
Abstract
We present a case of a 43-year-old woman with Vogt–Koyanagi–Harada syndrome, on adalimumab, methotrexate, and risedronate, who developed pruritic, skin-colored papules on the dorsal hands. A biopsy revealed features consistent with syringomas. Syringomas are benign eccrine duct tumors that typically appear as small, shiny papules, most often in the periorbital area but can also present in acral regions. Only 14 cases of exclusive acral syringomas have been reported. Eruptive variants may resemble conditions such as lichen nitidus or warts, making dermoscopy and histopathology crucial for diagnosis. Dermoscopically, syringomas may show fine reticulate brown lines and homogenous pigmentation. Histologically, they show small ductal structures and epithelial cords in the dermis. Their exact pathogenesis remains unclear, possibly involving hormonal or inflammatory triggers. Treatment is challenging due to their dermal depth and recurrence risk, with lasers and retinoids among the options. This case highlights the diagnostic complexity of acral eruptive syringomas.
Keywords
Introduction
Syringomas are benign tumors originating from the intraepidermal portion of the eccrine duct that present with a variable clinical appearance, including solitary or multiple lesions with localized multifocal, or generalized distribution. Syringomas often appear on the lower eyelids and upper cheeks, with additional sites reported such as the axillae, abdomen, and genital area.1–4 Here, we present a case of eruptive acral syringomas in a 43-year-old woman characterized by local skin-colored papules, prompting the need for differentiation from other papular eruptions. The clinical, dermoscopic, and histopathological features of eruptive syringomas, and particularly previous reports of the rare acral variants, are explored in this report. The patient consented to this publication.
Case report
A 43-year-old woman diagnosed with Vogt–Koyanagi–Harada syndrome with severe bilateral panuveitis is currently treated with adalimumab (40 mg every 2 weeks) and methotrexate (25 mg weekly). In addition to these medications, she is also taking risendronate. The patient presented with a 2-year history of sporadically pruritic skin-colored papules on the dorsal aspect of her hands particularly over the base of the thumb and first interphalangeal space (Figures 1 and 2).

