation of the concordance between the level of agreement and the grade of evidence, as estimated by experts (r represents the Spearman’s rank correlation coefficient).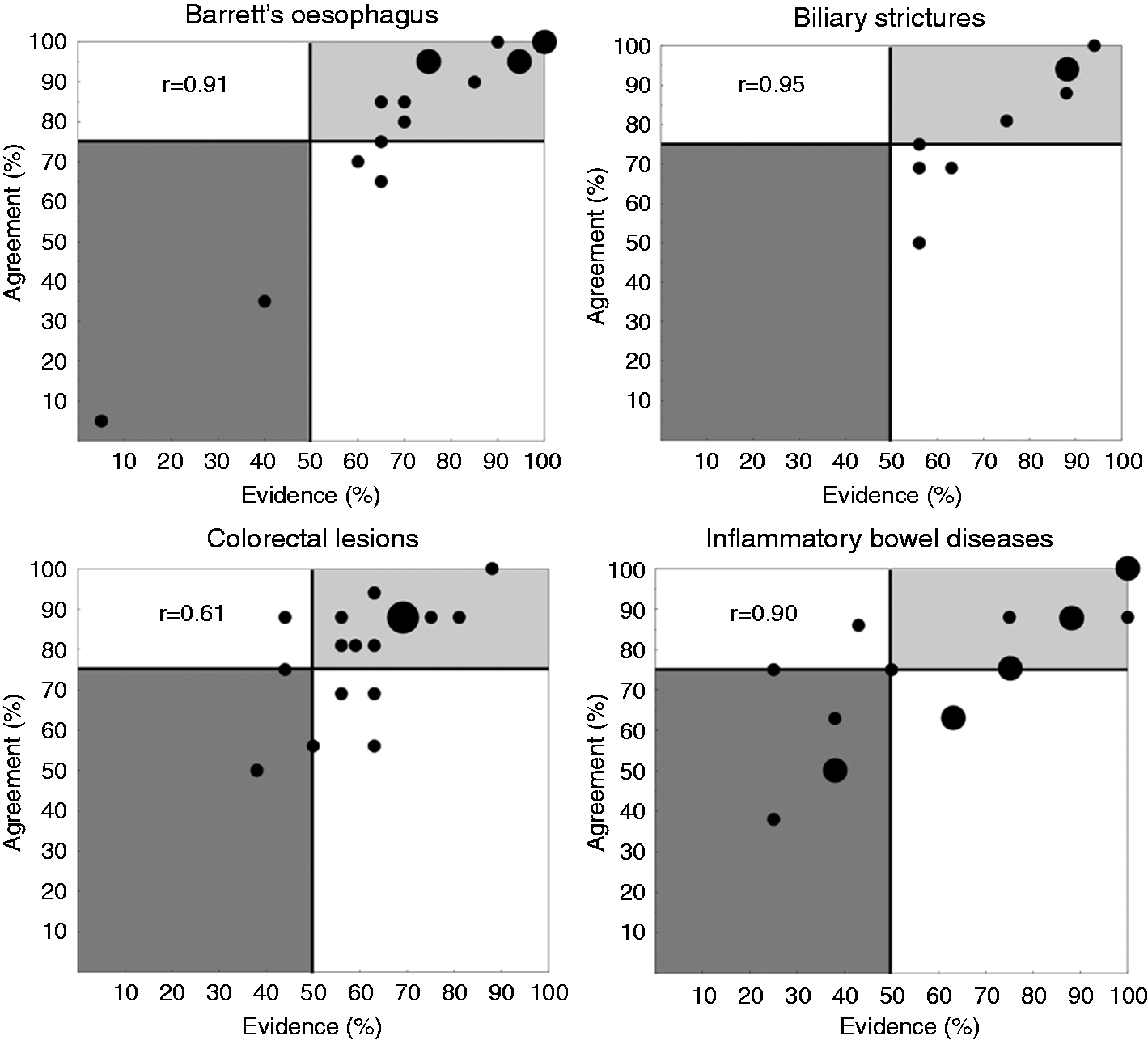
Barrett’s oesophagus
Available background knowledge
Diagnostic value of pCLE for the detection of neoplasia in BE (per patient analysis)
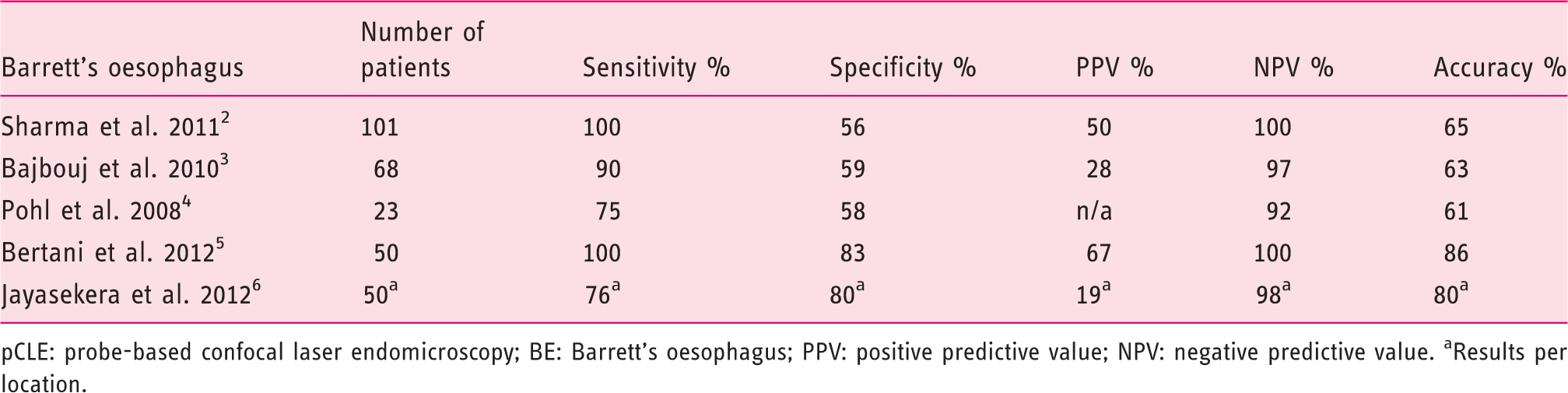
pCLE: probe-based confocal laser endomicroscopy; BE: Barrett’s oesophagus; PPV: positive predictive value; NPV: negative predictive value. aResults per location.
Results by statement
Twelve statements were adopted and four were rejected.
- Evidence: ++: 45%, +: 50%, –: 0%, – –: 5%
The use of CLE as a complementary tool during the endoscopic evaluation of BE was strongly supported by the panellists. The diagnostic value of CLE in BE has been assessed extensively during the last decade. Most studies reported quite similar results in terms of sensitivity, specificity and predictive values (Table 2). The specific clinical value of pCLE for the mapping of BE and the orientation of subsequent treatments has been established definitively by the DONT BIOPCE clinical trial. 2 In this study, 101 patients were followed-up after BE detection, and pCLE detected neoplasia with a sensitivity of 100%, a specificity of 56%, a positive predictive value (PPV) of 50% and a negative predictive value (NPV) of 100% per patient. The creation of upper GI level 1 CPT codes in the US relies largely on these data.
- Evidence: ++: 40%, +: 35%, −: 25%, – –: 0%
The patchy and inhomogeneous distribution of intraepithelial neoplasia within a BE segment makes it difficult to establish a correct diagnosis. Red-flag techniques are often used to delineate areas of interest. The use of CLE was strongly recommended by the panellists to collect microscopic information, for a better characterization of the mucosa with a high accuracy. Indeed, Sharma et al. 2 demonstrated that pCLE increased the sensitivity of white light endoscopy (WLE) and narrow band imaging (NBI) alone by 1.7 (45% vs. 75.8%, respectively, per location) and improved the PPV by 15%.
- Evidence: ++: 20%, +: 55%, –: 25%, – –: 0%
The use of CLE along with electronic enhancement was recommended by the panellists, as pCLE may further improve the identification of lesions and, specifically, of the margins. 2 Although adopted, this statement was supported by limited published data. Most studies did not report the use of electronic enhancement.
