
Abstract
Hypoglossal nerve palsy is a rare complication following general anesthesia, typically observed after prolonged surgical procedures. This case report discusses a 27-year-old male patient with no significant past medical or surgical history who developed isolated right-sided hypoglossal nerve palsy following an uneventful septoturbinoplasty surgery. The hypoglossal nerve, vulnerable to injury during intubation due to its anatomical course, may result in symptoms such as swallowing difficulties, speech impairment, and tongue deviation. Prompt identification is essential to differentiate it from other serious conditions, such as stroke or airway obstruction. Treatment typically involves steroid therapy, with most cases showing improvement within months. Following oral prednisolone treatment, the patient experienced relief in tongue movements after 1 month, with further partial improvement after 2 months, leading to full clinical recovery by the end of the second month. Careful management during intubation and surgical procedures can help prevent this complication. This case underscores the importance of vigilance and proper management in minimizing the risk of hypoglossal nerve palsy during perioperative care.
Introduction
After undergoing general anesthesia, patients may experience common postoperative symptoms such as throat discomfort, dryness, and difficulties with swallowing and speech, typically managed through postoperative care. 1 However, in rare instances, these symptoms may signify underlying cranial nerve injury. 2
The hypoglossal nerve emerges from the medulla and exits the cranial cavity via the hypoglossal canal. It innervates all muscles of the tongue, excluding the palatoglossus, allowing for coordinated tongue movement. 3
Hypoglossal nerve palsy (HNP) stands as an infrequent complication in the perioperative period, posing physical, social, and psychological challenges for afflicted individuals. 4
The causes of HNP are diverse and include neoplasms at the base, vascular lesions such as carotid artery dissection, trauma (e.g. occipital condyle fracture), infection, autoimmune diseases, and iatrogenic causes including airway instrumentation. 5
While some cases are idiopathic, many are attributable to compressive or mechanical factors, particularly in the surgical or anesthetic context. 5
Recognition of prodromal symptoms such as neck pain, dysphagia, or dysarthria may aid in surgical procedures involving operations, endotracheal intubation, or the use of a laryngeal mask airway in proximity to the hypoglossal nerve, which can lead to its injury. 6 Given the anatomical vulnerability of the hypoglossal nerve located between the stylohyoid ligament and the greater horn of the hyoid bone at the mandibular angle, it is susceptible to pressure from the intubation tube. 7
Identifying this complication promptly is imperative due to the potential for misdiagnosis, including ischemic stroke, intracranial hematoma, carotid artery dissection, airway obstruction, or airway trauma. 4
Recognition of HNP requires a high index of suspicion, especially when presenting with subtle or prodromal symptoms such as neck pain or dysarthria. 5
Here, we report a case of isolated unilateral HNP following an uneventful septoturbinoplasty operation.
Case presentation
A 27-year-old man with no significant medical or surgical history visited our outpatient clinic complaining of recurrent sinusitis episodes spanning a year. Despite prior treatments with antibiotics and nasal sprays, he continued to suffer from symptoms of nasal congestion, headaches, and recurring sinusitis attacks. Physical examination revealed a deviated S-shaped nasal septum and bilateral hypertrophy of the inferior turbinates, with normal findings in the oropharynx and ears. Consequently, a septoturbinoplasty was scheduled.
During preoperative assessment, the patient’s Mallampati score was 2, and the American Society of Anesthesiologists (ASA) score was 1. General anesthesia induction involved intravenous administration of 1 mg of midazolam, fentanyl at 1 μg/kg (70 μg), 35 mg of atracurium, and propofol at 2 mg/kg (160 mg). The patient underwent laryngoscopy using a No. 4 Macintosh laryngoscope, and successful intubation was achieved in the supine position with a No. 8 endotracheal tube on the second attempt.
During the first attempt, visualization of the vocal cords was limited. In the second attempt, increased upward and lateral pressure was applied with the laryngoscope to improve the view, along with additional neck extension.
Endotracheal tube cuff pressure was regulated to a maximum of 20 mmHg, ensuring no gas leakage. The tube was secured on the left side of the mouth, and the patient’s lungs were effectively ventilated using volume-controlled mechanical ventilation, delivering a tidal volume of 500 and a respiratory rate of 12. For inhalation anesthesia, a mixture of isoflurane at 1.2%, along with 2 l/min of oxygen and 3 l/min of nitrous oxide (N2O), was administered. Dexamethasone 8 mg IV was administered postoperatively to reduce the risk of laryngeal edema.
