
Abstract
Objective:
To evaluate the clinical efficacy of transcutaneous electric nerve stimulation in the treatment of postoperative knee arthroplasty pain and to relate these results to the stimulation parameters used.
Data Sources:
PubMed, Pedro and Web of Knowledge were systematically screened for studies investigating effects of transcutaneous electric nerve stimulation on postoperative knee arthroplasty pain.
Review Methods:
Studies were screened for their methodological and therapeutical quality. We appraised the influence of the stimulation settings used and indicated whether or not a neurophysiological and/or mechanistic rationale was given for these stimulation settings.
Results:
A total of 5 articles met the inclusion criteria. In total, 347 patients were investigated. The number of patients who received some form of transcutaneous electric nerve stimulation was 117, and 54 patients received sham transcutaneous electric nerve stimulation. Pain was the primary outcome in all studies. The stimulation settings used in the studies (n = 2) that reported significant effects differed from the others as they implemented a submaximal stimulation intensity. Stimulation parameters were heterogeneous, and only one study provided a rationale for them.
Conclusion:
This review reveals that an effect of transcutaneous electric nerve stimulation might have been missed due to low methodological and therapeutical quality. Justifying the choice of transcutaneous electric nerve stimulation parameters may improve therapeutical quality.
Introduction
Rationale
Studies on the effectiveness of transcutaneous electric nerve stimulation (TENS) to relieve pain after knee arthroplasty differ in whether or not they find it to be efficacious. One reason might be that they have used different stimulation parameters, and some may be ineffective. A review, focusing on methodological quality of randomized controlled trials of TENS, identified different sources of bias that may lead to an underestimation of the treatment effect. 1 This review revealed that the main areas of concern were the location of application, the intensity and the duration of TENS. However, none of the included studies investigated TENS in patients with knee arthroplasty.
The number of osteoarthritis patients undergoing knee arthroplasty has increased dramatically in the last decades. 2 This trend will probably persist in the coming years given the worldwide demographical changes, the growing incidence of overweight and obesity and the wish of elderly persons to maintain an active lifestyle. 2 Knee arthroplasty is a procedure often accompanied with high levels of postoperative pain, which may hinder functional rehabilitation. Therefore, an effective pain management is of major importance to achieve good rehabilitation outcomes. 3
TENS is a non-pharmacological, inexpensive and safe form of postoperative analgesia treatment 4 for which beneficial effects have been described after different surgical procedures.5–7 Its analgesic effects are attributed to mechanisms related to the “gate control” theory of pain 8 and, as proven more recently, pathways involving the central nervous system. 9
Objectives
The aim of this systematic literature review is to evaluate the clinical efficacy of TENS in the treatment of postoperative pain in knee arthroplasty patients and to relate this to the stimulation parameters used. All studies were screened for their methodological quality. In addition to this, we assessed the fidelity criteria for application of TENS for pain in clinical trials (i.e. potential sources of bias that may lead to underestimation of treatment effects), as proposed by Bennett et al. 1
Materials and methods
Eligibility criteria
Trials studying the effect of TENS on pain, range of motion (ROM) or function following knee arthroplasty were considered.
Information sources
PubMed, Pedro and Web of Knowledge were systematically screened. Additional studies were identified by scanning the reference lists of included articles (last search in November 2013).
Search
We used the following search terms to search both databases: post-surgery knee arthroplasty, after operation knee arthroplasty, knee replacement, knee arthroplasty, knee prosthesis, TENS, transcutaneous electrical nerve stimulation, percutaneous electrical nerve stimulation, pain, function and ROM (see Appendix 1 for full search strategy). The following language limits were applied: English, French or Dutch. No publication date or status restrictions were imposed.
Study selection
Eligibility assessment was performed independently by two investigators (D.B. and Y.V.). Disagreements between reviewers were resolved by consensus.
Data items
Information was extracted from each included study on the following: study set-up (including description of study arms, medication being used as co-intervention), type of intervention (including requirements for application of TENS for pain in clinical trials, as proposed by Bennett et al., 1 active area of the electrode, wave form, number of electrodes, location of the electrodes, pulse duration, stimulation frequency, intensity, duration of one treatment session, period of treatment) and type of outcome measures. As a supplementary criterion, we screened for a neurophysiological and/or mechanistic rationale for the stimulation parameters that were used.
