
Abstract
The treatment of GORD has been revolutionized by the introduction, in the 1980s, of proton-pump inhibitors as the mainstay of medical therapy and by the development of laparoscopic antireflux surgery which has definitively replaced open surgery. However, despite these major advances, many unmet therapeutic needs still persist and justify novel therapeutic approaches. The aim of this historical review is to recall the main discoveries in the treatment of GORD that have occurred during the last three decades and to discuss why some initially promising drugs or techniques have not translated into clinical applications. A careful analysis of these previous disappointing experiences should help to identify high priorities and better research programmes on the management of GORD.
Keywords
Introduction
Gastro-oesophageal reflux disease (GORD) is a highly prevalent disorder which impacts significantly on the quality of life (QoL) and work productivity of affected patients.1,2 For society the economic burden of GORD is extremely high, usually exceeding that of life-threatening diseases. During the last three decades, considerable progress has been made concerning the epidemiology and pathophysiology of GORD. In the meanwhile, the treatment of GORD has been revolutionized by the introduction of proton-pump inhibitors (PPIs) as the mainstay of medical therapy and by the development of laparoscopic antireflux surgery (LARS) which has definitively replaced open surgery. However, despite these major advances, many unmet therapeutic needs still persist and it must be acknowledged that initial enthusiasm for several novel therapeutic approaches has frequently been followed by disappointment. In this historical perspective, written in the context of the lifetime achievement award of one of the authors (JPG), we will aim briefly to review the main discoveries in the treatment of GORD that have occurred during the last three decades and how they have dramatically changed our therapeutic concepts concerning the management of this disease. We believe, however, that it is probably more informative for future research and development to emphasize the ‘flip side of the coin’ and to try to understand why some initially promising drugs or techniques have not translated into clinical applications.
Progress
In the 1970s, the expression GORD was not used as frequently as today – in practice the term, hiatus hernia, was more frequently employed, especially by surgeons, to refer to an entity mostly characterized by so-called ‘peptic oesophagitis'. In fact, the heterogeneity of the disease was recognized later with the development of rigorous endoscopic protocols applied during modern therapeutic trials, especially with the development of PPIs. Several international groups of experts3,4 have successively proposed new definitions of GORD, the last one being the Montreal definition (Figure 1) illustrating the different aspects of GORD and its complications. The finding that in the majority of cases there are no significant lesions (i.e. mucosal breaks) at oesophageal endoscopy implies that healing, although important for severe oesophagitis, cannot summarize by itself the aims of therapy in GORD.5,6 The relief of symptoms and a return to a normal QoL are actually the major aims of therapy and for the majority of reflux patients who present with nonerosive reflux disease (NERD), these are actually the only goals of treatment. The concepts of the natural history of GORD have been frequently disputed during the last few decades and some authors have proposed new paradigms to describe the heterogeneity of GORD as different entities with virtually no progression from one state to another. In fact, it is likely that GORD is a slowly progressive disease,
