
Abstract
The dietary carbohydrate fructose can be incompletely absorbed in the small intestine and is sometimes associated with gastrointestinal symptoms that include motility disturbances and abdominal pain. Fructose malabsorption has been well documented in variable but similar proportions of healthy and populations with functional gastrointestinal disorders. Recent work into the expression of the main intestinal fructose transporter proteins highlight that our understanding of the mechanistic basis for fructose malabsorption and how it differentiates in gastrointestinal patients is incomplete. Until we have further mechanistic insight, restricting dietary fructose intake and other poorly absorbed short-chain carbohydrates and polyols remains an efficacious approach for managing functional gastrointestinal symptoms.
There is ample evidence to support that fructose malabsorption plays a role in inducing gastrointestinal symptoms in patients with functional gastrointestinal disorders (FGID). 1 The underlying mechanism of fructose absorption is thought to be due to an individual’s transporter function capability capacity, dictated by expression of the respective transporters. In this issue, a study by Wilder-Smith et al. 2 provides insight into the mechanism of fructose malabsorption and for the first time assesses whether a direct correlation exists between the expression of the main intestinal fructose transporter proteins and patients with FGID.
Fructose is a dietary monosaccharide slowly absorbed across the intestinal epithelium by carrier-mediated facilitated diffusion, which is an energy-independent process (Figure 1). The fructose carrier is a member of the glucose transport (GLUT) family of genes encoding for facilitative sugar transporters, of which there are two absorptive pathways. GLUT5 is a high-affinity fructose transporter found in the apical membrane on the luminal surface of small intestinal epithelial cells, is low-capacity and glucose-independent, and depends on a concentration gradient.
3
GLUT2 also has a facultative role and is a high-capacity, glucose-dependent fructose co-transporter. In addition to fructose, GLUT2 also actively transports glucose and galactose. GLUT2 is essentially located in the basolateral membrane; however, an apical GLUT2 pathway also exists. When glucose is transported by the Na+/glucose co-transporter (SGLT1), GLUT2 activation and insertion is promoted into the apical membrane.
4
Although less substantiated, there have been suggestions of other regulatory pathways including GLUT8
5
and GLUT7–GLUT12
6
also being involved in fructose absorption, for example in allowing accommodation of large amounts of fructose.
The main transporters involved with fructose absorption.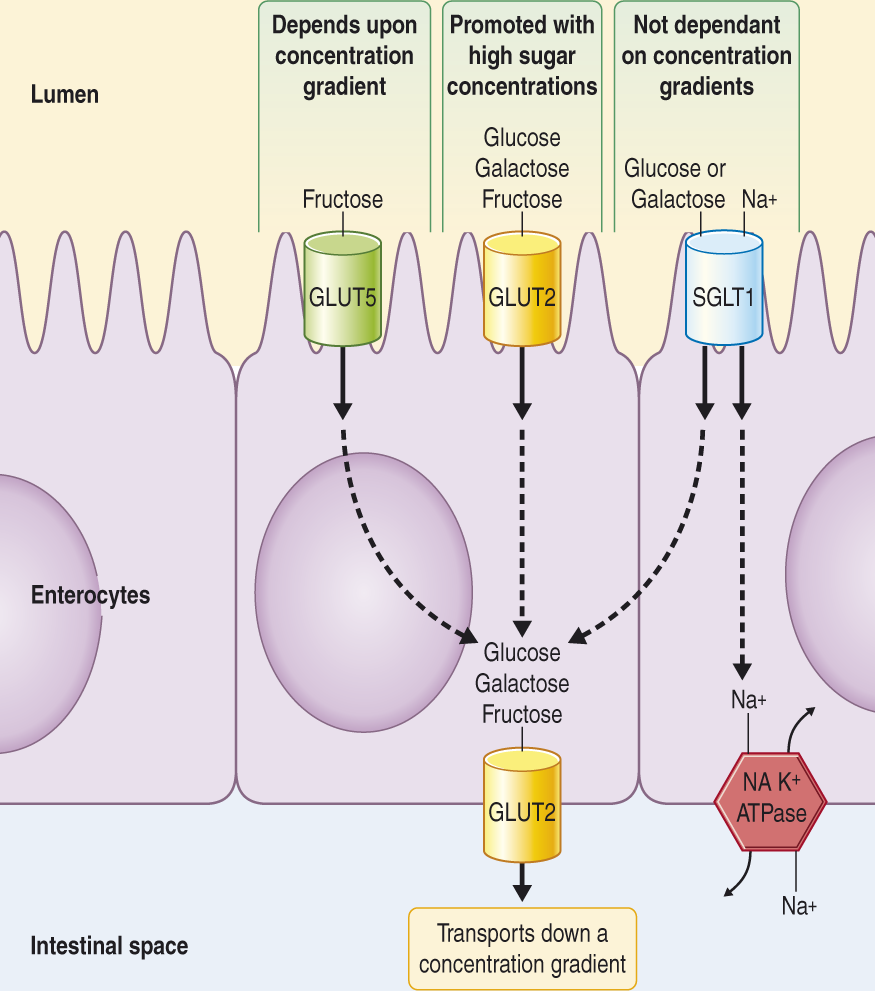