Throughout the 2-h operation, the patient’s head was positioned semi-supine at ~20°, supported by a donut pillow, and controlled hypotensive anesthesia was maintained to keep systolic arterial blood pressure between 80 and 90 mmHg.
The patient remained hemodynamically stable and well-oxygenated throughout the procedure, with no notable changes observed in cardiovascular and pulmonary parameters during general anesthesia or upon awakening. Extubation was carried out without complications.
On the second day of observation, the patient experienced difficulty swallowing both solid and liquid foods, along with challenges in speaking. During the examination, restricted tongue mobility was noted. When the patient protruded his tongue, it veered toward the right and was unable to move to the left. However, the gag reflex was intact, and there were no tongue fasciculations. Pharyngeal and soft palate movements appeared normal, as did the sense of taste. Indirect laryngoscopy revealed typical vocal cord function. Apart from isolated right hypoglossal nerve impairment, all other cranial nerve examinations yielded normal results. Following consultation at the neurology clinic, magnetic resonance imaging (MRI) and complete blood count tests returned normal results, except for significantly elevated C-reactive protein levels. The patient commenced oral prednisolone treatment at a dosage of 1 mg/kg, gradually tapering over 1 month. After this period, the patient experienced relief in tongue movements, which further improved partially after 2 months.
Discussion
The hypoglossal nerve (the 12th cranial nerve) is a motor nerve that innervates the intrinsic and extrinsic muscles of the tongue. Isolated hypoglossal nerve injury due to anesthesia—particularly endotracheal intubation—is a rare but documented complication. 8 In cases of peripheral nerve injury, neurapraxia is often implicated. It may arise from ischemia or mechanical compression and usually resolves within 3 months; this mechanism is believed to underlie intubation-associated lesions. 9
The occurrence of this complication is particularly unusual in the context of uneventful intubation and in the absence of congenital abnormalities such as Arnold–Chiari malformation. 10 A related condition, Tapia’s syndrome, involves concurrent injury to the hypoglossal nerve (cranial nerve XII) and the recurrent laryngeal branch of the vagus nerve (cranial nerve X), presenting with unilateral tongue and vocal cord paralysis during general anesthesia. 11
Unilateral peripheral HNP typically results in ipsilateral tongue deviation and difficulties with speech and swallowing. 4 When such findings are present, differential diagnoses including ischemic stroke, intracranial hemorrhage, carotid artery dissection, airway obstruction, or airway trauma should be considered. 4 In our case, neurovascular causes were ruled out via head MRI, and indirect laryngoscopy confirmed normal vocal cord mobility. All other cranial nerves were also intact, supporting a diagnosis of isolated right HNP.
Although our patient did not experience any apparent complications with airway management, several risk factors were present. The duration of the procedure extended to 2 h, and the patient was male, both potential risk enhancers.
Male patients are more predisposed to hypoglossal nerve injury due to a longer greater cornu of the hyoid bone, increased hyoid bone dimensions, and earlier ossification of the hyoid-ligament complex, all of which increase the risk of mechanical compression during airway manipulation. 11
Furthermore, N2O was used as part of the inhalation anesthesia, a known factor in increasing endotracheal cuff pressure. 12
Isolated HNP has been reported after various surgical procedures, including otorhinolaryngologic, 13 shoulder, cardiovascular, plastic, thoracic, and neurosurgeries.13–15 The mechanism may involve off-throat packing, pressure during hemostasis, undetected neck rotation, or hyperextension. Position changes during and after intubation, often necessary to access surgical fields, may further increase the risk. 14
In this case, the patient was positioned in a semi-supine posture at ~20°, with neck extension supported by a donut pillow for the duration of the 2-h septoturbinoplasty. These factors may have contributed to prolonged mechanical compression of the hypoglossal nerve.
Symptom onset typically occurs within 24 h after surgery, and recovery is expected within 6 weeks to 1 year due to the neuropraxic nature of the injury. 4 Our patient was managed with oral prednisolone at a dose of 1 mg/kg tapered over 1 month. Improvement in tongue mobility was observed after this period, with partial functional recovery by the end of 2 months. Notably, the patient also received dexamethasone (8 mg IV) intraoperatively to reduce the risk of laryngeal edema.