- EVIDENCE: ++: 35%, +: 55%, –: 10%, – –: 0%
The use of CLE to help to relocate the lesions of interest, and to prevent a new therapeutic procedure by acting directly during the first referral procedure, was recommended unanimously by the panellists. In cases where patients are referred from another institution or are scheduled for a repeat endoscopic session, CLE has been shown to facilitate the relocalisation of previously identified lesions and to allow for an immediate endoscopic treatment if necessary.7,8
- Evidence: ++: 35%, +: 30%, –: 35%, – –: 0%
Short-segment BE is difficult to identify and the presence of goblet cells is usually considered as a distinction between cardia and intestinal metaplasia. Image interpretation criteria have been developed to selectively identify cardia from intestinal metaplasia. Kiesslich et al. 9 reported the following classification to identify cardia: gastric-type epithelium includes capillaries with a regular shape visible only in the deeper parts of the mucosal layer and regular columnar-lined epithelium with round glandular openings and typical cobblestone appearance. Although the majority of the panellists supported the statement, they considered that the level of evidence was not sufficient and further studies were deemed necessary to demonstrate this.
- Evidence: ++: 70%, +: 30%, –: 0%, – –: 0%
According to the definition of BE, the presence of intestinal metaplasia is often considered as a diagnostic criterion. A consensus based mainly on the Miami Classification
10
considers the following criteria as characteristics of intestinal metaplasia: regular, columnar-lined epithelial surface, dark mucin goblet cells easily identified, equidistant glands, glands equal in size and shape, regular cells, equidistant cells (Figure 3).
Probe-based confocal laser endomicroscopy (pCLE) pictures showing: (a) non-dysplastic Barrett’s oesophagus with goblet cells easily identified, regular columnar-lined epithelium, equidistant glands and regular and equidistant cells, and (b) Barrett’s oesophagus with early oesophageal adenocarcinoma with goblet cells not easily identified and loss of structure.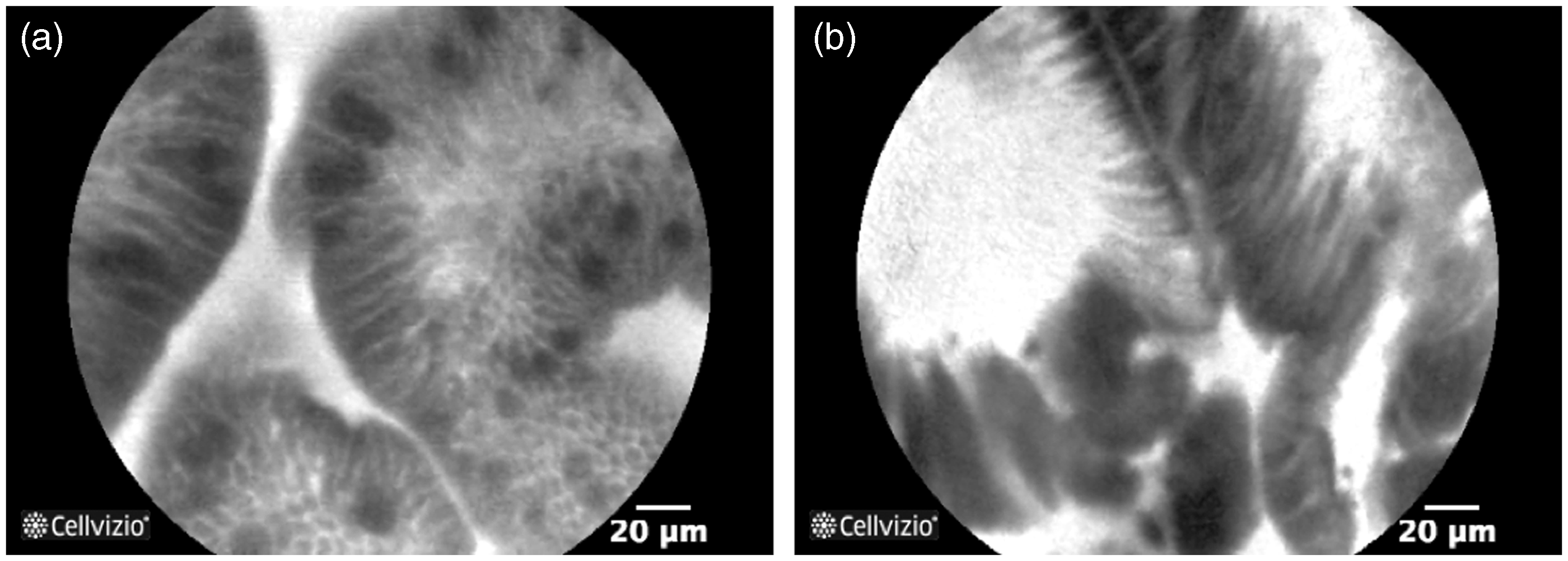
- Evidence: ++: 30%, +: 40%, –: 25%, – –: 5%
The currently recommended Seattle protocol implies a high number of biopsies, most of which are finally diagnosed as negative. It has been shown 11 that targeted biopsies have a higher diagnostic yield than random biopsies. The use of CLE to decrease the number of physical biopsies is supported by the results of a recent randomised clinical trial performed by Canto et al. 7 In this study, 192 patients with BE, enrolled for routine surveillance or referred for early neoplasia, were randomised into two groups: high-definition (HD)-WLE + random biopsies and HD-WLE + eCLE + targeted biopsies. Real-time diagnoses and management plans were recorded in the two groups. As a result, HD-WLE + eCLE + targeted biopsies had the ability to decrease the number of physical biopsies by 80%, and thus reduced the associated costs and tripled the diagnostic yield for neoplasia (22% of biopsies showed dysplasia for targeted sampling compared to 6% for random sampling). The addition of eCLE to HD-WLE increased the sensitivity of neoplasia detection (from 40% to 95%) without impairing the specificity. Overall, the NPV of CLE for the detection of neoplasia was very high (well above 90%) in all the reported studies (Table 2).
- Evidence: ++: 50%, +: 45%, –: 0%, – –: 5%
Canto et al. 7 showed that the yield for neoplasia increased from 6% for HD-WLE + random sampling to 22% for HD-WLE + eCLE + targeted sampling. The improvement in the yield for neoplasia was due to the reduction of the number of physical biopsies in conjunction with an increased sensitivity. Bertani et al. 5 compared the dysplasia detection rate between HD-WLE and pCLE, showing that pCLE had a significantly higher yield than HD-WLE (p = 0.04). Dunbar et al. 12 also demonstrated an increased detection rate of pCLE compared with HD-WLE (34% and 17%, respectively).
- Evidence: ++: 75%, +: 25%, –: 0%, – –: 0%
WLE-targeted biopsies are not sensitive enough for a proper assessment. The addition of pCLE has been shown to double the sensitivity for detecting dysplasia compared with recommended procedures using WLE and biopsies, with more than half of the dysplastic lesions found in endoscopically normal-appearing mucosa. 2 More data could be useful to confirm that pCLE enables the detection of more patients with dysplasia, in addition to more dysplastic lesions.
- Evidence: ++: 20%, +: 50%, –: 30%, – –: 0%
CLE random sampling, positive for neoplasia in at least one lesion/location, should be sufficient to decide to treat the lesion endoscopically (if applicable) immediately during the diagnostic procedure. In the case of a patient referred for a therapeutic intervention such as radio-frequency ablation (RFA) or endoscopic mucosal resection (EMR), the exact location and extent of the lesion must be reassessed prior to treatment, through histopathological assessment of new biopsies. Indeed, WLE alone may not provide sufficient information to proceed to treatment, and treatment may be delayed to the following endoscopic session. pCLE provides additional microscopic diagnostic information in real time with high accuracy (Table 2), allowing, in theory, immediate decision making and subsequent resection/ablation if applicable. However, at the present time, legal responsibility may still require tissue sampling to document decision making.
- Evidence: ++: 15%, +: 50%, –: 35%, – –: 0%
Preserving the function of the oesophageal junction is critical for the quality of life of patients. Microscopic in vivo assessment of the lesion provides additional information enabling the physician to optimise the treatment and to favour the most conservative, yet complete, margins.8,13 Although the level of evidence to support this strategy was judged to be limited, the panellists supported this practice.