Risk of bias in individual studies
The methodological quality of the included studies was assessed by two independent investigators (D.B. and I.B.), using the methodology checklist for randomized controlled trials of the National Institute for Health and Clinical Excellence (NICE) (http://www.nice.org.uk/guidelinesmanual; last checked 22 February 2013). This checklist focuses on potential risks of selection, performance, attrition and detection bias.
Results
Study selection
Five studies met the inclusion criteria (Figure 1).10–14

Study selection flowchart.
Study characteristics
The study characteristics are shown in Table 1. All studies were prospective randomized trials. Two of the included articles were from the same research group and report probably on the same cohort.11,12 They both have used the same or comparable outcome variables and interventions. Walker et al. 12 described a supplementary intervention arm treated by a continuous cooling pad (CCP). For the scope of this review, only the TENS-related results were extracted.
Study characteristics.

TENS: transcutaneous electric nerve stimulation; BEQ: bioequivalent scale; CCP: continuous cooling pad; CPM: continuous passive motion; EAD: equianalgesic dose (1.0 mg intramuscular morphine sulfate); ns: not specified; THA: total hip arthroplasty; TKA: total knee arthroplasty; PCA: patient-controlled analgesia; VAS: visual analog scale; ROM: range of motion.
Participants
In total, 347 patients were investigated (Figure 2; Table 1). The total number of patients who received some form of TENS was 117, and 54 patients received sham TENS. One study included participants following either total hip replacement or knee arthroplasty (n = 107, of which 43 received TENS and 22 received sham TENS) but did not provide specific data for knee arthroplasty patients solely 10 (Table 1).

Visualization of study arms with number of subjects of the five included studies. *Also implemented other study arms that were not included in this review.
Intervention
Two articles described the effect of TENS in three comparable treatment groups: continuous passive motion (n = 12), continuous passive motion in combination with “subthreshold” TENS (n = 18) and continuous passive motion in combination with “sensory threshold” TENS (n = 18).11,12 Both articles reported effects on active knee flexion, the use of analgesics, the length of hospital stay, 12 and visual analog scale (VAS) for pain. 11 Breit and Van der Wall 13 studied the effect of TENS in combination with patient-controlled analgesia. Their study contained three study arms: patient-controlled analgesia (n = 22), patient-controlled analgesia combined with TENS (n = 25) and patient-controlled analgesia combined with sham TENS (n = 22). Stabile and Mallory 10 studied the effects of TENS (n = 43) compared to sham TENS (n = 22) or treatment with intramuscular Dilaudid (hydromorphinone HCl) (n = 42). Wanich et al. 14 studied a patented device called “Deepwave” which sends a modulation of two high-frequency (HF) currents between two electrodes that comprised microneedles. This study involves an experimental group (n = 13) and a sham group (n = 10).
