
Abstract
Pasteurella multocida is a small, facultatively anaerobic coccobacillus commonly found in the upper respiratory tract of many mammals, birds, and especially felines. It can cause a wide range of infections in humans, often resulting from bites or scratches from pet animals. The literature has previously reported 15 cases of epiglottitis caused by Pasteurella multocida. Here we describe a case of severe epiglottitis complicated with neck area cellulitis in a previously healthy middle-aged woman. Blood cultures were positive for Pasteurella multocida, likely originating from a scratch by the patient’s pet cat. The infection was treated with antibiotics, and the patient required intubation in the intensive care unit for 6 days. Epiglottitis is a life-threatening disease. In epiglottitis caused by Pasteurella multocida, the pathogen is significantly more likely to be detected in blood cultures compared to its involvement in other types of infections. Pasteurella multocida should be considered a zoonosis.
Keywords
Introduction
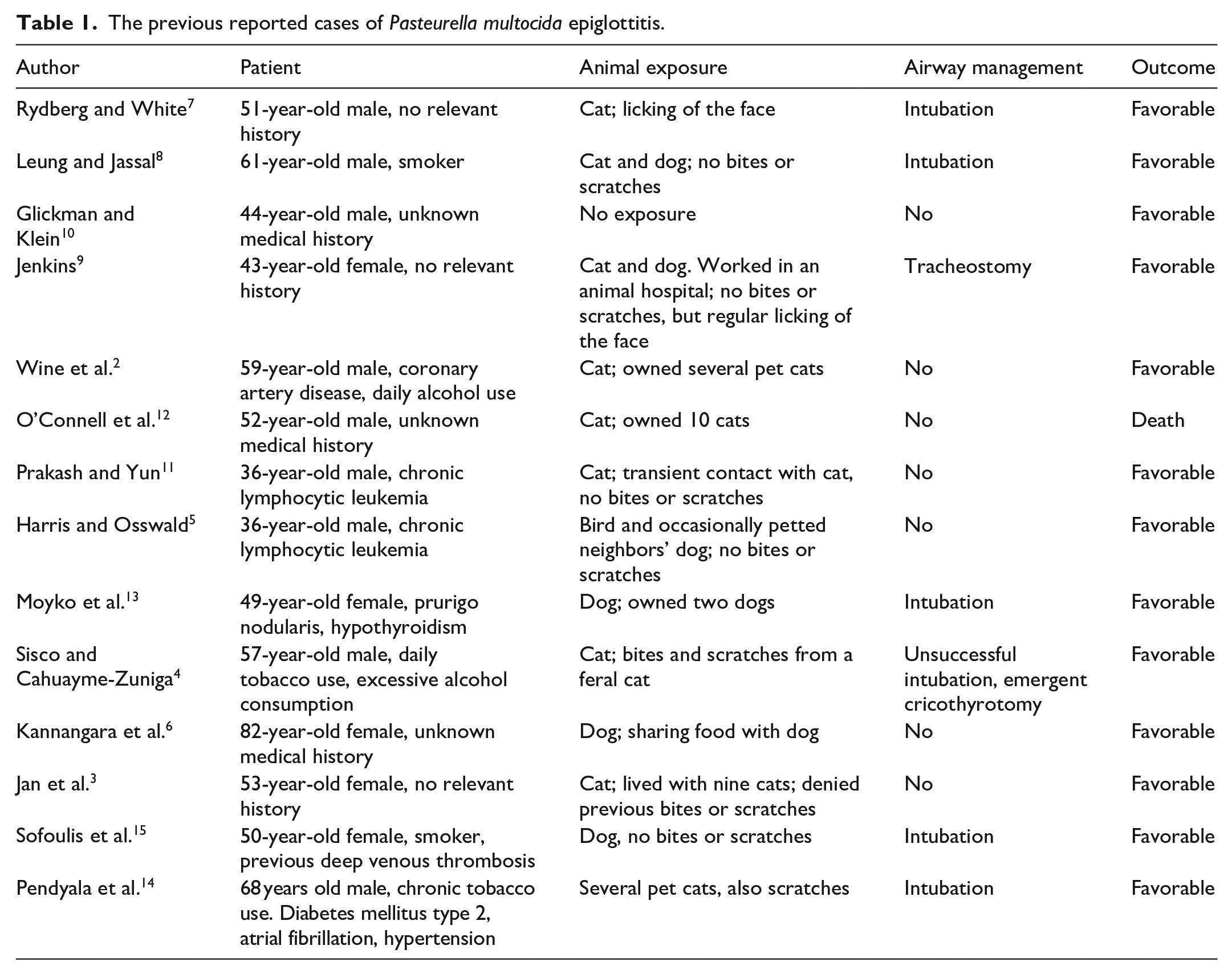
Pasteurella multocida is a small, facultatively anaerobic Gram-negative coccobacillus that is part of the normal flora of the upper respiratory tract, oral cavity, and pharynx in birds, mammals, and especially felines. 1 In humans, it has been described as causing infections of the skin, bone, joints, upper and lower respiratory tract, abdominal cavity, and central nervous system. Most of these infections have resulted from bites of pet animals, but other exposure mechanisms have also been documented. 2 The literature has previously reported 15 cases of epiglottitis caused by P. multocida, of which 14 involved animal-related exposure (Table 1).2–15 One case out of 15 resulted in death. 12 To the best of our knowledge, this is the second case in which, in addition to epiglottitis, there has also been cellulitis in the neck area.
The previous reported cases of Pasteurella multocida epiglottitis.
Case report
A 54-year-old previously healthy woman was admitted to the emergency department after complaining of a fever and sore throat. She advised that the previous day she had noticed that her neck was erythematous and swollen. At admission, she had a blood pressure of 184/114 mmHg, a heart rate of 150 beats/min, and an auricular temperature of 39°C (102.2°F). Peripheral oxygen saturation was 92% on room air. She had clear difficulty breathing as she had to sit with a forward lean, her respiratory rate was 30 breaths/min, and a stridor was audible on inspiration. She