- Evidence: 5% (++: 5%, +: 0%, –: 35%, – –: 60%)
Statement rejected
Accurate evaluation of tumour invasiveness and the presence of lymph node metastasis is essential to orient the patient between endoscopic or surgical treatments. The current limitations of the technique explain the rejection of this statement.
- Evidence: 40% (++: 10%, +: 30%, –: 55%, – –: 5%)
Statement rejected
Currently, the only surveillance method used after ablative treatment is a random biopsy performed on the treated area. However, this sampling provides limited information on the nature of the treated lesion and may impair future retreatment due to induced fibrosis. pCLE provides microscopic imaging that has not yet been correlated with image interpretation criteria for this application.
- Evidence: 60% (++: 10%, +: 50%, –: 30%, – –: 10%)
Statement rejected
Patients treated by EMR for dysplastic BE lesions require an endoscopic follow-up procedure to assess the completeness of the treatment and to proceed with a new treatment if needed. Randomised trials demonstrated that the accuracy of pCLE was higher than the accuracy of WLE alone for the characterisation of residual neoplasia. Bertani et al. showed an accuracy of 86%, 5 and Sharma et al. 2 65%. These results encourage the use of pCLE in this application; however the level of clinical evidence should be increased.
- Evidence: 65% (++: 10%, +: 55%, –: 30%, – –: 5%)
Statement rejected
Due to the transformation of oesophageal tissue after ablation, the interpretation of CLE remains to be defined after ablation therapy.
- Evidence: ++: 40%, +: 45%, –: 15%, – –:0%
The use of CLE as an important part of the management of patients with neoplasia has already been acknowledged in US guidelines. 1 The opinion expressed by the panellists suggests that BE should be added to the list of neoplastic conditions for which CLE may affect management decision, especially after outcomes-oriented data 7 have been reported in the literature.
Biliary strictures
Available background knowledge
Diagnostic value of pCLE in the characterization of indeterminate biliary strictures (main published articles)
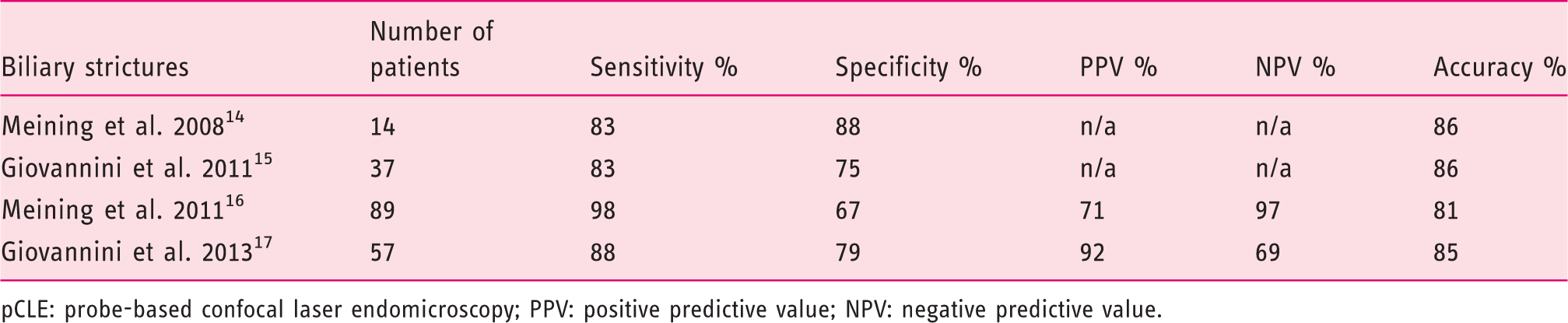
pCLE: probe-based confocal laser endomicroscopy; PPV: positive predictive value; NPV: negative predictive value.
Results by statement
Six statements were adopted and three were rejected.
- Evidence: ++: 63%, +: 31%, –: 6%, – –: 0%
pCLE has been demonstrated to be technically feasible and safe for biliopancreatic duct lesions, by delivering the confocal miniprobe either through a standard ERCP catheter or through a cholangioscope. 16
- Evidence: ++: 25%, +: 63%, –: 12%, – –: 0%
ERCP with tissue sampling is the standard of care to assess the pancreaticobiliary ductal epithelium within an indeterminate stricture. However, histologic confirmation of pancreaticobiliary malignancy provides only limited diagnostic accuracy, with about 50% sensitivity.16,18,19 The benefits of pCLE to obtain a more accurate characterisation of biliary strictures than with ERCP was strongly acknowledged by the panellists. pCLE allows a microscopic evaluation of the biliary epithelium in vivo (Figure 4). In a study by Meining et al.,
16
the sensitivity was 85% for ERCP + pCLE + biopsies and only 40% for ERCP alone + biopsies. Several other studies have shown a significant increase in sensitivity compared to tissue sampling techniques (Table 3) and this has resulted in the development of standardised image interpretation criteria, which have been proven to be highly accurate for the in vivo characterization of biliary lesions.20,21
Probe-based confocal laser endomicroscopy (pCLE) pictures showing: (a) healthy bile duct mucosa with a reticular network of thin dark branching bands and a grey background, and (b) malignant bile duct mucosa (cholangiocarcinoma) with epithelial borders.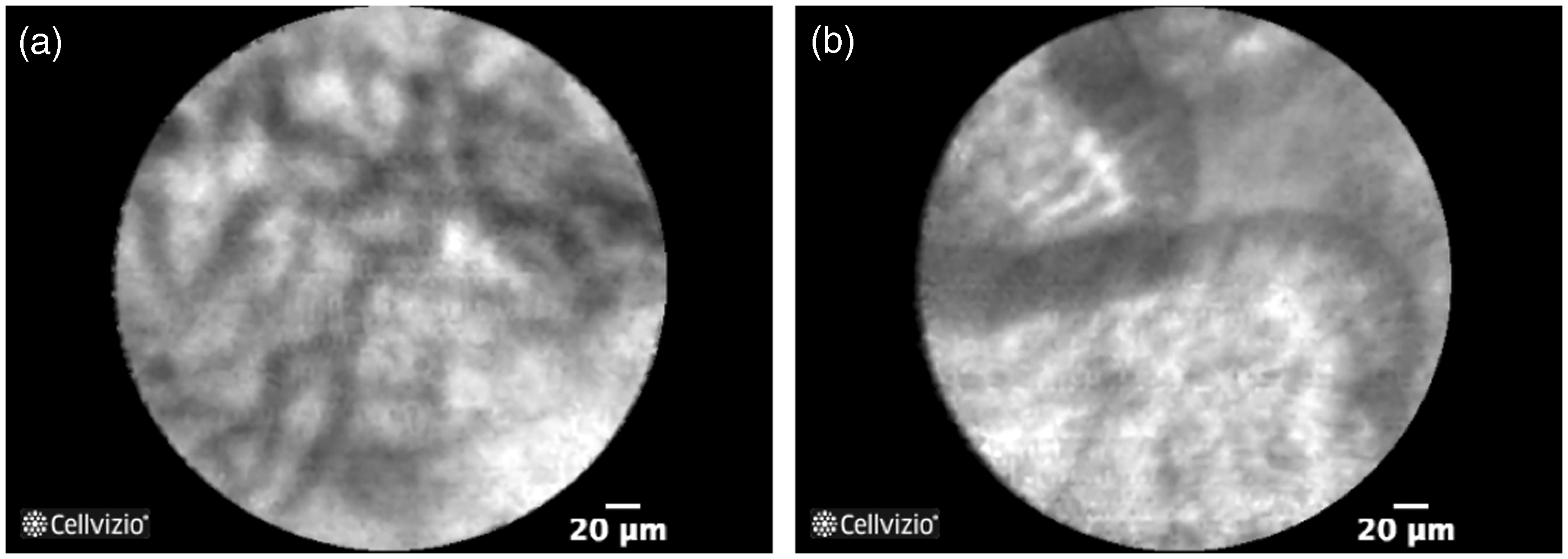
- Evidence: ++: 25%, +: 38%, –: 37%, – –: 0%
Statement rejected
The presence of a stent can induce inflammation and other modifications in the tissue microstructure. A retrospective analysis 21 based on the study of Meining et al. 16 showed that the accuracy of pCLE was slightly lower when the patients had a stent removed immediately prior to pCLE imaging (73% vs. 87%, respectively, p < 0.001), but the difference was not statistically significant. The sensitivity was, respectively, 75% and 88% (p = 0.71), and the specificity, 71% and 83% (p = 1). Image interpretation criteria should be refined to limit false positives due to stenting and inflammation. A prospective evaluation is ongoing. 21
- Evidence: ++: 38%, +: 50%, –: 12%, – –: 0%
pCLE has been shown to have a very high NPV (Meining et al., 16 97%, Slivka et al., 22 83%), enabling physicians to rely on negative results with confidence during an ERCP procedure.