Outcomes
Pain was used as the primary outcome variable in all included studies and was quantified by VAS11,13,14 and/or analgesic consumption.10–14 In one study, VAS data could not be interpreted because of missing data and inconsistencies. 13 Analgesic consumption was quantified by standardized medication intake using a parenteral and oral dosage equivalence system 12 or a bioequivalent scale (BEQ). 11 These equivalence systems were devised for the narcotic medications used by the patient sample and based on a comparative dosage of injectable narcotic medication. Other quantification methods used for analgesic consumption were dose of spinal anesthesia, 13 dose of sedation 13 and amount of postoperative morphine.10,13
Risk of bias within studies
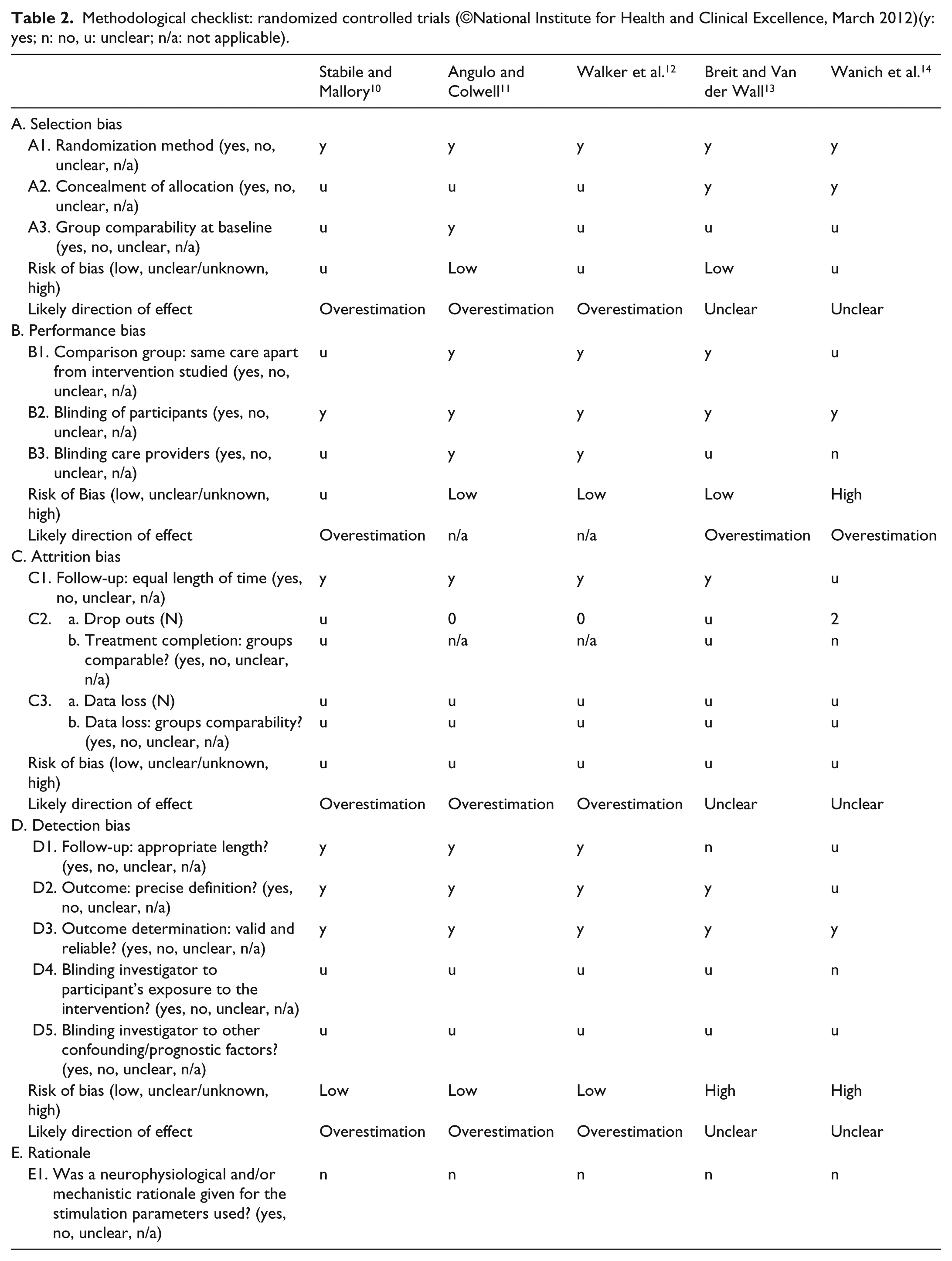
Overall, methodological quality of the included studies was poor and risk of bias was present with a likely overestimation of the treatment effect (Table 2). All studies involved a relatively low sample size (N = 25 or lower per intervention arm), and none of the studies reported a priori sample size calculation or power analysis. There was a lack of information regarding the number of subjects that were excluded or dropped out. One study mentioned the withdrawal of two subjects from the experimental group because they were unwilling (due to fatigue) to comply with twice daily treatments. 14 Only one study registered adverse effects. 10 Although participants of all included studies were randomly assigned to comparison groups, only two studies provided some information on the randomization procedure.13,14 All studies involved a control group which did not receive any form of TENS. Two included articles mentioned blinding of therapists.11,12 However, in the study by Angulo and Colwell, 11 therapists were only blinded to the intensity of TENS being applied (40 mA in group 1 vs 14 mA in group 2) by hiding the intensity indicator with adhesive tape, but they did not mention whether they were blinded for treatment allocation. Walker et al. 12 mentioned that therapists were blinded for group allocation and outcome measurements. In all studies, the investigators attempted to blind the participants for the study interventions.10–14 Patients were blinded by either hiding the intensity indicator with adhesive tape, 11 by leaving the intensity at zero, 14 by placing unconnected wires under the blankets so that the machine appears connected to the electrodes 13 or by using TENS units without power supply (no batteries). 10 Walker et al. 12 mentioned blinding of patients “as to parameters under study” without further specification. In two studies, participants who had knowledge of or had previously used a TENS machine were excluded for participation.11,13
Methodological checklist: randomized controlled trials (©National Institute for Health and Clinical Excellence, March 2012)(y: yes; n: no, u: unclear; n/a: not applicable).