Skin-colored papules arising on the dorsal hand.
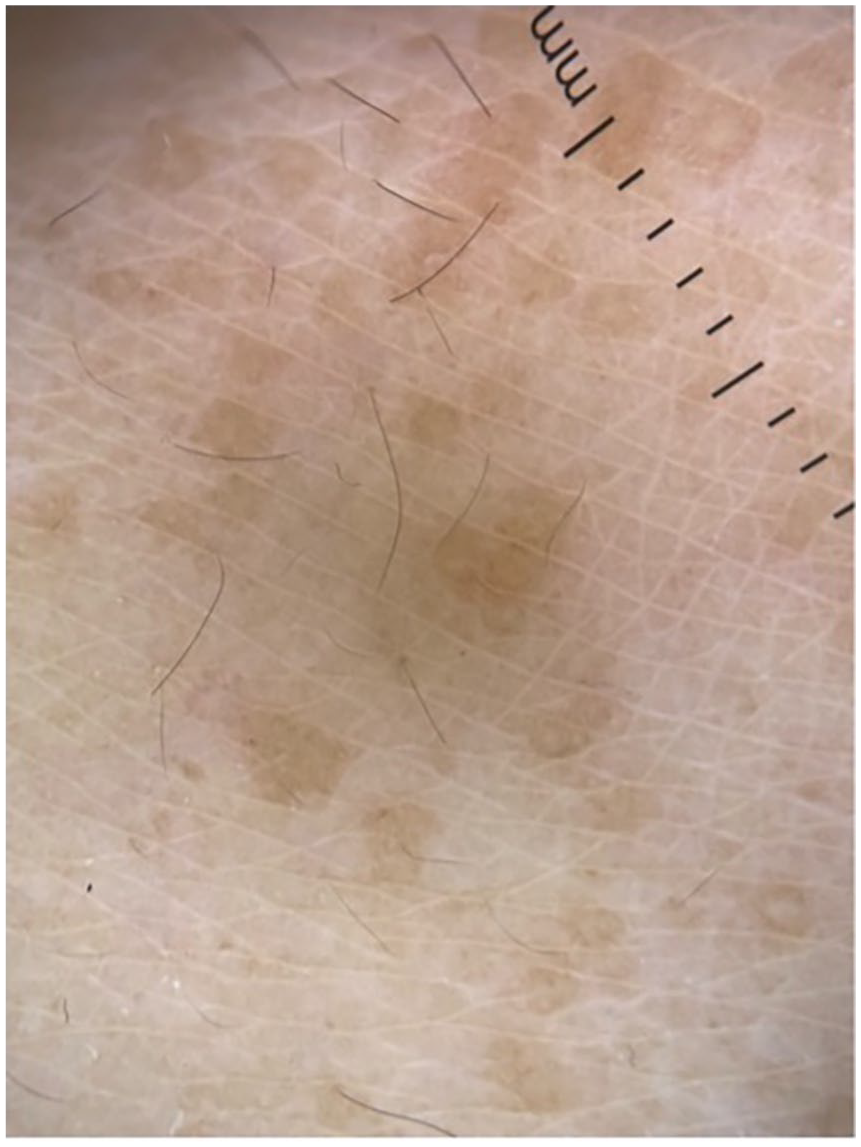
Dermoscopy (Dermlite DL4, 10X; contact, polarised mode) revealed clusters of brown papules, which showed a light brown faint network.
Clinically lichen nitidus was suspected. A biopsy of one of these lesions was performed, revealing histologic findings consistent with syringomas (Figure 3). Evidence of dermatitis was not identified.

Photomicrographs of biopsy specimen. Low-power view (a) demonstrates small clusters (multifocal) of epithelioid islands in the superficial dermis (arrows) (H&E, 10×), identified as exhibiting ductal differentiation on medium power (b, H&E 20×) and high-power (c and d, H&E 40×).
Discussion
Syringomas are benign tumors that originate from the intraepidermal portion of the eccrine duct.5–8 These were initially described by Kaposi in 1872 as lymphangioma tuberosum multiplex.
Syringomas manifest as single or clustered, soft, dome-shaped, or flat-topped papules varying in size from one to several millimeters. These lesions typically exhibit symmetry and are characterized by skin colored to brownish shiny papules, that may be asymptomatic or pruritic.9,10 They are more frequently seen in women at puberty or later in life. The onset of these lesions has also been reported during pregnancy. 11
Syringomas predominately appear in the periorbital region 12 but can occur in other areas including the axillae, abdomen, vulva, and penis.2–4,13,14
The clinical appearance of syringomas is variable, presenting as solitary or multiple lesions. The tumors can be localized, multifocal, or generalized in their distribution, and they may also appear in an eruptive manner.5,15.
As per the classification proposed by Friedman and Butler in 1987, syringomas exhibit four primary variants: localized, generalized (including eruptive and multiple forms), familial, and those associated with Down syndrome. 16 This classification remains used in current medical practice.