- Evidence: ++: 25%, +: 63%, –: 12%, – –: 0%
Currently, yields from standard tissue sampling with biopsy or brushings in indeterminate biliary stricture remain low. Lack of confirmation of malignancy occurs from negative sampling results in clinical uncertainty, which can be difficult to accept for both the patient and the physician. Moreover, according to the published literature, 23 a significant proportion of patients sent for surgical resection are ultimately found to have benign pathology. Thus, the current diagnostic armamentarium is far from optimal, leading to frequent over-treatment (unnecessary surgery for patients who don’t need it) and under-treatment (delayed surgical treatment for patients who do need it).
pCLE of indeterminate biliary strictures has been shown to have a high NPV and a greater overall diagnostic accuracy than biopsies and/or brushings.17,19,24 Thus, the panellists supported the use of pCLE in the evaluation of biliary strictures, as a mean to increase diagnostic accuracy and improve clinical decision making.
- Evidence: ++: 38%, +: 37%, –: 19%, – –: 6%
CLE has already been cited in ASGE guidelines for the management of patients with biliary strictures. 1 Guidelines in development should also incorporate the value of CLE for biliary strictures.
- Evidence: ++: 6%, +: 50%, –: 31%, – –: 13%
Statement rejected
No red-flag technique has been shown to be useful to improve the characterisation of biliary strictures.
- Evidence: ++: 6%, +: 50%, –: 38%, – –: 6%
A comprehensive analysis of the correlation of biliary pCLE images and histology, utilising a novel frozen sectioning protocol, was carried out recently, during which typical pCLE images were reproduced ex vivo, allowing for multimodal assessment. 25 Findings from this work indicated that ‘black bands’ were collagen fibrils, which support the network of ‘white bands’ structurally and, predictably, are increased in diameter in pathologic specimens. This study is the only evidence of such a correlation and needs to be further validated.
- Evidence: ++: 12%, +: 44%, –: 44%, – –: 0%
Statement rejected
The results of the work mentioned in the previous statement, 25 contrary to previous reports, suggested that the previously termed ‘white bands’ were lymphatic sinuses and small blood vessels. To date, there has been no report recognising this complex subepithelial plexus of lymphatic vessels, suggesting that pCLE could redefine traditional histology tenets.
Colorectal lesions
Available background knowledge
Diagnostic value of pCLE in the characterization of colorectal lesions (main published articles)
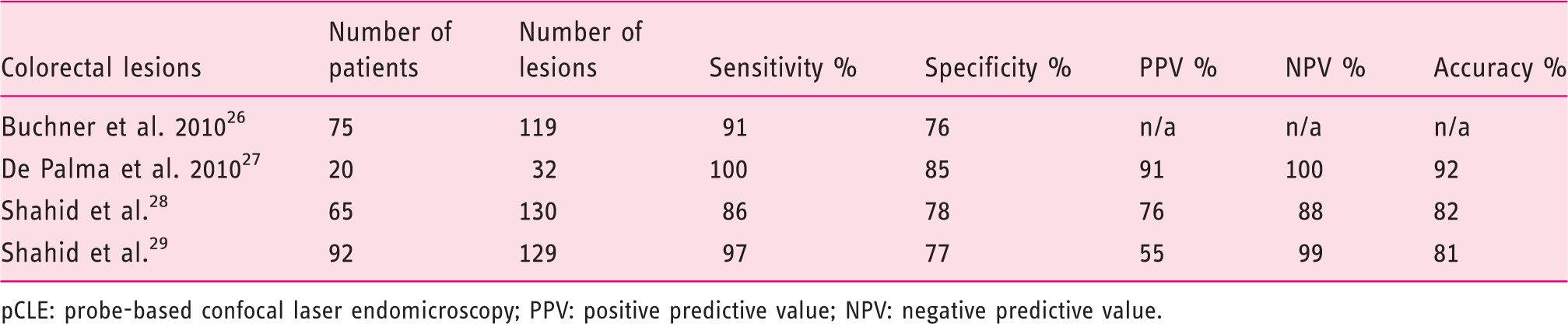
pCLE: probe-based confocal laser endomicroscopy; PPV: positive predictive value; NPV: negative predictive value.
Results by statement
Fifteen statements were adopted and five were rejected.
Mucosa and lesion characterisation:
- Evidence: ++: 44%, +: 37%, –: 19%, – –: 0%
The value of pCLE to identify normal colorectal mucosa and to eliminate indetermination was acknowledged by the panellists. A set of interpretation criteria has been developed to characterise the tissue and to be able to differentiate neoplastic from non-neoplastic mucosa in colorectal lesions.
10
Healthy colon is characterised by round crypt structures, dark goblet cells and regular and narrow vessels surrounding the crypts (Figure 5). Several clinical studies have shown a very good NPV using this classification (Table 4).
Probe-based confocal laser endomicroscopy (pCLE) pictures showing: (a) healthy colon mucosa with round crypt structures and dark goblet cells, and (b) hyperplastic lesion with crypts with slit or stellate openings surrounded by uniform epithelium and goblet cells.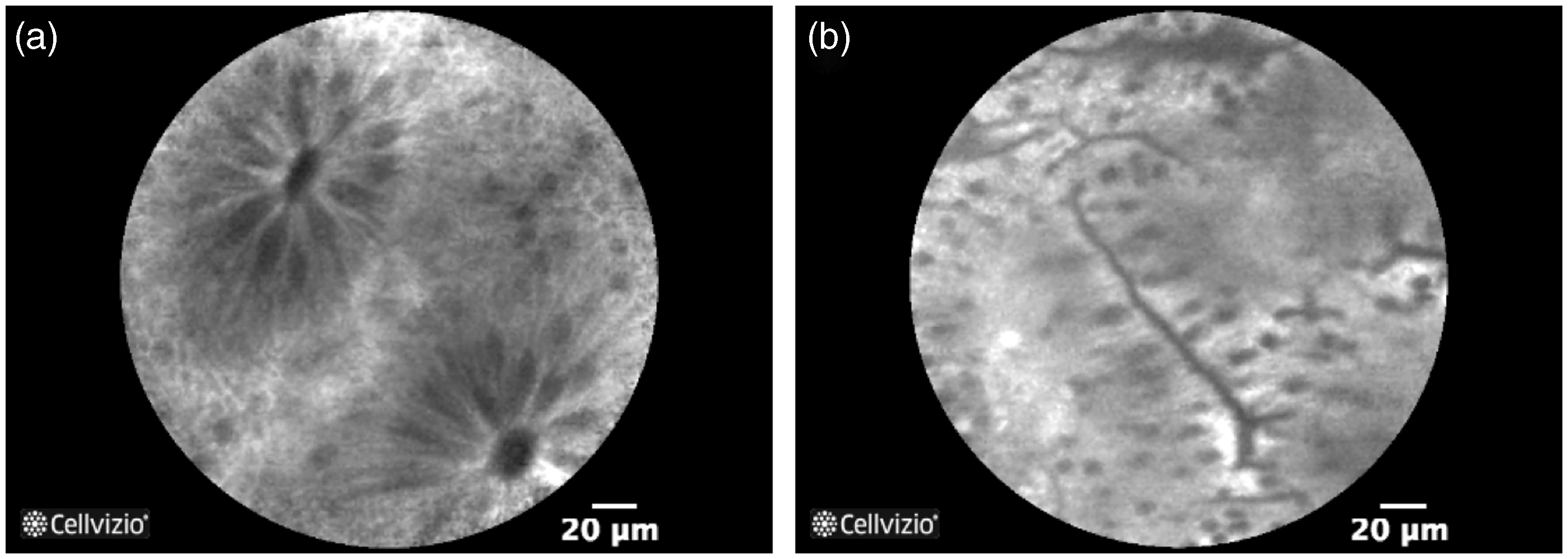
- Evidence: ++: 32%, +: 31%, –: 31%, – –: 6%
Statement rejected
The clinical value of pCLE for the characterisation of these lesions and for the management of the associated treatment has been reported in numerous studies, with an accuracy always higher than 80% (Table 4). However, the impact of this high accuracy is to be established depending on the type and size of the polyp, as well as on the requirements of scientific societies and on liability considerations.