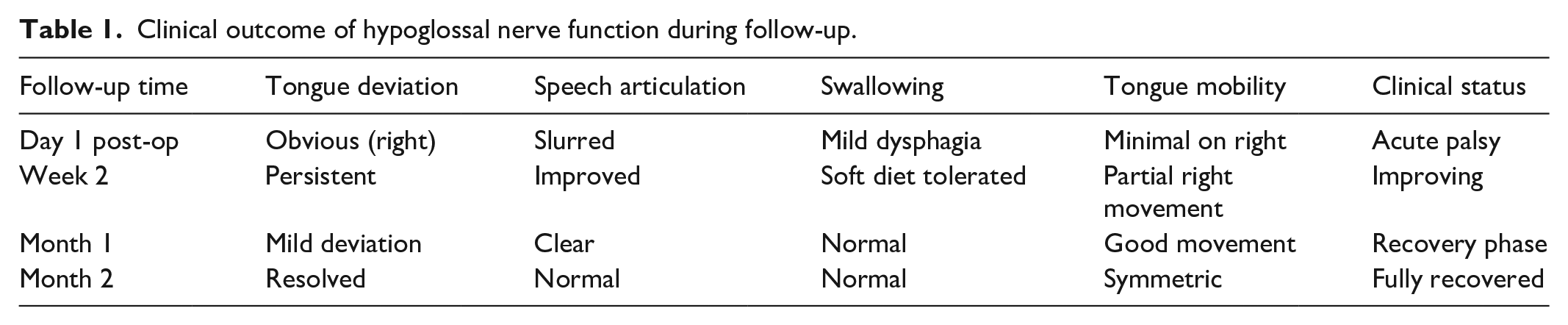
During follow-up, the patient was assessed at regular intervals to evaluate tongue deviation, mobility, speech articulation, and swallowing function. A simple functional rating approach was used based on physical examination and patient-reported symptoms (Table 1).
Clinical outcome of hypoglossal nerve function during follow-up.
Although the intubation was ultimately successful, repeated attempts and exaggerated head extension may have contributed to mechanical compression of the hypoglossal nerve. These maneuvers have been associated with nerve injury in prior reports.
Leuzinger et al. 16 reported an isolated HNP in a patient who underwent prolonged intubation with a difficult airway, suggesting that both stretch injury and compression between the tube and hyoid bone contribute to nerve damage.
The patient showed full clinical recovery by the end of the second month, with no residual symptoms on examination. 17 More recently, Bassi et al. documented cranial nerve involvement in a case requiring nasotracheal intubation alongside hypoglossal neuromonitoring, emphasizing the vulnerability of the hypoglossal nerve even during emergency airway management. 18
The hypoglossal nerve’s anatomical course near the occipital condyle and its exit through the hypoglossal canal predispose it to compression injuries, even in the absence of direct trauma. Ozdemir et al. highlight the role of surrounding bony structures, such as the clivus, in redirecting force toward the nerve, reinforcing its vulnerability during surgical or intubation-related manipulations. 19
Even HNP has been reported after various surgical procedures and airway manipulations; isolated unilateral HNP following septoturbinoplasty remains an exceptionally rare complication, with limited recent reports in the literature, especially in our regional context.
Although we were unable to include clinical images due to unavailability, the case is thoroughly documented through clinical descriptions, physical findings, and diagnostic investigations, all of which returned normal, aside from the hypoglossal nerve findings. While visual documentation would have added clarity, the textual description is intended to provide a clear and comprehensive understanding of this rare presentation.
Conclusion
This case underscores hypoglossal nerve injury as a rare yet important complication of septoturbinoplasty under general anesthesia. Prevention relies on thorough preoperative assessment, gentle airway management, and awareness of positioning risks during surgery. Prompt recognition and early initiation of treatment, such as corticosteroids, may aid in recovery and improve patient outcomes.
Footnotes
Acknowledgements
The authors express their gratitude to the patient and their family for their great contribution. Also, the authors express profound gratitude to the Polytechnic Medical Students’ Research Association (PMRA) for their invaluable contributions and unwavering support that significantly enriched every stage of the research journey.
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for Publication
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Authors Contributions
Omar H. Salloum, Mohammad Marrawani, Fouad Asafra, Mustafa Alatawneh, Omar Qasem Heih, and Dina Mamdouh Qumsiyeh contributed to various aspects of this study. Omar H. Salloum and Mohammad Marrawani contributed to the design of the study and drafting of the manuscript. Fouad Asafra, Omar H. Salloum, and Abed Alkareem Asherah contributed to data collection, data entry, and data interpretation, and also participated in drafting the manuscript. Mustafa Alatawneh, Omar Qasem Heih, and Dina Mamdouh Qumsiyeh provided valuable insights into data interpretation and contributed to the drafting of the manuscript. Abed Alkareem Asherah supervised the work, provided guidance on study design and data interpretation. All authors have read and approved the final manuscript. Each author has contributed sufficiently to take public responsibility for the content of the study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data supporting the findings of this study are readily available within the article.