
Abstract
There has been a significant evolution in the definition and management of sepsis over the last three decades. This is driven in part due to the advances made in our understanding of its pathophysiology. There is evidence to show that the manifestations of sepsis can no longer be attributed only to the infectious agent and the immune response it engenders, but also to significant alterations in coagulation, immunosuppression, and organ dysfunction. A revolutionary change in the way we manage sepsis has been the adoption of early goal-directed therapy. This involves the early identification of at-risk patients and prompt treatment with antibiotics, hemodynamic optimization, and appropriate supportive care. This has contributed significantly to the overall improved outcomes with sepsis. Investigation into clinically relevant biomarkers of sepsis are ongoing and have yet to yield effective results. Scoring systems such as the sequential organ failure assessment and Acute Physiology and Chronic Health Evaluation help risk-stratify patients with sepsis. Advances in precision medicine techniques and the development of targeted therapy directed at limiting the excesses of the inflammatory and coagulatory cascades offer potentially viable avenues for future research. This review summarizes the progress made in the diagnosis and management of sepsis over the past two decades and examines promising avenues for future research.
Introduction
Sepsis is a medical emergency that describes the body’s systemic immunological response to an infectious process that can lead to end-stage organ dysfunction and death. Despite significant advancements in the understanding of the pathophysiology of this clinical syndrome, advancements in hemodynamic monitoring tools, and resuscitation measures, sepsis remains one of the major causes of morbidity and mortality in critically ill patients. 1 The annual incidence of severe sepsis and septic shock in the United States is up to 300 cases per 100,000 people. Sepsis is also the most expensive healthcare problem in the United States, accounting for more than $20 million (about 5.2% of the total hospital cost) in 2011 alone. 2
The global epidemiological burden of sepsis is, however, difficult to ascertain. It is estimated that more than 30 million people are affected by sepsis every year worldwide, resulting in potentially 6 million deaths annually. Mortality rates from sepsis, as per the data from the Surviving Sepsis Campaign 2012, were approximately 41% in Europe versus approximately 28.3% in the United States. 3 This difference however disappeared when adjusted for disease severity. 3 This implies that the mortality in sepsis varies according to patient characteristics as well. A multicenter study in Australia and New Zealand that included 101,064 critical patients showed that the mortality rate in sepsis has decreased over the years from around 35% in 2000 to about 20% in 2012. 1
Definition
Over the years, our understanding of the complex pathophysiology of sepsis has improved, and so has our ability to define sepsis. The word sepsis is derived from the Greek word for “decomposition” or “decay,” and its first documented use was about 2700 years ago in Homer’s poems. It was subsequently used in the works of Hippocrates and Galen in later centuries. 4 In the 1800s, the “Germ theory” of disease was conceived and there was some recognition that sepsis originated from harmful microorganisms. The first modern definition was attempted in 1914 by Hugo Schottmüller who wrote that “sepsis is present if a focus has developed from which pathogenic bacteria, constantly or periodically, invade the blood stream in such a way that this causes subjective and objective symptoms.” 5 Over the course of the 20th century, numerous experimental and clinical trials were able to demonstrate the importance of the host immune response to the manifestations of sepsis. However, due to heterogeneity of the disease process, it posed serious difficulties in recognizing, treating, and studying sepsis. 5 Finally, at a SCCM-ACCP conference in 1991, Roger Bone and his colleagues laid the foundation for the first consensus definition of sepsis. There have been significant advances in the pathobiology of sepsis in the last two decades. We have a better understanding of cell biology, biochemistry, immunology, and morphology, as well as changes in circulation and organ function. This understanding has led to the changes in the definition of sepsis. This has also contributed to better management of sepsis leading to changes in the epidemiology of the sepsis (Table 1).
Definitions of sepsis.

FIO2: fraction of inspired oxygen; GCS: Glasgow Coma Scale; MAP: mean arterial pressure; PaCO2: partial pressure of carbon dioxide; PaO2: partial pressure of oxygen; SOFA: sequential organ failure assessment.

FIO2: fraction of inspired oxygen; MAP: mean arterial pressure; PaO2: partial pressure of oxygen.
Catecholamine doses are given as µg kg−1 min−1 for at least 1 h.
Glasgow Coma Scale scores range from 3 to 15; higher score indicates better neurological function.
Pathophysiology of sepsis
There has been a marked evolution in our understanding of the molecular pathobiology and immunology of sepsis. Previously it was felt that hemodynamic manifestations of sepsis were primarily related to the hyperimmune host response to a particular pathogen. 8 However, a large body of work on the molecular basis of sepsis has revealed a far more nuanced and complex interplay between the infectious agent and host that together produce the heterogeneous manifestations of sepsis.