- Evidence: ++: 38%, +: 31%, –: 31%, – –: 0%
Conventional endoscopy has a limited ability to discriminate adenomatous from nonadenomatous colorectal polyps. The Miami Classification 10 describes dysplastic neoplasia with the following microscopic features: tubular and villous structures, thickening of the epithelial lining, dark cells and distorted or elongated crypts. These features are clearly different from the features of non-neoplastic lesions, such as normal mucosa, hyperplastic or serrated polyps. De Palma et al. 27 assessed the accuracy and inter-observer agreement (IOA) of pCLE in colorectal polyps using the Miami Classification, in a study involving 32 small polyps ranging from 1 mm to 9 mm, in 20 patients. Lesions were identified using WLE and then pCLE. pCLE achieved a sensitivity, specificity, PPV and NPV of 100%, 85%, 91% and 100%, respectively, in predicting adenomatous histology, using the final histopathological diagnosis as a reference. Other clinical trials focused on the differentiation between neoplastic and non-neoplastic lesions, hence the limited clinical evidence associated with this statement.
- Evidence: ++: 38%, +: 31%, –: 31%, – –: 0%
The Miami Classification 10 describes hyperplastic colorectal lesions with bright, non-thickened uniform epithelium, crypts with slit of stellate openings, and small vessels (Figure 5). Kuiper et al. 30 developed a very similar classification, also based on vessel and crypt architecture. All clinical studies performed to date have used these classifications. Although accepted by a large majority of experts, this statement was thought not to be sufficiently well supported in terms of clinical data.
- Evidence: ++: 0%, +: 38%, −: 37%, − −: 25%
Statement rejected
Sessile serrated adenoma polyps are thought to have a different degeneration profile compared with regular polyps and the in vivo distinction between sessile serrated adenomas and hyperplastic polyps is complicated. A limited number of studies have been performed suggesting the ability of pCLE to distinguish hyperplastic lesions from sessile serrated adenomas.31,32 These studies have highlighted image interpretation criteria, which could be used to distinguish these two types of polyps, but these early findings need to be validated prospectively.
- Evidence: ++: 38%, +: 31%, −: 25%, − −: 6%
The panellists accepted largely the use of CLE to identify colorectal carcinoma and to provide a faster diagnosis. According to the Miami Classification,
10
the microscopic appearance of neoplastic tissue presents disorganised patterns with the loss of structures. Several studies have assessed the accuracy of this classification (Table 4).
Combination of CLE and red-flag techniques:
- Evidence: ++: 19%, +: 50%, −: 31%, − −: 0%
The association of CLE with red-flag techniques in order to obtain higher-quality imaging assessment and more-complete information was supported by the panellists. Shahid et al. 29 reported the high accuracy of the association of pCLE + NBI. Buchner et al. 26 reported a comparison of the accuracy of pCLE with virtual chromoendoscopy (NBI or Fuji Intelligent Colour Enhancement, FICE). In this study, the sensitivity of pCLE was higher than that of virtual chromoendoscopy (91% and 77%, respectively, p = 0.010), and the specificity was not significantly different (76% and 71%, respectively, p = 0.77), indicating that the association of both techniques should aid better-informed decision making, with high confidence.
- Evidence: ++: 6%, +: 56%, −: 25%, − −: 13%
Statement rejected
The studies reported in the previous statement support the fact that CLE is more accurate than digital chromoendoscopy. A recent meta-analysis by Wanders et al. 33 concluded that both narrow-spectrum endoscopy (NBI, FICE and i-scan) and CLE, but not autofluorescence imaging, could be used to differentiate neoplastic and non-neoplastic lesions, when performed by appropriately trained endoscopists. Although the diagnostic performance of CLE seemed better compared with other techniques, it is not yet possible to conclude from available data that CLE significantly outperforms digital chromoendoscopy. Further trials with head-to-head comparison are needed.
- Evidence: ++: 19%, +: 56%, −: 25%, − −: 0%
The risk of malignant degeneration of an adenomatous polyp is largely dependent on its size. For small, diminutive adenamatous polyps with a diameter inferior to 6 mm, the risk is actually very low. For these diminutive polyps, the necessity arises either to remove them or just to survey for further endoscopy. In the document entitled Preservation and Incorporation of Valuable endoscopic Innovations (PIVI), the ASGE provides guidance for the adoption of virtual biopsy techniques in the characterisation of colorectal neoplasia. 34 The PIVI initiative suggests two strategies for patient management: ‘resect, diagnose and discard’ and ‘leave hyperplastic polyps behind’. The initiative states that an NPV and an accuracy higher than 90% and a high confidence in the observations are necessary to enable a technology to guide the decision to leave a suspected polyp ≤ 5 mm in size in place. The objective of the ‘leave behind’ strategy is to limit the number of resections and thus the duration of the procedures, as well as the number of resected specimens sent for histopathological evaluation. This conservative strategy has some inconveniences, including legal considerations. Another option consists of the removal of diminutive polyps without further histologic assessment (the so-called ‘resect, diagnose and discard’ strategy), a strategy that saves time and money by reducing the number of histopathological evaluations, but requires close follow-up.
Shahid et al. 28 performed high-definition colonoscopies on 65 patients with 130 polyps. The surface pit pattern of all polyps smaller than 9 mm in size was determined in vivo. CLE imaging was then performed and analysed offline, blinded to endoscopic characteristics and histopathology. The accuracy, sensitivity, specificity, PPV and NPV for the combination of pCLE + NBI were higher than the threshold set by the PIVI initiative: 95%, 94%, 97%, 97% and 94%, respectively. The results did not report the accuracy of the combination of both techniques in the subset of diminutive polyps. The results of Shahid et al. are encouraging regarding the potential of pCLE to enable one of the strategies of the PIVI initiative (‘leave behind’). However, in addition to requiring a high NPV and a high accuracy, the adoption of this strategy requires a significant change in clinical practice from a community of physicians who are used to resecting all polyps, even diminutive ones.
- Evidence: ++: 6%, +: 50%, –: 31%, – –: 13%
Statement rejected
Hyperplastic polyps of less than 10 mm are benign tumours not requiring resection. Therefore, in vivo identification of the histological pattern of these polyps could help the decision to leave them behind. This strategy is supported by the generally high NPV of pCLE in colorectal lesions, but needs further confirmation for this specific set of polyps.
Offline and real-time decision making:
- Evidence: ++: 44%, +: 44%, –: 12%, – –: 0%
There was a consensus to validate the benefits of the use of pCLE to characterise colonic tissue during the endoscopy procedure. The main results supporting this statement are reported in Table 4.
- Evidence: ++: 38%, +: 25%, –: 37%, – –: 0%
CLE provides in vivo microscopic videos of the mucosa that can be recorded and reviewed after the procedure. Shahid et al. 35 compared the overall accuracy of real-time and offline pCLE diagnosis for 154 polyps and the two accuracies were not significantly different (79% vs. 83%, respectively). Reviewing offline pCLE images is feasible and the panellists agreed that this practice could be useful for beginners in pCLE, to better understand and learn the interpretation criteria of the microscopic imaging (statement reported in Appendix).
- Evidence: ++: 32%, +: 31%, –: 31%, – –: 6%
The study performed by Shahid et al.
35
comparing the performances of online and offline pCLE showed that real-time interpretation is slightly less accurate than offline diagnosis, but overall both are not statistically different. Thus, the in vivo additional information brought by pCLE during the procedure can be used to obtain a higher-confidence decision making.
Management of patients with colorectal lesions:
- Evidence: ++: 6%, +: 44%, –: 50%, – –: 0%
Statement rejected
As already explained in statement CL9, the risk of malignant degeneration for small polyps (< 10 mm) is relatively low. The use of pCLE for patients with small colonic polyps is supported by the generally high NPV and accuracy of pCLE in colorectal lesions, but the number of studies focusing on small polyps was considered by the panellists to be too low for this statement to be adopted.