7
meaning that prevention of aggravation and complications remains an objective of treatment even if such an aggravation rarely occurs for the majority of patients, especially those with NERD.
The Montreal definition of GORD and the different clinical entities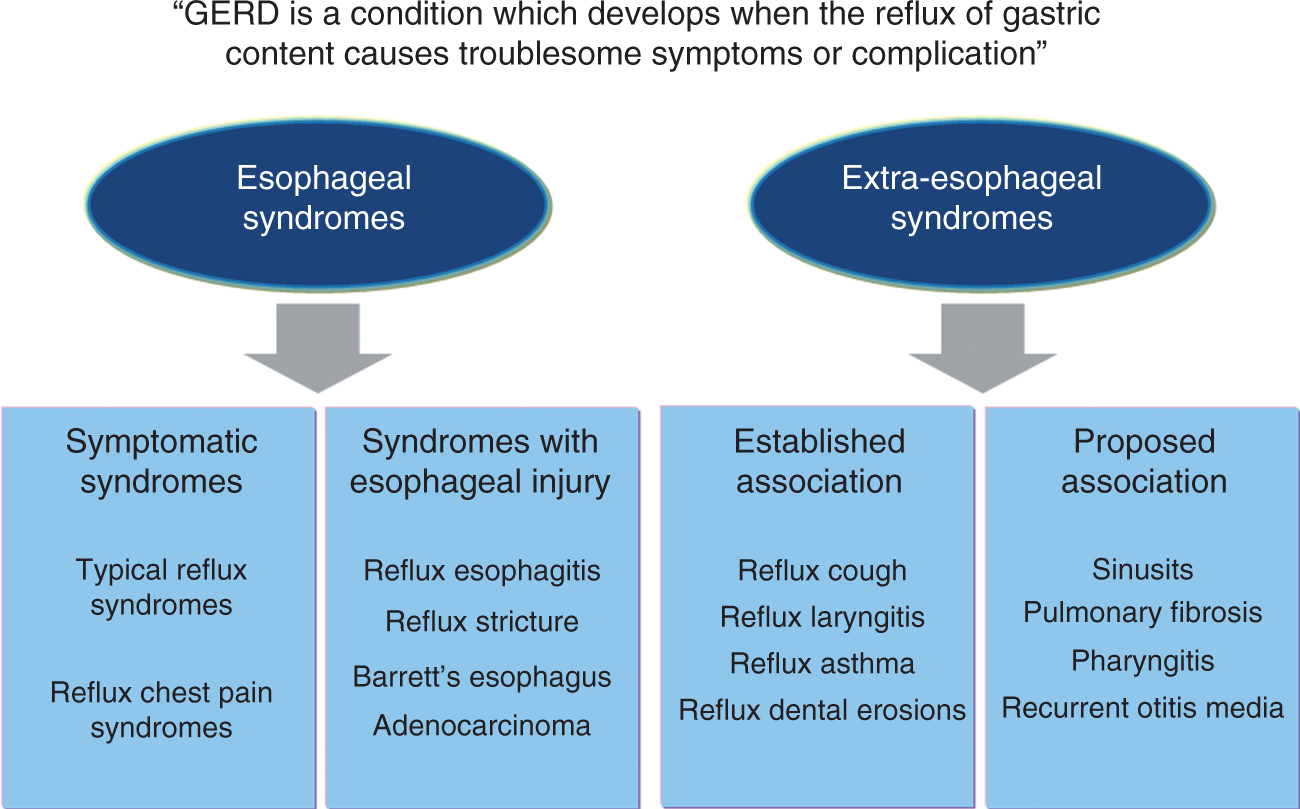
In theory, the ideal treatment should address the basic underlying mechanisms of the disease. Therefore the description by Dent et al. in the early 1980s 8 that transient relaxations of the lower oesophageal sphincter (TLOSRs) represent the main underlying mechanism of all reflux episodes, either acid or nonacid, is actually one of the major discoveries of recent decades and probably the one with the greatest potential for application to the investigation of novel drugs effective against GORD.
Proportion of oesophagitis healing and heartburn relief in patients with endoscopically proven erosive or ulcerative oesophagitis treated with proton-pump inhibitors (PPIs) or H2-receptor antagonists: a meta-analysis including 7635 patients
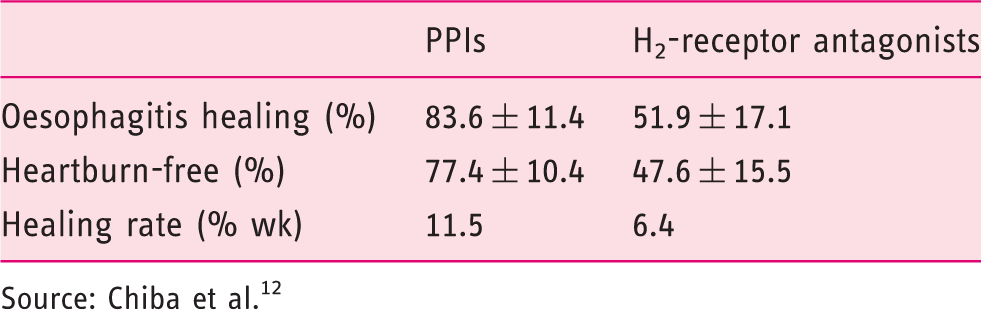
Source: Chiba et al. 12
The classic alternative to long-term maintenance with PPI therapy is antireflux surgery.
19
Although GORD is primarily a motility disorder, the role of anatomical factors in the impairment of the normal antireflux barrier has been continuously revisited since the 1980s to date. In particular, the role of hiatus hernia as a precipitating as well as an aggravating factor has been investigated thoroughly, especially with the development of modern investigation techniques such as high-resolution manometry.
20
Altogether, these studies have lent support to the paradigm of surgical treatment of GORD, because surgery is the only reflux therapy capable of correcting the underlying mechanisms responsible for reflux and, thus, definitively curing GORD (although not in all cases). Concerning the surgical procedures used to treat reflux, there has been a continuous trend during recent decades to simplify the surgical approach, abandoning complex surgery and resections in favour of more conservative and physiological procedures, namely fundoplication, either total or partial, which has become the standard for antireflux surgery. However, the revolution has come from the general development of laparoscopic surgery. Indeed, all the various components of standard antireflux surgery have been reproduced perfectly with LARS, leading to the same efficacy against reflux but with fewer complications, particularly incisional hernias.
21
The excellent and almost equivalent long-term results obtained with either esomeprazole maintenance or LARS were recently demonstrated by the LOTUS randomized trial showing that, in patients who initially responded to PPI therapy, approximately 90% remained in remission at the horizon of 5 years after enrolment in the study
22
(Figure 2). These results were clearly better than those of the SOPRAN study (a randomized comparison of omeprazole and open antireflux surgery) conducted a decade earlier, thus illustrating the progress achieved with both modern PPI therapy and LARS.