was immediately given 80 mg methylprednisolone intravenously as well as ipratropium–salbutamol and racepinephrine inhalations. Thirty-five percent of supplementary oxygen was also initiated. In the laboratory tests, taken at admission (Table 2), the blood neutrophil level was 5.65 E9/L and the total leukocytes were 6.5 E9/L. C-reactive protein (CRP) level was highly elevated at 255 mg/L. Blood cultures were also taken. Antibiotic therapy with cefuroxime 1500 mg four times daily and metronidazole 500 mg three times daily was started empirically.
Laboratory test values on admission to the emergency department.

aB: arterial blood; BE: base excess; p: partial pressure.
The patient was rapidly transferred to an operating room where an anesthesiologist successfully intubated the patient with a video laryngoscope and an intubation adjunct. The view, however, was limited. ENT specialists examined the patient in the operating room. The patient’s neck was slightly swollen and erythematous, but in the test incision, of skin tissues were vital and no fasciitis was diagnosed. During the video laryngoscope examination, epiglottis, vallecula, and arytenoids were red and swollen, while the oropharynx appeared healthy. As a result, an epiglottitis/supraglottitis diagnosis was made. The throat culture obtained during intubation was negative; however, the patient had already received antibiotics.
Patient’s care continued in the intensive care unit. A computed tomography of the neck and mediastinal area was completed, and a diffuse edema of the pharynx, neck, and mediastinum was found, though no abscesses were observed (Figure 1). The next day, a Gram-negative rod was grown in a blood culture, and the antibiotic treatment was changed to ceftriaxone and metronidazole. IV-steroids were not continued after a single dose. On day 3, the blood culture result was confirmed as P. multocida. The bacteria were sensitive to amoxicillin, ampicillin, doxycycline, cefotaxime, levofloxacin, and sulfa-trimethoprim. Ceftriaxone and metronidazole were continued during the whole hospitalization time. The patient remained hemodynamically stable during the whole treatment period. The highest CRP level was 523 mg/L on the second day of hospitalization. On the sixth treatment day, the patient was extubated as the edema of the larynx was reduced. The next day, the patient was transferred to the inpatient ward, where the patient returned home on the eighth treatment day. That day, leukocytes were 9.3 and CRP 43. Per oral sulfa-trimethoprim was continued at home for 3 days.