- Evidence: ++: 19%, +: 37%, –: 31%, – –: 13%
The panellists considered that physicians could base their therapeutic decision on CLE imaging presenting signs of high-grade dysplasia or cancer. Several studies have demonstrated that pCLE has the ability to characterise colonic neoplasia accurately, with a high sensitivity (Table 4). This being performed in real time, detailed information can be used to improve patient management, avoiding further delays and triggering an immediate therapeutic resection when applicable. The statement was adopted even though the panellists considered that the grade of evidence remained low.
- Evidence: ++: 13%, +: 50%, –: 25%, – –: 12%
The ability of pCLE combined with digital chromoendoscopy to identify residual neoplastic colorectal lesions, and to define the extent of the potential additional resection, was approved by the panellists, based on the Shahid et al. study 29 reported above. More studies would improve the level of evidence.
- Evidence: ++: 19%, +: 25%, –: 37%, – –: 19%
The use of CLE to determine the margins of flat colorectal lesions directly during the procedure can increase the accuracy of the resection and reduce the risk of recurrence or complication (bleeding and perforation of the colon). This strategy was supported by the panellists, based on the accuracy of results reported in the different clinical studies (Table 4). However, further studies, especially to evaluate the performance of the technique for the characterisation of margins, are necessary.
Surveillance of patients after resection or ablation:
- Evidence: ++: 19%, +: 38%, –: 37%, – –: 6%
After EMR, about a quarter of lesions show residual or reoccurring neoplastic tissue. 29 The neoplasia foci can be confirmed by means of the histopathological assessment of a corresponding biopsy taken during the follow-up procedure, and can be treated during a subsequent endoscopic session or evaluated empirically based on a macroscopic assessment of the margins. Both approaches are suboptimal. The first approach leads to repeat colonoscopy procedures with inherent costs, while the second carries the risk of either under- or over-treatment. Microscopic assessment of the tissue, before and during the resection, can bring more information and detect residual or reoccurring neoplasia. The grade of evidence was considered by the panellists to be low, because only one large study has assessed the role of CLE for this purpose. However, the results of this study are very encouraging. Shahid et al. 29 combined pCLE + virtual chromoendoscopy in a study involving 92 patients (with a total of 129 scars) who underwent follow-up colonoscopies for the evaluation of prior EMR sites. The sensitivity of pCLE was statistically higher compared with high-resolution endoscopy + virtual chromoendoscopy (97% vs. 72%, respectively, p = 0.045), but there was no statistically significant difference in accuracy and specificity (81% vs. 77%, p = 0.23 and 77% vs 78%, p = 1.0, respectively). When combining pCLE + virtual chromoendoscopy in real time, and taking into account only the scars for which both techniques were in agreement regarding the diagnosis, the accuracy, sensitivity, specificity, PPV and NPV were, respectively, 88%, 100%, 85%, 60% and 100%, compared with histopathology. Thus, microscopic visualisation of the mucosa with CLE during the assessment of previously resected colorectal areas seems to be useful to assess the completeness of the treatment and to trigger retreatment if needed.
- Evidence: ++: 13%, +: 31%, –: 56%, – –: 0%
In several recently published studies,29,36 up to 20% of patients had residual or reoccurring neoplastic tissue identified on follow-up colonoscopy within a year of their initial examination. The previously reported study 29 suggested that pCLE would be useful to detect neoplastic lesions during the year following a previous EMR.
- Evidence: ++: 12%, +: 44%, –: 44%, – –: 0%
Although the grade of evidence seemed to be suboptimal, the panellists supported the association of pCLE + digital chromoendoscopy to suggest the absence of residual neoplasia during surveillance after an EMR or ablation. This is based on the results of Shahid et al. presented in statement CL18.
Inflammatory bowel diseases (IBD)
Available background knowledge
Contrary to sporadic colorectal cancer (CRC), IBD neoplastic tissue is often flat and multifocal. The risk of CRC increases in particular with longer duration and extensive severe colitis, and family history of CRC. Patients with ulcerative colitis (UC) who have left-sided colitis or more extensive disease are at increased risk. In Crohn’s colitis, those patients with extensive disease involving more than one-third of the colon also have an increased risk of CRC, similarly to patients with UC. 37 The extent of colonic involvement should be based on both endoscopic and histologic criteria, which can reveal more-extensive disease. Patients with UC or extensive Crohn’s colitis should undergo surveillance colonoscopy every one to two years, beginning eight to 10 years after disease onset. Even if there is no definitive evidence that surveillance colonoscopy extends survival, patients in surveillance programmes tend to have cancers detected at an earlier stage.
A large number of biopsy specimens are recommended to ensure proper surveillance colonoscopy in IBD, making this time-consuming and prone to sampling error, with a low diagnostic yield. 38 Several clinical trials have reported that the diagnostic yield for the detection of neoplasia in an inflammatory environment using targeted biopsies is higher compared with conventional colonoscopy. 39 Chromoendoscopy with topical dye application enhances the detection of flat neoplastic tissue in IBD. In a study by Kiesslich et al., 40 161 patients with long-term UC in clinical remission were randomised at a 1:1 ratio to undergo either a conventional colonoscopy with random biopsies or an association of chromoendoscopy + eCLE with targeted biopsies. Chromoendoscopy + eCLE detected 4.75-fold more neoplastic lesions in comparison with conventional colonoscopy, thus reducing the number of biopsies needed by 50%. Other studies have been performed and are reported below.
Results by statement
Thirteen statements were adopted and four were rejected.
- Evidence: ++: 0%, +: 25%, –: 38%, – –: 37%
The step-up treatment approach is the traditional approach for patients with moderate to severely active disease. It starts with the mildest form of drug therapy and then moves to the next step if the patient does not respond to the treatment. The step-down therapeutic approach is based on an aggressive model that includes the early introduction of immunomodulators and biologics. Both approaches have benefits and limitations. The prediction of long-term IBD outcomes is necessary to individualise the treatment to prevent complications and enhance complete remission endoscopically, histologically and biologically. The statements reported below acknowledged that mucosal healing was an important prognostic feature of the efficacy of treatment in IBD and could be identified with CLE.41–45 The integration of CLE and the concept of mucosal healing in the patient management strategy should be further defined in order to enable physicians to characterise the mucosa microscopically, to rationalise therapeutic strategies and to initiate or stop treatment when appropriate.
- Evidence: ++: 63%, +: 12%, –: 25%, – –: 0%
pCLE can be used to target physical biopsies in patients with IBD. Such an approach should replace random four-quadrant biopsies in order to improve the yield and efficiency of the procedure and to decrease the number of histopathological examinations needed. Random four-quadrant biopsies have a very low yield in patients with IBD, even lower than in patients with BE.46,47
- Evidence: ++: 63%, +: 37%, –: 0%, – –: 0%
Kiesslich et al. (38) used the combination of eCLE + chromoendoscopy to detect neoplasia in flat or suspected lesions in a randomized study including 161 patients with long-standing UC. There were 4.75 times more neoplastic lesions detected compared with conventional colonoscopy, and the number of biopsy specimens was reduced by half. A case report from De Palma et al. 48 described the use of mass (DALM). Coron et al. 49 enrolled 73 patients with UC or CD in a prospective study in which the information obtained with pCLE correlated well with routine histology, thus reducing the need for multiple biopsies.
- Evidence: ++: 13%, +: 87%, –: 0%, – –: 0%
Neumann et al. 50 developed a specific score, the Crohn’s Disease Endomicroscopic Activity Score (CDEAS), to assess CD activity in vivo with CLE. The CDEAS included six parameters, corresponding to interpretation criteria, identified as discriminant for active versus inactive CD and controls: (i) crypt number (increased or decreased), (ii) crypt distortion, (iii) micro-erosions, (iv) cellular infiltrate, (v) vascularity, (vi) number of goblet cells (increased or decreased). By assigning one point for each given parameter, the score ranged from 0 to 8. In a study including 54 patients, the median CDEAS was 2 for patients with quiescent CD and 5 for patients with active CD, with a significant association with C-reactive protein (2.8 and 24.5, respectively, p = 0.005), an already-established biological inflammatory marker of CD.