23
The LOTUS study results: comparison of remission rates (time-to-treatment failure, intention-to-treat analysis) of laparoscopic anti-reflux surgery (LARS) and esomeprazole maintenance therapy in patients initially responding to PPI therapy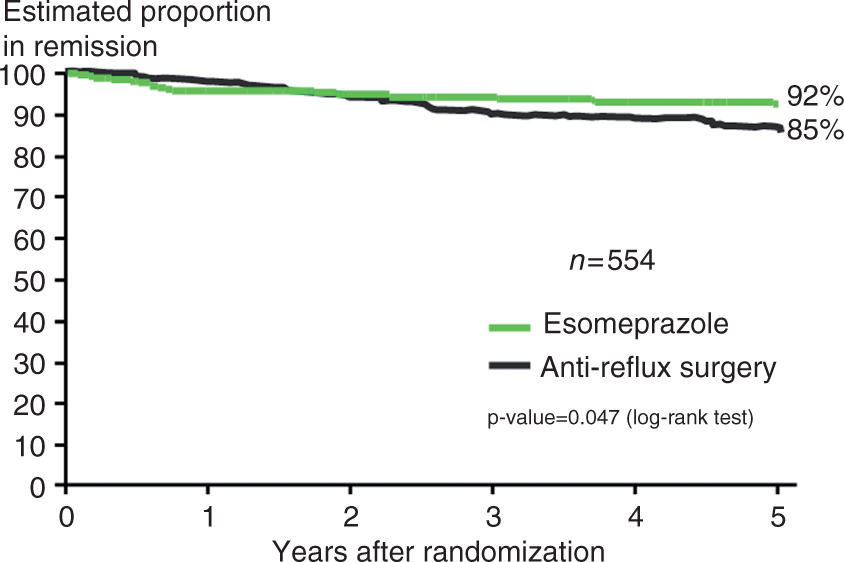
Disappointments
Despite the major progress made in both the medical and surgical management of GORD in recent decades, it should be realized that there are still many unmet needs that are not addressed by PPIs and LARS. 24 Approximately 20–30% of reflux patients, especially those with NERD 25 and/or extraoesophageal manifestations,26,27 are clearly poor responders to PPI therapy. Unfortunately for this group of patients, LARS is also less likely to achieve satisfactory results than in PPI responders. 28
The expression ‘refractory reflux symptoms’ seems more appropriate than ‘refractory GORD’ to characterize these patients, as pH-impedance studies have shown that the majority of PPI non-responder patients do not have reflux-related symptoms.29,30 In this respect, the Rome III classification has helped to clarify which clinical situations belong to the GORD spectrum (including NERD and hypersensitive oesophagus) and which do not. 31
After excluding patients without GORD and those in whom persistent symptoms are not reflux-related, there are multiple mechanisms potentially responsible for PPI resistance, as illustrated by Figure 3.32,33 Among these different mechanisms, the role of hypersensitivity is probably the most important one, especially for patients with normal acid exposure or functional heartburn. In practice, recent studies using pH-impedance monitoring have shown that persistent symptoms can be associated with acid and nonacid reflux in 10 and 30% of patients, respectively, while no association can be found in approximately 60% of cases.29,30,34 These data suggest that there is some room for improved inhibition of gastric acid secretion and reinforcement of the antireflux barrier.
Mechanisms potentially responsible for PPI resistance.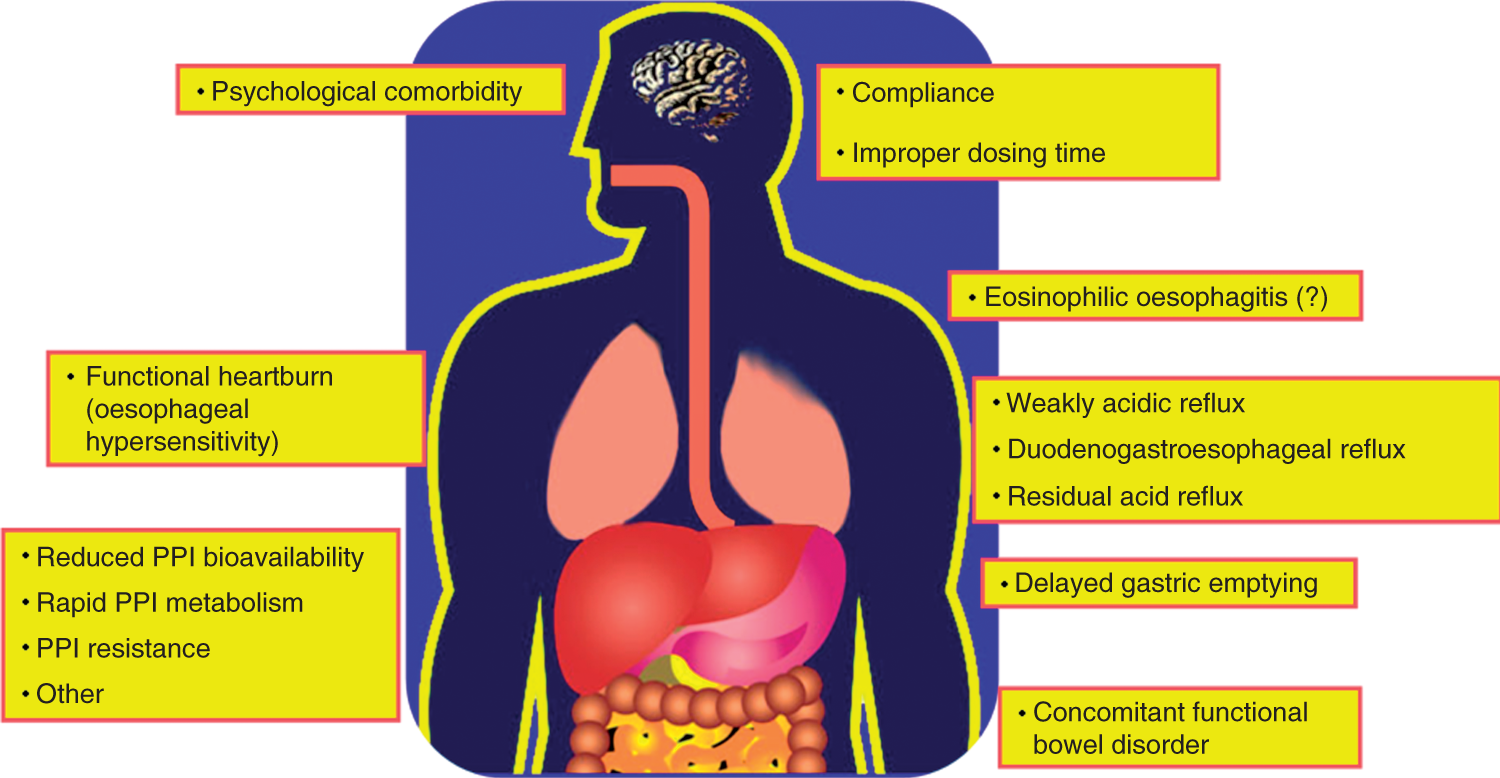
More potent acid suppression
In GORD, there is a significant correlation between the severity of oesophagitis and the duration of oesophageal acid exposure measured by 24-h pH monitoring. 35 It is, therefore, not surprising to observe a similar relationship between the acid inhibitory effect of a drug regimen and its therapeutic efficacy. 