When fructose is incompletely absorbed (malabsorption), it can exert osmotic effects in the intestinal lumen, increasing water delivery and undergoing rapid fermentation by bacteria with consequent gas production. Although the prevalence of malabsorption is similar between subjects with FGID and healthy individuals, 7,8 the clinical ramifications are different. Malabsorption can become problematic for patients with FGID because their heightened visceral hypersensitivity leads to the increased gas and fluid content of the bowel being associated with bloating, distension, excessive flatus, and motility disturbances. 9,10 The mechanism underlying adult fructose malabsorption is unclear, although it has been hypothesized that a cause could be a change in the expression or activation of the transporter proteins.
Research into specific fructose transport and absorption has mostly been conducted in animal model studies and has shown that changes in GLUT expression correlates with altered fructose intestinal absorption. 11,12 Recent human data from infant 13,14 and diabetic 15 studies have supported this, where a reduced expression of GLUT5 were associated with high rates of fructose malabsorption. Moreover, fructose malabsorption is not associated with GLUT2 or GLUT5 mutations. 3
Factors that may influence the degree of absorption include rapid small intestinal transit time, small intestinal microbiota (bacterial overgrowth), developmental patterns, and varying glucocorticoid and thyroid hormonal roles. 6,16,17 High-fructose dietary intake has been shown to transiently up-regulate GLUT5 and GLUT2, with increases in mRNA and protein levels. 18 Intestinal fructose absorption is facilitated by co-ingestion with glucose due to the solvent drag and passive diffusion by the GLUT2 mechanism. 1,8 Increasing GLUT5 expression by the presence of luminal fructose or sucrose, co-ingestion of amino acids, or altering the insertion of GLUT2 into the apical membrane, such as in the case of diabetes, can also increase fructose uptake. 19 Sorbitol ingestion impedes fructose absorption. 20
The study in this issue provides the first evidence in human adults directly assessing expression of the main fructose transporters, GLUT5 and GLUT2 protein and mRNA in small intestinal tissue in adults with symptomatic fructose malabsorption in comparison with controls. 2 Eleven patients met the Rome III criteria for irritable bowel syndrome and reported increased symptoms during a positive fructose breath test. The control group (n = 15) were made up of age- and sex-matched asymptomatic subjects with a negative fructose breath test. The authors found that levels of mRNA in the duodenal mucosa did not differ significantly between the patient groups. This conflicts with previous thoughts that depressed or absent GLUT5 or GLUT2 protein levels could result in failure to transport fructose normally. The authors acknowledge that differences in membrane abundance, cellular activation or subcellular localization and expression of the transporters along different sites of the small intestine should be examined before excluding a role of the fructose transporters.