- Evidence: ++: 25%, +: 75%, –: 0%, – –: 0%
eCLE has been shown to correlate well with histological findings in UC. The most efficient combination in UC surveillance is chromoendoscopy + CLE. Chromoendoscopy is the gold standard to detect suspicious areas, which can then be examined by CLE to identify histological changes, confirm intraepithelial neoplasia and guide immediate therapy. Many authors refer to the classification for UC established by Kiesslich et al.
40
in 2007, which differentiates normal mucosa, regeneration, neoplasia and inflammation, using crypt architecture, cellular infiltration and vessel architecture (Figure 6). Recent data have also reported the ability to differentiate between CD and UC, based on specific aspects used for conventional histology.
51
Probe-based confocal laser endomicroscopy (pCLE) pictures showing: (a) inflamed colon mucosa with difference in shape, size and distribution of crypts, increase of capillaries dilated and distorted and cellular infiltration, and (b) dysplastic colon mucosa with ridged-lined irregular epithelial layer with loss of crypts and goblet cells and irregular cell architecture with little or no mucin. Dilated and distorted vessels with increased leakage could also be observed.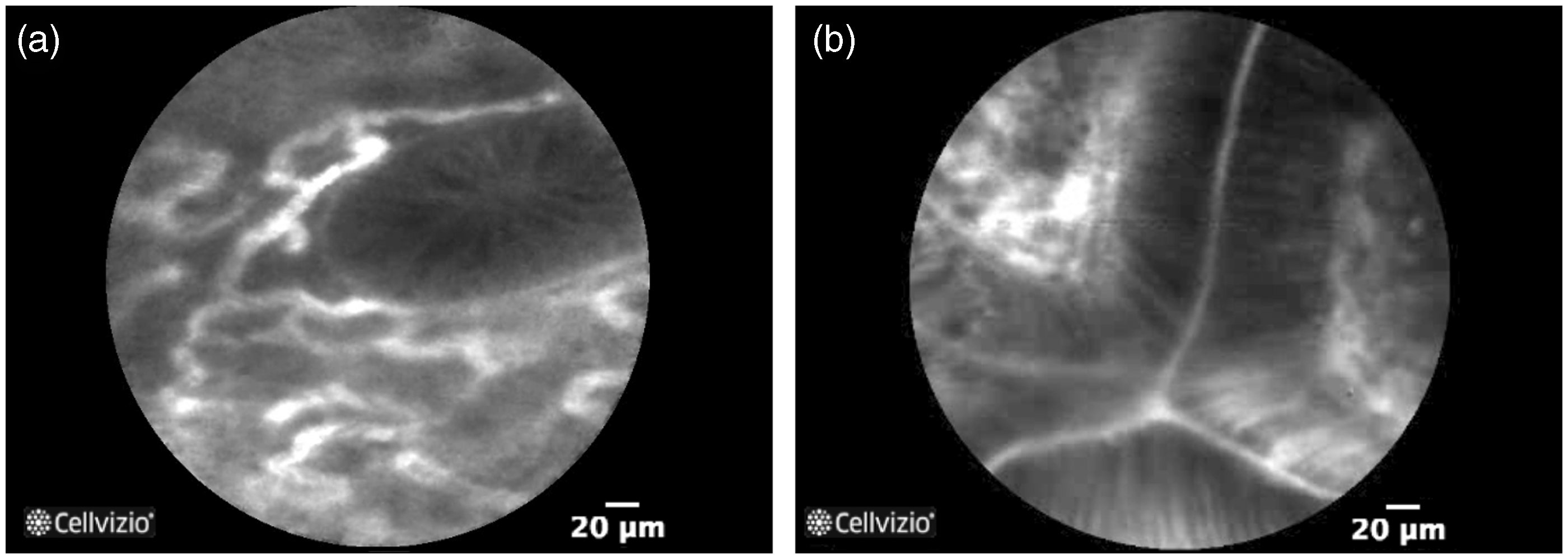
- Evidence: ++: 63%, +: 25%, –: 12%, – –: 0%
The panellists acknowledged the utility of random CLE sampling during IBD evaluation to increase the chances of identifying inflammation that may not have been found during the macroscopic evaluation of the mucosa. Neumann et al. 41 developed a new classification for eCLE and pCLE, to predict histological inflammation in macroscopically non-inflamed mucosa, where accuracy, sensitivity, specificity, PPV and NPV were 87%, 94%, 81%, 82% and 94%, respectively.
- Evidence: ++: 50%, +: 38%, –: 12%, – –: 0%
In addition to macroscopic data, CLE can provide in vivo functional information which may aid in the characterisation of intestinal barrier function and vascular permeability. In IBD, the barrier function is affected, leading to more permeability through the epithelial lining. This permeability is enhanced by vascular leakage. As CLE is currently mostly performed with an intravenous injection of sodium fluorescein used as a contrast agent to optimise image quality, fluorescein leakage can be assessed and quantified visually as a marker of intestinal barrier dysfunction.42–45,52–54
- Evidence: ++: 38%, +: 37%, –: 25%, – –: 0%
The results reported in statement IBD6 suggested that CLE should be used during the surveillance of IBD, to detect more inflammation in the macroscopically non-inflamed mucosa. However, more clinical evidence should be developed in order to validate this strategy in clinical practice.
- Evidence: ++: 25%, +: 50%, –: 25%, – –: 0%
Contrary to standard pathology, CLE offers the ability to visualise dynamic mechanisms, which could have a predictive value for clinical disease course and outcomes. There is at present no worldwide accepted classification of CLE images in IBD, but all classifications use dynamic features such as vascular flow information as well as cellular infiltration or depletion. Many authors refer to the classification established by Kiesslich et al. 38 As for CD, Neumann et al. 50 recently developed the CDEAS to assess CD activity in vivo. With biomarkers such as epithelial gaps or vessel leakage,43–45 physicians could predict flares and anticipate relapse.
- Evidence: ++: 25%, +: 75%, –: 0%, – –: 0%
In patients with UC, as inflammation is limited to the mucosal layer, mucosal healing may represent the ultimate therapeutic goal. In CD, the lesion can impact the entire wall and a more complete healing may be necessary. If the mucosa heals, it is thought that disease complications are unlikely to occur and future hospitalisation and surgery requirements should decrease. pCLE has been shown to allow the visualisation of residual cellular inflammation41,43–45 even when the patient presents clinical symptoms compatible with remission, redefining the term ‘mucosal healing’ in vivo.
-
- Evidence: ++: 71%, +: 29%, –: 0%, – –: 0%
The risk of CRC is increased in patients with IBD. In particular, UC patients should undergo colonoscopy surveillance to identify flat dysplasia, which is usually detected microscopically in random biopsies from unremarkable mucosa.36,55 It has been calculated that, when random biopsies are performed, 33 biopsy specimens are needed to exclude dysplasia, with a sensitivity of 90%.56–58 This diagnostic approach is thus considered to be time-consuming and unlikely to be cost-effective. CLE allows for unlimited sampling of the colonic mucosa. Moreover, published results have shown that eCLE has an excellent diagnostic accuracy for the detection of dysplasia/neoplasia in UC patients, with accuracy, sensitivity and specificity of 97.8%, 94.7% and 98.3%, respectively, 38 and that the detection rate was increased by a factor of 4.75.
- Evidence: ++: 13%, +: 25%, –: 37%, – –: 25%
Statement rejected
There is no specific clinical evidence to support this strategy and clinical trials comparing standard and tailored management are necessary.
- Evidence: ++: 13%, +: 37%, –: 13%, – –: 37%
The development of anti-TNF antibodies has led to remarkable progress in IBD therapy. 59 The role of CLE in the assessment of the efficacy of this therapy by evaluating residual inflammation before the clinical symptoms appear, or conversely by confirming complete remission, would enable the adaptation of the treatment to each patient in a proactive manner. Atreya et al. 60 created a fluorescent antibody for molecular membrane-bound TNF (mTNF) that was administrated in 25 patients with Crohn’s disease and evaluated with pCLE. Patients with a high number of mTNF+ cells showed significantly higher short-term response 12 weeks after anti-TNF therapy, compared with patients with a low amount of mTNF+ cells. This clinical response was sustained during the one-year follow-up period and was associated with mucosal healing observed in follow-up endoscopy. Clinical validation of this high-impact application still needs to be performed in vivo and in a higher number of patients.