36 However, the antisecretory effect of a once-daily PPI regimen does not cover the whole 24-h period; indeed, although gastric pH is significantly increased after meals, it falls to an acidic level during the night. This phenomenon, sometimes called ‘nocturnal acid breakthrough’ 37 is directly related to the mechanism-of-action of PPIs, which behave as prodrugs requiring a protonation of their molecule after activation (by food) of the enzyme H+/K+‐ATPase (i.e. the gastric proton pumps) present in the parietal cells of the stomach. 17 Moreover, the plasma half-lives of conventional PPIs are relatively short (approximately 1.5 hours), therefore limiting the duration of exposure of the gastric proton pumps to the activated drug. One effective strategy to overcome these pharmacological limitations consists of dividing the total daily dose into two separate doses, given before breakfast and dinner, respectively. Another option is to double the dose of PPI, and it is generally assumed that such a strategy results in some additional improvement in 20–30% of poor responders. 32 Adding an H2-receptor antagonist to a PPI is also effective in reducing nocturnal acidity but this enhanced effect disappears after few weeks because of the development of a pharmacological tolerance to the H2-receptor antagonist molecule. Finally, all of these adaptations using currently available drugs have relatively limited efficacy and do not completely abolish gastric acidity.
For these reasons, new PPIs have been developed by pharmaceutical companies (for a review, see Bruley des Varannes et al. 17 ). For example, tenatoprazole has a long plasma half-life which translates into stronger and more sustained acid inhibition than a conventional PPI such as esomeprazole, 38 but the clinical development of tenatoprazole was abandoned for unclear reasons. Another conceptually original category of PPI is called potassium-competitive acid blockers (P-CABs) because of their mode-of-action through a reversible binding mechanism different from classic (irreversible) PPIs. In pharmacological studies these have shown a fast onset of action with a maximum effect obtained after the first dose, whereas classic PPIs need several days to reach their steady state effect. Moreover, P-CABs are active in the absence of stimulated acid secretion. However, despite their stronger and long-lasting acid-inhibitory effect, P-CABs were not more effective, against either symptoms or oesophagitis, when compared with a conventional PPI regimen using esomeprazole. 39 In addition, the P-CAB therapy resulted in an increase in liver transaminases, precluding any further clinical development.