Application fidelity
None of the included studies match all the requirements for TENS application as stated by Bennett et al. 1 (Table 2). One study 12 (80%) did not report if TENS was used over the area of pain or segmental area and only 210,14 (40%) used TENS at an adequate intensity. Three studies11,13,14 (60%) mention that TENS is applied for at least 30 min.
Rationale
No study provided a neurophysiological or mechanistic rationale for the stimulation parameters used.10–14 Although Wanich et al. claimed to use a special wave form which is based on a new technology that is supported by the theory of hyperpolarization for inhibiting pain transmission, the authors did not provide reference to scientific evidence for this. They combined two HF electronic waveforms with the aim of interrupting sodium/potassium ion exchange across the membrane of the C-fiber, inhibiting cell wall from changing polarity and impeding transmissions of pain impulses. 14 Wanich et al. presented some information concerning the electrodes that comprised microneedles to facilitate the delivery of the current through the skin but also did not provide any reference to scientific proof for this assumption.
Results of individual studies
Two studies found a beneficial effect of TENS on pain.10,14 Both studies implemented a submaximal stimulation intensity, perceived as “strong but comfortable” (Table 3). None of the other studies used this intensity setting. While Wanich et al. set this parameter after the surgery, Stabile and Mallory 10 preoperatively obtained values for pulse width and frequency that gave the patient this strong sensation. Wanich et al. applied the TENS twice daily for 30 min, but Stabile and Mallory did not report on the duration or the frequency of a treatment session. In both studies, HF TENS was used. Wanich et al. 14 started the intervention at 36/48 h post-surgery after the removal of the Dilaudid/bupivacaine epidural, but they did not report on opioid intake or other pain control as an adjunct for the electrical stimulation. However, they report a trend towards a decreased opioid use in the experimental group, but it is not clear how and when this opioid use was provided and registered. They also found a significant decrease in VAS pain scores (p < 0.05) in the experimental group (decrease in VAS from 28/100 to 19/100) compared to the control group (decrease in VAS from 26/100 to 25/100). In contrast, the patients in the study of Stabile and Mallory 10 started the TENS “as soon as the patient awoke from surgery and complained from pain,” and they were offered Dilaudid as an adjunct for pain control. In the latter study, the postoperative pain control, determined by the amount of milligrams per day of Dilaudid on the first, second and third postoperative days, was significantly lower in the experimental and placebo group than in the control group. This finding was supported by the subjective opinion of the patients from the experimental and placebo groups: 86% of them felt that “TENS helped in the management of their discomfort and lessened the need for the narcotic medication.” However, the placebo effect was not significant.
TENS current settings.

TENS: transcutaneous electric nerve stimulation; d: pulse width; f: pulse frequency; ns: specified.
In contrast, three studies did not show that TENS or sham TENS significantly altered analgesia consumption.11–13 They all applied TENS continuously 24 h/day. Two of these study reports were, as previously mentioned, from the same research group. They used a stimulation frequency of 70 Hz and fixed-pulse amplitudes of 14 mA (below sensory threshold) and 40 mA (above sensory threshold).11,12 These intensities were based on a preoperative test of 13 subjects in which the “mean level of the sensory threshold” (i.e. 21 mA) and the “mean maximum comfortable sensory stimulation below the level of visible muscle contraction” (i.e. 40 mA) were determined. No significant differences in percentage decrease of VAS scores for pain were demonstrated between the “subthreshold” and the “sensory threshold” TENS treatments. 11 No clear rationale was given for this procedure to obtain the stimulation parameters, and no information was given concerning the VAS scores of the control group.