Computed tomography of the neck and thoracic area (sagittal view) showing neck area soft tissue edema (thin arrow) and mediastinal edema (thick arrow).
During the treatment period, it was discovered that the patient had cats at home and one of them had scratched her toe before an infection started. Thus, the infection was considered zoonosis. After 3-month follow-up, the patient has made a full recovery.
Discussion
P. multocida has commonly been described as causing skin and soft tissue infections, particularly in relation to animal bites or scratches. However, epiglottitis has been an extremely rare complication, and it is even rarer for it to be associated with cellulitis of the neck and mediastinum, which has disseminated hematogenously, as in our case. Our patient was considered immunocompetent, but she used tobacco, which has been associated with Pasteurella infection in previous case reports.
In Giordano’s material of 44 patients with various P. multocida infections, bacteremia was described in only eight patients. Of these, only one case was bite or scratch-related, while seven were non-bite-related. Among the non-bite-related bacteremias, six out of seven patients had underlying immunocompromising conditions, most commonly various malignancies (both solid and hematologic), liver cirrhosis, and end-stage renal disease. The patient with bite-related bacteremia did not have a diagnosed immune system disorder, but was elderly. 17 In Kannangara et al.’s data of eight patients (non-bite-related P. multocida bacteremias, including one epiglottitis), the findings were similar. 6 Thus, P. multocida bacteremias have almost invariably occurred in patients with immune system impairments. However, it is worth noting that there was only one case of epiglottitis.
Liver cirrhosis was the most common individual comorbidity predisposing patients to Pasteurella bacteremia. 18 One potential explanation is cirrhosis-associated immune dysfunction, which can be classified into two immune phenotypes: the low-grade systemic inflammatory and the high-grade systemic inflammatory phenotype. Both represent dynamic and progressive states characterized by simultaneous pro-inflammatory activity and immunosuppression, depending on the stage of cirrhosis.
The high-grade phenotype is typically observed in patients with acute-on-chronic liver failure, decompensation, and organ dysfunction, and is marked by profound functional paralysis of the immune system cells. When combined with cirrhosis-associated intestinal bacterial translocation and portosystemic shunt, this substantially increases the risk of bacteremia and, consequently, systemic dissemination of infection and worsens prognosis. 19
In epiglottitis caused by P. multocida, the pathogen has been found in blood cultures in the majority of cases, unlike in many other infections caused by P. multocida.5,6 In general, positive blood cultures are found in <10% of epiglottitis cases. 20
Interestingly, among the cases of P. multocida bacteremia with epiglottitis, many patients were previously healthy and did not necessarily have known immune system compromises. Comorbidities were rarer in bite-related bacteremias compared to non-bite-related ones. This alone, however, does not fully explain the difference, as about half of the previously reported P. multocida epiglottitis cases were non-bite-related (Table 1). One notable feature in epiglottitis cases is the relatively high proportion of smokers. It is possible that smoking causes local damage to the mucosa of the upper respiratory tract and/or impairs the local mucosal immune defense system. No cases of IgA deficiency have been reported among P. multocida epiglottitis patients to date. On the other hand, P. multocida naturally colonizes the upper respiratory tracts of carriers, which may predispose that area to infection. All of this suggests that P. multocida is not solely an opportunistic pathogen. It is also important to note that animal bites are frequently managed with prophylactic antimicrobials, which may decrease the incidence of bite-related infections and thereby highlight the relative prominence of non-bite-related cases.
In P. multocida epiglottitis cases, infections originating from cats are particularly emphasized. One reason might be that P. multocida occurs more frequently in the normal oral flora of cats compared to, for example, dogs. 21 Another possible explanation—especially in bite-related infections—is the different structure of cats’ teeth and claws compared to dogs’, as they are more likely to cause deeper penetrating bites or scratches.