Hence the question arises: Is there any future for more potent acid-inhibitory compounds in GORD? Although there may be some temptation for a positive answer, especially in conditions like Barrett's oesophagus, severe oesophagitis, or uncontrolled nocturnal symptoms, 40 one should refrain from too much enthusiasm. Indeed, correlation is not necessarily evidence of causality; for example despite a statistical correlation between gastric and oesophageal pH in general, it is less obvious that there is anything to expect clinically from increasing gastric inhibition. Indeed, with a double-dose PPI regimen, nearly all GORD patients have a normal oesophageal acid exposure. 41 Moreover, recent pH-impedance studies performed off- and on-PPI have clearly established that a residual oesophageal reflux is rarely the cause of persistent symptoms.30,42 Finally, in NERD patients, large controlled trials did not show any superiority of esomeprazole at 40 mg compared with 20 mg daily. 43 However, the benefit (or risks) of potent and prolonged acid suppression on the development of specific complications, such as the malignant transformation of a Barrett's metaplasia, cannot be completely excluded 44 and the results of long-term studies such as the ASPECT trial are eagerly awaited. The ASPECT trial is the biggest multicentre, randomized controlled clinical trial looking at the long-term chemoprevention effect of esomeprazole with or without aspirin.
TLOSR inhibitors
Transient lower oesophageal sphincter relaxations are not induced by swallowing, but involve a vago-vagal reflex triggered by gastric distension.8,45 TLOSR is considered to be mediated by nonadrenergic/noncholinergic neurons whose main neurotransmitters are vasoactive intestinal peptide and nitric oxide. Although many pharmacological compounds can reduce the occurrence of TLOSRs, only a minority of them are really available for therapeutic use in humans (Figure 4).
Diagram illustrating the potential targets for TLOSRs inhibition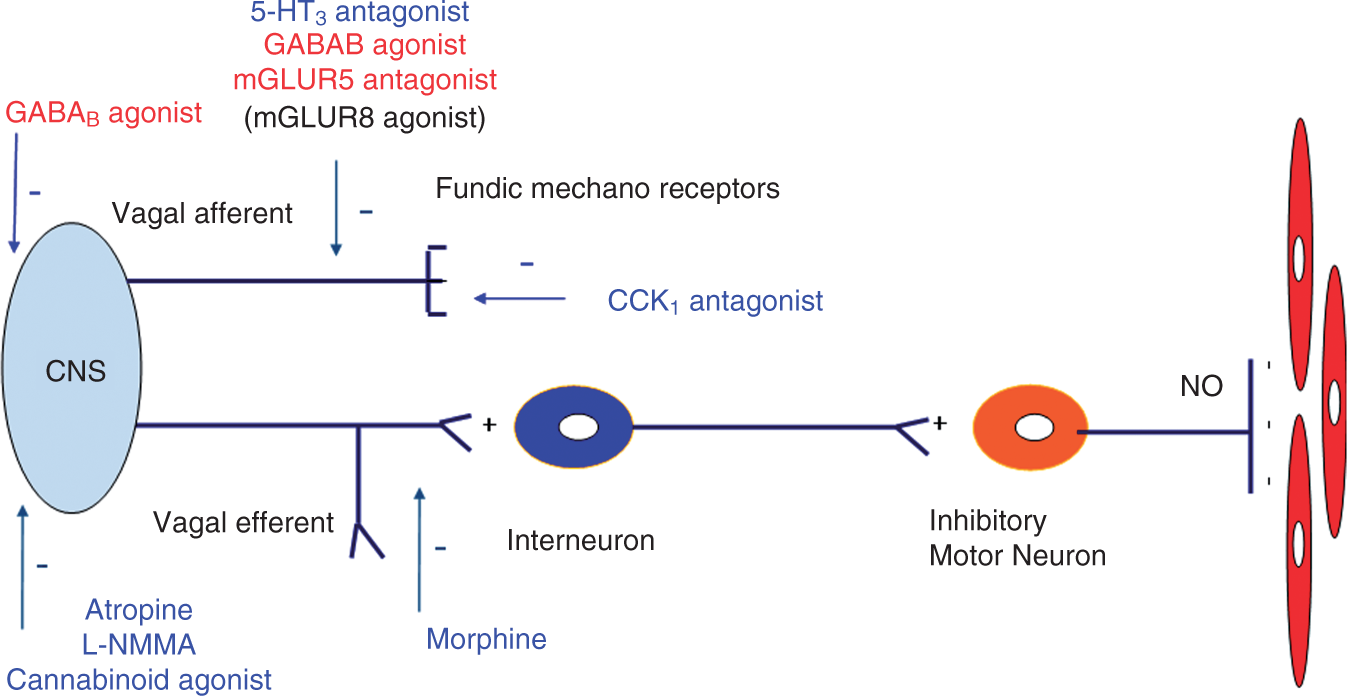
Gamma-aminobutyric acid (GABA) type B receptor (GABAB) agonists have been extensively studied in GORD. The only GABAB agonist currently available for human use is baclofen, a drug used for many years for the treatment of spasticity in neurological disorders. Baclofen has been shown to decrease TLOSR rate, reflux (both acid and nonacid) occurrence, and symptoms in patients with GORD.46–49 However, baclofen has a poor tolerability profile that limits its use in clinical practice and several pharmaceutical companies have developed other GABAB agonists. Arbaclofen placarbil, a prodrug of the R-isomer of baclofen, had a good tolerability profile but failed to demonstrate any benefit over placebo regarding the occurrence of heartburn, and its development has been abandoned. 50 Lesogaberan (AZD3355), a GABAB agonist, has been shown to increase basal lower oesophageal sphincter pressure, and to decrease both TLOSR rate and reflux episode occurrence, in patients with reflux symptoms refractory to PPIs. 51 Four weeks of treatment as an add-on therapy with PPIs in patients with refractory symptoms resulted in a low (although significant) 16% remission rate as compared with PPIs alone (8% remission rate). 52 Regarding its limited efficacy, and despite a good tolerability, the development of this compound has been abandoned.