TENS parameters
A wide range of TENS parameters were used in the included studies (Table 3). Three studies reported the number of electrodes used: two11,14 or four. 13 Four studies reported on the location of the electrodes: one10,11,14 or two electrodes (above and beneath the knee) 13 on the medial and lateral aspects of the operated knee. One study did not provide any information on the number, type or placement of the electrodes. 12 The electrodes used by Wanich et al. 14 were made to facilitate the delivery of the feed signals through the skin by 1014 microneedles that are 0.74 mm in length within a 2.5-in-diameter sterile patch. One study applied stimulation intensities that were controlled by the patient, 13 but they were not registered or reported. One study did not provide information on pulse width and frequencies. 13 TENS was used continuously during the first postoperative 24 h 13 or the first three postoperative days.11,12 One study did not specify the duration of the TENS treatment. 10 Wanich et al. 14 used a premixed modulated envelope of two HF electronic waveforms.
Discussion
In this review, we aimed to evaluate the clinical efficacy of TENS in the postoperative treatment of knee arthroplasty. We included five study reports of which two showed a positive effect of TENS on analgesics consumption 10 or subjective measures of pain. 14 These were the only studies that used a stimulation intensity that was perceived as “strong but comfortable,” which is in accordance with latest guidelines. 1 However, all included articles showed poor methodological quality with a risk of overestimation of the effects. An important finding of our review is the lack of articles providing clear, transparent and sufficiently detailed information which is in line with the conclusions of a previous review. 1 In the future, TENS studies should follow the international standards for reporting randomized controlled trials, such as provided by the Consolidated Standards of Reporting Trials Group (CONSORT). 15
When assessing the quality of the included studies, we took additional criteria into account that were previously presented by Bennett et al. 1 and that are related to application fidelity. Our findings are in line with Bennett’s results: the quality of the TENS interventions that are used in the included studies show multiple areas of concern that may underestimate the effects of TENS. The criteria proposed by Bennett et al. 1 may be used for judging sources of potential bias related to TENS application, but their checklist does not take into account the rationale that researchers have been using to justify their choice of stimulation parameters. Hoogeboom et al. 16 state that the rationale for choosing an intervention (including its parameters) and whether this is based on good scientific evidence may add to the quality of an intervention. A study can be perfectly set up methodologically, but if the quality of the intervention is weak, study results are susceptible to bias. Especially for non-pharmacological therapies, justifying the choice of the therapy (including its components such as intensity, frequency) is an important feature of evidence-based practice. Therefore, when interpreting the results of the included studies of our review, we did not only consider the stimulation parameters but also the rationale for using them. We think that this is an important asset of our review. Only one study in this review provided rationales for the stimulation settings being used, but none of them were scientifically empowered. 14
Knowing the rationale for the procedure of preoperatively assessing TENS settings that will be used for TENS treatment after surgery would give more insight in the decision-making and reasoning process of the researchers.10–12 In this context, it should be noted that sensation alterations exist in the skin following knee arthroplasty, 17 and thus, preoperatively assessed parameters corresponding to “strong but nonpainful” 10 or “maximum comfortable” 11 stimulation may not always reflect the postoperative sensations.
Previously, placebo TENS has shown similar effects to active TENS, 18 and therefore, it is essential to incorporate a well-constructed sham TENS device that not only blinds the patient but also the investigator. 19 Especially, the treatment allocation should be concealed for the outcome assessors in order to avoid bias. 1 All of the included studies of our review tried to blind the patients in a way that therapist could be aware of the treatment allocation, that is, they were not blinded for the treatment (e.g. pulling out batteries or using unconnected wires).10,13 Therefore, a separate blinded investigator is needed to assess the outcomes. Recently, a new sham TENS device has been proposed that allows blinding the investigator while delivering a placebo treatment. 19 This device delivers stimulation for 30 s and gradually decreases to 0 over the next 15 s.