- Evidence: ++: 0%, +: 38%, –: 37%, – –: 25%
Statement rejected
Microscopic evaluation could enable physicians to detect a relapse before clinical symptoms appear. Early reports seem to be promising, but a deeper clinical evaluation should be performed.
- Evidence: ++: 0%, +: 38%, –: 50%, – –: 12%
Statement rejected
To date, there have been only two case reports61,62 describing the use of eCLE and pCLE respectively, in lymphocytic colitis. In this setting, CLE has the potential to detect lymphocytic colitis in vivo, therefore reducing the number of biopsy specimens necessary to establish such a diagnosis. More evidence is needed to confirm whether CLE can identify lymphocytic colitis in a routine clinical setting.
- Evidence: ++: 0%, +: 25%, –: 63%, – –: 12%
Statement rejected
A single case report 63 has described eCLE findings in collagenous colitis. More evidence is needed to determine whether CLE can identify collagenous colitis.
- Evidence: ++: 14%, +: 29%, –: 57%, – –: 0%
Ideally, surveillance and monitoring of IBD patients should be performed using a combination of ‘red-flag’ techniques such as chromoendoscopy, NBI, or autofluorescence imaging to screen large surfaces of mucosa for ‘areas of interest’. These targeted areas could then be further evaluated at the microscopic level, using pCLE, to improve the characterisation of the tissue during the procedure. 37 Alternatively, an extensive random pCLE sampling can represent a good method to increase the detection yield. Further evaluation is still needed.
Discussion
A precise methodology was used to develop consensus statements on the use of CLE in gastroenterology. The adoption of a statement was based on the agreement level voted by the panellists. The grade of evidence was also assessed for each statement, and the results were used to understand the adoption and rejection decisions. Assessment of clinical evidence also included proof-of-concept studies with eCLE. Indeed, although most of the evidences were based on pCLE results, several landmark studies using eCLE were initially published, mostly in IBD. The evidence grade classification requires an in-depth systematic review of the current literature. The five group leaders of the initiative provided up-to-date literature to the participants, who undertook the responsibility to vote on their own conviction. The correlation between the level of agreement and the grade of evidence was not perfect for all applications. If a low (respectively, high) grade of evidence was associated with a low (respectively, high) grade of agreement, the correlation was high. However, in some cases, the agreement level was considered to be high whereas the grade of evidence was low. This was explained by the fact that the panel was composed of experts deeply involved in the technology and in its ongoing clinical validation, independent of a potential lack of current clinical evidence. To the contrary, no statement with a good grade of evidence was rejected. The least favourable correlation was observed for the colorectal lesions statements. Indeed, a differentiation must be made between large and small and diminutive polyps in terms of management. However, only a few studies have focused on small and diminutive polyps. The number of statements and the size of the panel were different for each topic. Finally, strong agreement was reached for only 16 of the 63 statements.
The use of pCLE in the evaluation of BE has been recognised for a list of clinical situations, including its use in conjunction with electronic enhancement, the surveillance of BE dysplasia in patients undergoing follow-up and the definition of the lateral extent of neoplasia prior to therapy. pCLE-targeted biopsies appear to reduce the number of physical biopsies and to increase the accuracy of the procedure, in real time. As a result, the yield for neoplasia is higher than that of WLE and random biopsies. Some commentators even claim that positive pCLE imaging in an endoscopically neoplastic-appearing oesophagus is sufficient for immediate therapeutic intervention. However, this largely depends on local rules and practices. The limitations acknowledged by the panellists were the inability of pCLE to determine the depth of invasion of an early neoplastic lesion and the lack of an established classification for the interpretation of pCLE imaging after ablation or resection. The clinical relevance of the detection of flat lesions by pCLE has recently been discussed by Boerwinckel et al., 64 because these lesions can be eradicated by ablation therapy. According to these highly recognised experts, most dysplastic lesions can be detected by HD-WLE. This can be true in their case, but difficult to generalise, even considering only tertiary centres. In this context, detecting more dysplastic lesions with pCLE, and even more importantly, more patients with high-grade dysplasia or early cancer, represents a significant and clinically relevant advantage.
The diagnostic performance of ERCP is limited by a flawed histological gold standard, due to accessibility issues. pCLE enables microscopic evaluation of the bile duct mucosa, which enhances the imaging arsenal of the physician and increases the accuracy of the procedure. The panellists acknowledged that pCLE is able to assist the physician in making clinical decisions, such as excluding malignancy. The understanding of the microscopic images obtained with pCLE still needs to be improved, to enable better adoption and confidence in the microscopic findings, but the panellists agreed on the necessity to include pCLE in the diagnostic guidelines for the assessment of biliary strictures.
The value of pCLE in the characterisation of colorectal lesions has been demonstrated for many years. A classification has been established, validated and enhanced. Since all large polyps are removed in daily practice, the impact of pCLE should be recognised for diminutive polyps as part of the ‘diagnose, resect and discard’ or ‘leave behind’ strategies suggested in the PIVI initiative. The panellists acknowledged that pCLE should be considered in the diagnosis of intramucosal neoplasia to trigger a therapeutic decision, the evaluation of the extent of the lesion and the associated therapy, and for post-resection surveillance. In order to be applied in daily clinical practice, pCLE needs to be recognised in the guidelines of scientific societies. This will also clarify the current responsibilities and legal implications underlying the histopathological evaluation of sampled specimens. Interestingly, guidelines recently published 65 by the European Society of Gastrointestinal Endoscopy (ESGE) ‘suggest that virtual chromoscopy can be used under strictly controlled conditions for real time optical diagnosis of diminutive colorectal polyps to replace histopathological diagnosis’. Such recommendation can certainly be extended to the case of pCLE.
The IBD statements were largely based on the integration of CLE into practice changes from the current management algorithm to an individualised one. The use of CLE to target biopsies in order to improve the performance of the procedure during surveillance of neoplasia in IBD patients was acknowledged by the panellists. They also agreed that systematic sampling with CLE can detect more dysplastic and early neoplastic lesions in long-standing UC. Specific CLE classifications to identify UC and CD were recognised by the panellists to enhance the endoscopic evaluation of the disease activity. The role of this technology to provide dynamic microscopic in vivo information to supplement endoscopic and clinical evaluations has been highlighted. However, the impact of CLE to deliver a tailored management of patients by anticipating clinical symptoms has not yet been established. The role of CLE to predict relapse rather than wait for clinical symptoms was recognised to have great potential, but required a deeper clinical evaluation before being recommended.
The 26 panellists agreed that pCLE should be used to enhance the diagnostic arsenal in the evaluation of BE, biliary strictures, colorectal lesions and IBD, by providing microscopic information which improves the diagnostic performance of the physician. In order to actually implement the technology in clinical routine, and to ensure good practice, standardised initial and continuing institutional training programmes should be established. Consensus statements on training and credentialing have also been developed during this project, and are reported in the Appendix.
Footnotes
Acknowledgements
The authors are grateful to Dr Joshi Virendra (Oschner Medical Centre, Oschner, LA, USA) and Prof Bernard Filoche (Hôpital St Philibert, Lille, France) for providing samples of pCLE pictures, and to Nolwenn Gaudin for her tremendous work in coordinating the whole process of this consensus report. The logistical support of Mauna Kea Technologies was very much appreciated.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest
Helmut Neumann: scientific support from Olympus, Pentax Medical, Fujifilm, EndoChoice, Abbvie, Siemens, SpectraScience, Smart Medical; lectures for Pentax Medical, EndoChoice, Abbvie, SpectraScience, Aptalis, Mauna Kea Technologies, Eisai, Recordati; and consultant for Pentax Medical, Fujifilm, Smart Medical, EndoChoice, Fraunhofer, SpectraScience. Khek Y Ho: member of the medical advisory board of Mauna Kea Technologies. Vani Konda: grant funding from Olympus and honoraria from Mauna Kea. Adam Slikva: research funding from Mauna Kea Technologies. Jean-Paul Galmiche: consultant for Mauna Kea Technologies. Kenneth K Wang: member of the medical advisory board of Mauna Kea Technologies. Herbert Wolfsen: research support from Olympus, NinePoint Medical; and consultant for CSA Medical, Mauna Kea Technologies, Covidien, and Fuji Film.