Epiglottitis is a life-threatening disease. 4 In adults, the most common causative agents in the post-Haemophilus influenzae vaccination era are bacteria from the Streptococci and Staphylococci groups, viruses, and, less commonly, fungal infections. If epiglottitis is suspected, the patient should be evaluated as quickly as possible, with particular attention paid to the potential development of an airway obstruction. Symptoms of an impending airway obstruction include difficulty inhaling, stridor, seeking a forward-leaning sitting position, drooling, hoarseness, as well as hypoxia and increased respiratory rate.22,23
Securing the airway is the most important priority before conducting any other diagnostic examinations. If intubation is necessary, it should be performed by an experienced specialist, as it can be very challenging due to swelling of the epiglottis and surrounding structures. In our patient’s case, the airway was secured in the operating room with immediate emergency tracheostomy readiness.
Contact with animals has been documented in all case reports except one. 3 However, the contacts have not always been bites or scratches. They have also included, for example, facial licking and kissing, and in some cases, the exact mode of exposure to pathogens has remained unknown.3,6 A single case has also been described where the source of infection was peanut butter and crackers that the patient had shared with a dog. 6
For the treatment of P. multocida infections, it is recommended to use a combination of amoxicillin and a beta-lactamase inhibitor, or in cases of penicillin allergy, a combination of doxycycline and metronidazole. Ceftriaxone or a combination of clindamycin with either fluoroquinolone or trimethoprim-sulfamethoxazole is also an option. 21
In the previous case reports, the difficulty of the disease has been variable. Many of the patients with P. multocida epiglottitis have been treated with intravenous antibiotics without tracheostomy or intubation. However, some of the patients have needed intubation for up to 4 days or tracheostomy. In our case, the disease was severe, and symptoms developed rapidly. This was similar to another case, in which, in addition to epiglottitis, a skin and soft tissue infection of the neck area was also presented. 4
In Giordano’s cohort of 44 patients (all P. multocida infections in the Medical University of South Carolina laboratory system from 2000 to 2014), 18% required intensive care, and the mortality rate was 9%. 17 In a data of 14 patients with epiglottitis (Table 1), the need for intensive care was 50%, and potentially even higher, as it was not reported in all cases. The mortality rate was 7%. These findings suggest that epiglottitis caused by P. multocida represents a substantially more severe clinical manifestation compared to the average presentation of infections caused by P. multocida.
In our case, antimicrobial treatment was initiated according to the general principles for treating epiglottitis, with a combination of cefuroxime and metronidazole. When a Gram-negative rod grew in the blood culture, cefuroxime was replaced with ceftriaxone. At the end of the parenteral treatment, the patient continued with trimethoprim-sulfamethoxazole for 3 more days. The total duration of antibiotic therapy was 10 days. Previously reported antimicrobial treatment durations in the literature have typically ranged from 10 days to 2 weeks. 3
Conclusion
Epiglottitis caused by P. multocida is a life-threatening infection. Unlike in other cases of epiglottitis, the pathogen seems to be found in blood cultures in the majority of cases. Practically all cases described in the literature have involved direct exposure to animals, most commonly cats and dogs. P. multocida can be considered a zoonosis. However, the exposure has not always been due to bites or scratches; various routes of exposure have been described. For this reason, pets should not be allowed to lick faces or share kisses, as—even though the infection is extremely rare—it can be potentially fatal.
Footnotes
Ethical considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent to participate
Informed consent for the use of data was obtained from the patient, after which all data were fully anonymized.
Consent for publication
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Author contributions
Tuomas Filppula: writing original draft, project administration, investigation. Pihla Pakkanen: writing original draft, review, and editing. Eero Saari: writing original draft. Veli-Pekka Harjola: review and editing, supervision, project administration.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Open Access funding provided by University of Helsinki including Helsinki University Central Hospital.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.