Endogenous activation of metabotropic glutamate receptor 5 (mGluR5) is an important component of the pathway(s) triggering or regulating TLOSRs. ADX10059 is negative allosteric modulator of mGluR5 which demonstrated a significant effect on reflux occurrence and symptoms as a monotherapy,53,54 but failed to demonstrate a significant clinical efficacy as an add-on therapy in refractory GORD patients. 55 Moreover, longer term administration of ADX10059 resulted in an unacceptably high incidence of hepatic transaminase abnormalities and the further development of this compound has been halted. Other antireflux compounds, such as nitric oxide synthase inhibitors 56 and cannabinoid agonists (CB1 receptor agonists), 57 have shown their abilities to decrease the occurrence of TLOSRs and reflux events but are no longer being developed mainly because of tolerability issues.
Overall, the development of antireflux compounds during the past 5 years has been disappointing, as all have been abandoned despite initial encouraging results. Several reasons may explain these failures. First, the target population in clinical trials is not appropriate, as most patients with refractory symptoms do not have GORD-related symptoms. Most studies with antireflux compounds have included patients on the basis of symptoms rather than functional investigations (24-hour pH-impedance monitoring) which could identify patients who may benefit from the treatment. Moreover, since most of these patients have underlying functional disorders, 58 a high placebo response could be expected. Second, the antireflux barrier involves other components like oesophageal musculature, diaphragmatic musculature, and likely gastric and abdominal wall musculature as well. Therefore the role of TLOSRs may have been overestimated. Finally, these antireflux compounds do not address visceral hypersensitivity, which plays a major role in this context.
Last but not least, tolerability and safety issues are crucial. Neither patients nor physicians will accept poorly tolerated drugs for the treatment of a benign and chronic disorder such as GORD. Since these antireflux therapies act on neurons, either centrally or peripherally, the probability of experiencing side effects is high, unless a ‘TLOSR-specific’ pharmacological target is discovered, which appears so far to be quite improbable.
Hence, the future for such treatments appears to be uncertain. Ideally, these compounds should prove to be safe and well tolerated and should be tested in patients in whom GORD has been clearly identified as the cause of the persisting, bothersome symptoms.
Endoscopic treatments for GORD
At the end of the 1990s, a number of endoscopic procedures aimed at improving the antireflux barrier function of the lower oesophageal sphincter emerged. These new endoscopic techniques generally use one of three different approaches (for a review, see Arts et al. 59 ). Endoscopic gastroplication (EndoCinch) was the first endoscopic antireflux procedure to become commercially available. Several endoscopic suturing and knotting techniques were then developed, including the flexible endoscopic suturing device (Wilson-Cook), the Full-Thickness Plicator (NDO), and, more recently, the EsophyX technology which aims to reproduce the main components of antireflux surgery. 60 The Enteryx system consists of an injection in the lower oesophageal sphincter of a biocompatible, nonbiodegradable polymer, which solidifies when in contact with water and remains in place to restore barrier function. Other injection techniques, such as the placement of several implantable prostheses (e.g. the Gatekeeper repair system), have also been developed. The last type of endoluminal therapy is the Stretta procedure, which consists of delivering a radiofrequency energy current at the gastro-oesophageal junction. 61
All of the above techniques have been tested in animal models and are usually effective, although at different degrees, in significantly reinforcing the antireflux barrier; for example, most of them reduce the number of TLOSRs. In addition to its effect on the antireflux barrier, some studies have suggested that delivering a radiofrequency energy may also reduce oesophageal sensitivity to stimuli such as acid. 62 Therefore they were considered as attractive alternatives to long-term maintenance therapy with PPIs or surgery. Many reports of uncontrolled trials have been published at the early phase of development of these endoscopic techniques, suggesting successful outcomes in terms of symptom improvement and/or reduction of PPI use.
Unfortunately, when randomized trials and more prolonged follow-up studies have been conducted, the results have been less enthusiastic and finally the clinical development of these techniques has been abandoned, for reasons including, mainly, a lack of or insufficient efficacy (EndoCinch, Gatekeeper) or concerns about safety (Enteryx and Plicator). Today, only EsophyX 60 and Stretta61–63 are currently being performed in some centres, but the level of evidence for these procedures is generally considered to be relatively low and/or insufficient for them to become standard practice and approved for funding.