Less common variations, including plaque-type, linear, milium-like syringomas, chondroid, scalp, acral, and solitary on the ankle have been documented in the medical literature.4,6,13
In localized cases, the periorbital region is typically affected, and clinical diagnosis suffices. 17 However, with eruptive syringomas, reports indicate a higher prevalence on the neck, anterior trunk, and axillae. 6 Notably, it tends to spare the palms, soles, and mucosal areas. 10
Exclusively acral syringomas are rare and infrequently reported. 18 In contrast to the typical clinical presentation of syringomas, these have been observed in older individuals with no gender predilection. 11 Approximately 14 cases of isolated eruptive acral syringomas have been reported in the literature, with the earliest case identified in 1977 by Hughes and Apisarnthanarax. 19 Cases of acral syringomas concomitant with syringomas in the typical bilateral infraorbital location have also been reported. 11 It has been suggested to categorize acral syringomas as a distinct entity within the initial classification of syringomas put forth by Friedman and Butler. 11
Balci et al. documented the coexistence of syringomas and trichoepitheliomas on the face, with an earlier onset of the latter. However, they found no apparent relationship between the two conditions. The association of syringomas and trichoepitheliomas was proposed to be coincidental. 20
Eruptive syringomas can be easily misidentified among the differential diagnoses associated with skin-colored papules, occasionally resembling lichen nitidus, milia, acne vulgaris, lichen planus, trichoepithelioma, and warts. Two cases have been reported misdiagnosing eruptive syringomas as warts. 21
In lichen nitidus, the skin-colored papules exhibit a shiny, slightly elevated appearance, as in our case. Multiple trichoepitheliomas typically appear on the face, in the nasolabial folds, on the forehead and eyelids without becoming generalized. Primary milia occur spontaneously as white papules on the face of predisposed individuals, while secondary milia appear following dermabrasion or the healing of subepidermal bullae. In juvenile xanthogranuloma and benign cephalic histiocytoma, reddish-brown papules appear suddenly, typically in the first few years of life.5,22
The dermoscopic findings can help to differentiate syringomas from other papules. Dermoscopic observations documented in the literature describe fine reticulate brown lines on a light brown background, in contrast to the typical findings of Wickham striae observed in lichen planus. 5 A homogeneous brown area with a delicate brown pigment network was reported by Hayashi et al. 7 Reticular light brown lines, structureless light brown areas, and reticular vessels were seen on dermoscopy by Botsali et al. 17 Dermoscopic findings of an incomplete pigment network with a reddish tinge have been described as well. 15 There is also a reported description of shiny white structures over a fading pink background with dotted and linear vessels in vulvar syringoma. 14
Histopathologically, syringomas exhibit numerous small ductal structures and cords of cells wrapped by a fibrous stroma, generally limited to the superficial reticular dermis and papillary dermis. The ductal structures typically display a double layer of epithelial cells and may contain an amorphous substance or keratin. Additionally, comma-like, or tadpole-like extensions of epithelial cells prolong from some ductal structures. 9
The exact pathophysiology of eruptive syringomas is not completely understood. One theory suggests that previous skin inflammation may trigger a response in the sweat glands, leading to the development of the lesions. It has been reported that eruptive syringomas often follow events such as contact dermatitis, shaving, laser hair removal, alopecia areata, or radiation dermatitis.10,23 Although some experts consider the possibility of a growth-related process (neoplastic), this idea is not universally accepted.23,24 No triggers were found in our patient.
It has been postulated that hormone levels could contribute to the progression of syringoma development, as evidenced by a higher occurrence in women. Increased proliferation is also observed during pregnancy, puberty, and the premenstrual period.25,26 In one patient, there was a noted correlation between the appearance of lesions and factors such as sun exposure, heat, hot baths, and stress, which exacerbated the condition. Described as reddish-brown, confluent papules the lesions in this case were localized to the sun-exposed areas of the distal arms and forearms, with a relative sparing of the sun-protected wristwatch area. 9
Syringomas typically exhibit a mean depth of 0.70 ± 0.20 mm, ranging from 0.4 to 1.2 mm. 27 Various therapeutic approaches, primarily pursued for cosmetic reasons, include surgical excision, cryotherapy, electrodessication, chemical peels, topical atropine, and topical and oral retinoids.2,10,28 Ablative laser and nonablative fractional lasers have been reported with positive outcomes for syringomas. 29
Generalized forms have been treated with topical and oral retinoids, with limited efficacy. 5 No therapeutic measures were used in our patient as on subsequent visits the lesions appeared flatter and less noticeable.
The challenge in treating syringomas lies in their dermal location, resulting in incomplete removal and a high likelihood of recurrence. The majority of these treatments yield unsatisfactory results, carrying the risk of lesion recurrence, scarring, and postinflammatory pigmentation after intervention. 1
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The funding source is the Krembil Foundation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.