Given these results can be reproduced in larger samples, explanations other than differing GLUT5 and GLUT2 expression are needed for the manifestation of fructose malabsorption. For example, there may be other avenues of fructose absorption. The molecular effects of fructose on GLUT5 message and protein levels are not fully understood, for example there may be differences in the cis-acting elements and trans-acting factors. 3 Additional proteins may exist that are necessary for proper functioning of the GLUT5 transporter within the enterocyte membrane. 3 Because fructose absorption is stimulated by the presence of glucose in a dose-dependent fashion, there is a possibility of additional fructose transport mechanisms such as a transepithelial, phosphorylation-dependent glucose transport system. 13
Breath hydrogen tests have been advocated for the assessment of dietary fructose malabsorption. 8 One of the uncertainties regarding the diagnosis of malabsorption are that there are reasons other than inefficient fructose absorption behind a positive breath test result, such as rapid small bowel transit, excessive hydrogen-consuming bacteria, too few hydrogen-producing bacteria, or inadequate bacterial sugar fermentation. 1,20 There are also issues in the heterogeneity of methodologies used (e.g. ingested dose and concentration of fructose used), and gastrointestinal symptoms have poor correlation with breath hydrogen levels 21 and can appear independent of carbohydrate malabsorption. 22 Another issue is the cut-off value used for hydrogen/methane concentrations, especially given the known variability of methane production and possibility of inadequate hydrogen production. 23,24 Of note, this study employed a low cut off (>10 ppm from baseline) for methane production (although the authors did not state how many of their subjects were diagnosed as fructose malabsorbers according to hydrogen or methane criteria), which may lead to overestimating the prevalence of fructose malabsorption. Malabsorption has been shown to range from 5 g to more than 50 g, 8 and might be dose- and concentration-related. 25 Reasons for the absorptive capacity of fructose varying widely within the population remain unknown. Recently introduced semiquantification of breath hydrogen results has allowed for insight into degree of malabsorption. 23 This offers the opportunity for future mechanistic studies to focus on those depicting convincing malabsorption only, and to assess the differences between the likely distinct populations with low- and high-absorptive capacity. 23
The patients in the current study were more likely to get symptoms from the fructose ingestion, rather than from fructose malabsorption, 2 suggesting mechanism(s) other than or additional to their fermentation may be responsible for fructose induced symptoms in FGID. For example, it has been hypothesized that other poorly absorbed short-chain carbohydrates may affect the enteric nervous system via local osmolytic effects or the involvement of inflammatory mediators. 22 Undoubtedly the enteric nervous system has a complex role in responding to any food stimuli by varying secretion, motility, blood flow, and mucosal growth. 26
At 50 g, a dose well below the average daily fructose intake in the USA, about 60–80% of adults experience some form of malabsorption. 13 The main dietary sources of fructose include honey, apples, pears, and the increased use of high-fructose corn syrup. Other poorly absorbed short-chain carbohydrates and sugar alcohols have a similar fate to fructose in the distal small bowel and colon. Their effects are additive, distending the intestinal lumen by changing the volume of its contents. 20 Dietary restriction of these fermentable short-chain carbohydrates (also referred to as the low FODMAP diet) is a proven efficacious approach that is effective in the majority of patients with FGID, as recently reviewed. 26 Regardless of actual fermentation or breath hydrogen response, there is likely to be symptoms induced by fructose and the other FODMAPs because of their osmotic effect and slow absorption. 22
Contrary to previous hypotheses, the study by Wilder-Smith et al. demonstrates that fructose intolerance with malabsorption may not be secondary to changes in the duodenal expression of the fructose transporters or their production. Despite GLUT5 and GLUT2 being established as the primary fructose transporters, the connection between a biological mechanism for fructose transport and malabsorption remains elusive. These data add further support to the concept that the ability to absorb fructose in patients with FGID are not abnormal overall and that the sensitivity of the bowel to the change in luminal conditions induced by fructose malabsorption is the key difference rather than the malabsorption itself.