Analysing the reasons for such failed development is quite informative. Indeed, most of these techniques were developed by small companies without sufficient investment in rigorous clinical research, particularly well-conducted, prospective randomized, controlled trials. To the contrary, there has been a useless accumulation in the published literature of uncontrolled data concerning small series of poorly selected patients, treated with various procedures and devices, even when these refer to the same ‘brand’ of technique. The need for controlled studies, using a sham procedure as a comparator for new endoscopic treatment, has sometimes been difficult to convince to ethical committees. Some evaluation criteria, such as the ability to stop or reduce PPI in patients responding to this treatment is not necessarily the most relevant assessment. On the contrary, the potential of endoscopic techniques in well-selected indications remains to be investigated further. For example, in France, a national research programme is currently underway to evaluate the efficacy of the Stretta procedure in NERD patients whose symptoms are refractory to PPI. Similarly, a recent trial (unfortunately with an uncontrolled design) suggests that magnetic ring (LINX) placed around the lower oesophageal sphincter could be effective in reducing acid oesophageal exposure, reflux symptoms and use of PPIs. 64
Summary
The limitations of PPI therapy and LARS have justified new approaches, including more potent antisecretory drugs, TLOSR inhibitors, and endoscopic antireflux techniques. Unfortunately, all of these innovations have been less successful than initially expected and their development has been largely compromised or even abandoned. Many of these disappointing studies have, however, at least established important proofs-of-concept on which future research should capitalize in the hope of more successful outcomes.
Some directions for future research in GORD
The unmet therapeutic needs which persist in GORD clearly justify further research in such an important area of clinical medicine. In our opinion, some specific aspects should be considered with high priority in further research programmes on the management of GORD. These include methodological improvements in therapeutic trials, better pathophysiological knowledge, especially concerning refractory symptoms, and, last but not least, an appropriate strategy to maintain sufficient motivation and support from industry and public research agencies.
Performing better trials with already-available therapies and new treatments is the first priority. That means well-designed, prospective, controlled studies, conducted with well-selected patients, representing the real target for therapy. For example, several trials on the effect of PPI in NERD have been polluted by patients who did not have the disease, as shown by a recent meta-analysis. 65 New tools such as pH-impedance monitoring may help in this selection, as suggested by recent surgical studies 66 which, however, need confirmation by randomized trials. This also holds true for conditions such as extraoesophageal manifestations of reflux (e.g. asthma, cough) where the potentially responsive population remains to be identified.26,27,67 Without such an appropriate selection, there is a huge risk of missing a true beneficial effect simply by diluting it in a large population sample containing more nonresponders than actual responders. In this context, the search for new clinical and biological markers should be encouraged as well as the identification of potentially important confounding variables which need specific adjustment in multivariate statistical analyses (e.g. the role of obesity on the pharmacokinetics of drugs 68 ). Generally speaking, research priority should focus on the group of PPI nonresponders, even if alternatives to long-term maintenance drug therapy deserve continuous investigations in PPI responders.
Oesophageal hypersensitivity is the second-most priority because it is now clear that it represents the main mechanism of refractory symptoms in GORD.
33
Indeed, most patients with refractory symptoms have a number of reflux events within the normal range.
30
oesophageal hypersensitivity has been demonstrated in many subgroups of patients (Figure 5) with refractory reflux symptoms, especially patients with NERD, hypersensitive oesophagus,
69
and functional heartburn.
32
The mechanisms underlying oesophageal hypersensitivity remain largely unknown, but probably involve some degree of mucosal integrity alteration (e.g. dilated intercellular spaces) as well as peripheral and central sensitization. The role of a generalized visceral hypersensitivity is further supported by the high prevalence of functional digestive disorders
70
which represent a major condition associated with PPI failure. The concept of oesophageal/visceral hypersensitivity in refractory reflux symptoms supports the development of pain modulators in these patients. In this context, a recently reported trial
71
showing that 20 mg citalopram daily for 6 months is effective in a group of adequately selected patients with a hypersensitive oesophagus appears encouraging.