All of the included studies took medication intake as an outcome measure. An important feature to take into account when interpreting TENS results is the use of analgesics and more specifically opioids because TENS-induced analgesia also involves opioid receptors.20,21 Therefore, a possible interaction between TENS and opioid use may exist. Moreover, low-frequency (LF) TENS seemed ineffective in rats that were made previously tolerant to opioids. 22 So, LF TENS might be ineffective in patients using opioids due to analgesic tolerance. In all of the included studies, TENS has been used following or during the use of opioids. However, all studies except one 13 reported the use of HF TENS. In contrast, instead of hindering each other’s effect, a combination of TENS with pharmacological agents has previously been proven to enhance the effectiveness of the treatment.23,24 For example, clonidine is a pharmacological agent that produces an alpha-2 adrenergic–mediated anti-nociceptive effect, because of which its potency is increased when it is combined with TENS. 24 Consequently, a lower dose of the drug could produce a similar degree of analgesia, thus diminishing the risk of drug-related side effects.
The three studies that did not find an anti-nociceptive effect of TENS applied TENS continuously 24 h/day.11–13 In this respect, it is interesting to note that previously it has been proven that both HF and LF TENS may produce analgesic tolerance.25–28 However, this occurs through different pathways.29–31 Since burst TENS is a combination of LF TENS and HF TENS, it may generate a combination of analgesic action of both LF TENS and HF TENS and by doing so delaying or limiting analgesic tolerance. Thus, in the future, it would be interesting to investigate the analgesic effects of burst TENS following knee arthroplasty.
Two of the three studies that did not find a significant effect of TENS used continuous passive motion during the hospitalization period for 20 h/day.11,12 Besides the fact that continuous passive motion has not been shown to provide added value to the rehabilitation outcomes, 32 the long period of continuous passive motion that is applied in the studies may initiate central sensitization. 33 By continuously activating polymodal nociceptors and stimulating the release of pro-inflammatory cytokines, the continuous passive motion may initiate central sensitization resulting in an altered responsiveness to electrical stimuli. This may lead to an underestimation of the TENS effects.
Our study has several limitations. We a priori set the eligibility criteria, including the language restrictions for including studies. We think that by adding French and Dutch alongside English, we increased the chance of getting a comprehensive search result. However, we are aware that language restriction may increase the risk on influencing the effect estimates. Nevertheless, a study of Jüni et al. 34 showed that excluding trials published in languages other than English has generally little effect on summary treatment effect estimates. As mentioned previously, the overall quality of the included studies (methodologically and therapeutically) was poor, and this may lead to substantial over- or underestimations of the reported effects. Publication bias may account for some of the presented effects. Two studies were from the same research group. They both reported the same or comparable study groups, outcome measures and used the same TENS settings. Therefore, it cannot be ruled out that these studies should be treated as one. Due to the low number of studies that report effects of TENS in this specific population and due to the incomplete reporting of the study designs, interpretation and applicability of our review may be restricted. However, based on the findings of our review, we propose some advices to take into account when using TENS in a clinical setting: (1) the intensity of the current should be perceived as strong but comfortable, (2) HF TENS should be used, (3) therapists should be aware of the rationale for each TENS parameter and (4) burst TENS may combine analgesic effects of HF TENS and LF TENS. We also propose some recommendations when designing TENS studies in hospitalized knee arthroplasty patients: (1) CONSORT recommendations should be incorporated when designing and reporting trials; (2) when applying TENS, the fidelity criteria as proposed by Bennett et al. 1 should be taken into account; (3) the use of a sham TENS device as proposed by Rakel et al. 19 allows blinding of the investigator while delivering the placebo treatment, and thus, a separate blinded investigator is not needed to assess the outcomes; (4) the use of burst TENS should be considered since this may produce a combination of the mechanisms of action of both LF and HF TENS and (5) interactions between TENS and medication is a promising study field that may help to provide a more effective pain management with less drug-related side effects.
We conclude that the majority of the included studies point out that TENS has no analgesic effect in knee arthroplasty patients. However, the two studies that used TENS intensities as advised by the recent scientific literature did report significant analgesic effects. All studies showed poor methodological quality and are heterogeneous in study design and outcome. Supplementary well-designed studies are needed to determine whether TENS can counter postoperative knee arthroplasty pain.
Footnotes
Appendix 1
Declaration of conflicting interests
The authors declare that they have no competing interests.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.