The respective roles of acid and hypersensitivity in the different phenotypes of GORD and their response to proton pump inhibitors.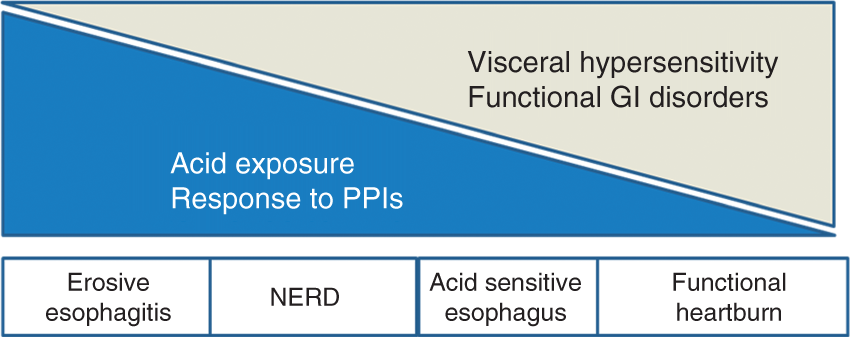
Identifying new targets for drug development is another important area for future research. Beyond PPIs and besides inhibitors of TLOSRs or pain modulators, some ‘exotic’ areas of research deserve further exploration. For example, the pathophysiological mechanisms by which overweight and obesity increase the risk of reflux and oesophagitis 72 are probably far more complex than pure mechanical effects. 73 Similarly the role of cytokines in the development of oesophagitis and its complications74,75 seems important, suggesting that reflux oesophagitis cannot simply be reduced to a caustic effect of acid on the oesophageal mucosa. Also, the role of microbiota is important in many GI disorders and needs to be investigated further in GORD. For example, we have shown that induced colonic fermentation is able to trigger the occurrence of TLOSRs and reflux. 76 More recently, specific microbioma types of the distal oesophagus have been shown to be associated with intestinal metaplasia and oesophagitis. 77 Finally the role of genetic versus environmental factors 78 should be further explored and may ultimately contribute to a better understanding of the pathophysiology of GORD as well as an improvement in the classification of the different phenotypes associated with reflux.
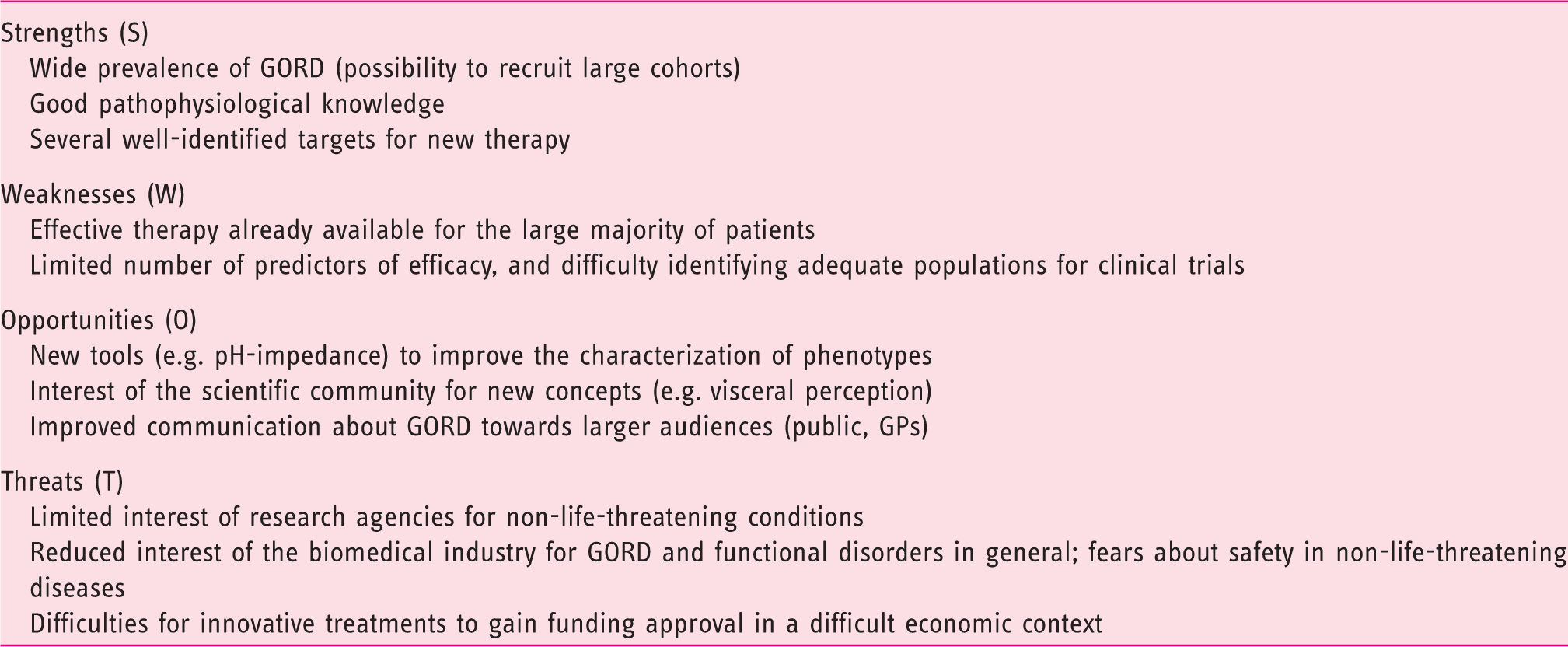
A tentative (SWOT) strategic analysis of potential for research in GORD
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
JPG has received consulting fees from Shire, Given Imaging and Mauna Kea Technology. FZ has received consulting fees from Addex Pharma SA, Xenoport, Shire Movetis, Reckitt Benckiser, Abbott, Pfizer, Given Imaging, Cephalon and Almirall, and lectures for Astra-Zeneca and Janssen. SBV has received consulting fees from Shire, Given Imaging, Teva, Almirall, Biocodex and Mayoli Spindler.