Innate immunity and inflammatory mediators
The first step in the initiation of the host response to the pathogen is the activation of innate immune cells, constituted primarily by macrophages, monocytes, neutrophils, and natural killer cells. 9 This occurs via the binding of pathogen-associated molecular patterns (PAMPs), such as bacterial endotoxins and fungal β-glucans to specific pattern recognition receptors, on these cells. Another source of such interaction are damage-associated molecular patterns (DAMPs) that may be intracellular material or molecules released from dead or damaged host cells, such as ATP and mitochondrial DNA. These bind to specific receptors on monocytes and macrophages such as toll-like receptors (TLRs), C-type leptin receptors, NOD-like receptors (nucleotide-binding oligomerization domain) and RIG-1 like receptors (retinoic acid inducible gene 1). This results in the activation of intracellular signal transduction pathways that cause the transcription and release of proinflammatory cytokines like TNFα, IL-1, and IL-6. In addition, some of the pattern recognition receptors, such as the NOD-like receptor group, can aggregate into larger protein complexes called inflammasomes that are involved in the production of crucial cytokines, such as IL-1β and IL-18 as well as caspases, which are involved in programmed cell death. Proinflammatory cytokines cause activation and proliferation of leukocytes, activation of the complement system, upregulation of endothelial adhesion molecules and chemokine expression, tissue factor production, and induction of hepatic acute phase reactants. In sepsis, there is an exaggeration of the above immune response resulting in collateral damage and death of host cells and tissues.
Dysregulation of hemostasis
In sepsis, there is an intersection between the inflammatory and hemostatic pathways, with the simultaneous activation of both the inflammatory and the coagulation cascades. The spectrum of this interaction can vary from mild thrombocytopenia to fulminant disseminated intravascular coagulation (DIC). The etiology of the dysregulation of coagulation in sepsis is multifactorial. The hypercoagulability of sepsis is thought to be driven by the release of tissue factor from disrupted endothelial cells (other sources include monocytes and polymorphonuclear cells). 10 In fact, in vitro experimental models of endotoxemia and bacteremia have shown a complete inhibition of inflammation-induced thrombin production with the blockade of tissue factor. 11 Tissue factor then causes the systemic activation of the coagulation cascade resulting in the production of thrombin, activation of platelets, and formation of platelet–fibrin clots. These microthrombi can cause local perfusion defects resulting in tissue hypoxia and organ dysfunction.
In addition to the procoagulant effect described above, there is a depression of the anticoagulant effects of protein C and antithrombin that would normally temper the coagulation cascade. Protein C is converted to its active form (activated protein C) by thrombomodulin which itself is activated by thrombin. Activated protein C then exerts an anticoagulant effect by degradation of factors Va and VIIIa acting in concert with activated protein S. It is also known to have potent anti-inflammatory effects via the inhibition of TNFα, IL-1β, and IL-6 and limiting of neutrophil and monocyte adhesion to endothelium. In patients with severe systemic inflammation, such as in sepsis, there are decreased plasma levels of protein C, downregulation of thrombomodulin, and low levels of protein S thus allowing for the unregulated propagation of the coagulation cascade. 12
In addition to the hypercoagulability described above, a reduction of fibrinolysis is also observed as a result of sepsis. 13 As TNFα and IL-1β levels increase, tissue plasminogen activators are released from vascular endothelial cells. The resultant increase in activation of plasmin is blunted by the sustained increase in plasminogen activator inhibitor type 1 (PAI-1). The net effect is diminished fibrinolysis and fibrin removal, which contributes to the perpetuation of microvascular thrombosis.
Immunosuppression
Interestingly, the initial proinflammatory state of sepsis is often superseded by a prolonged state of immunosuppression. There is a decrease in the number of T cells (helper and cytotoxic) as a result of apoptosis and a decreased response to inflammatory cytokines. 14 Postmortem studies of ICU patients who died of sepsis demonstrated a global depletion of CD4+ and CD8+ T cells, most notably found in the lymphoid organs such as the spleen. Studies have also demonstrated decreased production of crucial cytokines such as IL-6 and TNF in response to endotoxin.15,16 In septic patients, neutrophils were found to have expressed fewer chemokine receptors, and there was diminished chemotaxis in response to IL-8. 17
The above findings suggest that the immune system in a septic individual is unable to stage an effective immune response to secondary bacterial, viral, or fungal infections. Based on a study that showed that a low lymphocyte count early in sepsis (day 4 of diagnosis) is predictive of both 28-day and 1-year mortality, it has been postulated that early lymphopenia can serve as a biomarker for immunosuppression in sepsis. 18
Cellular, tissue, and organ dysfunction
The underlying mechanism behind tissue and organ dysfunction in sepsis is the decreased delivery to and utilization of oxygen by cells as a result of hypoperfusion. Hypoperfusion occurs due to the cardiovascular dysfunction that is seen in sepsis. 19 The incidence of septic cardiomyopathy varies from 18% to 60% in various studies. It is thought to be related to circulating cytokines, such as TNFα and IL-1β among others, which can cause depression of cardiac myocytes and an interference with their mitochondrial function. The most important feature of septic cardiomyopathy is that it is acute in onset and reversible. Second, the low left ventricular ejection fraction is accompanied by normal or low left ventricular filling pressures (unlike in cardiogenic shock) with increased left ventricular compliance. 20 Multiple studies have shown both systolic and diastolic dysfunction with decreased stroke volumes and increased end-diastolic and end-systolic volumes in sepsis.21,22 A definite effect on mortality as a result of myocardial depression, however, has not yet been established. In addition, because of the arterial and venous dilation (induced by inflammatory mediators) and consequent reduced venous return, a state of hypotension and distributive shock is produced by sepsis. There is dilation of all three components of the microvasculature—arterioles, venules, and capillaries. This is exacerbated by the leakage of intravascular fluid into the interstitial space as a result of loss of endothelial barrier function induced by alterations in endothelial cadherin and tight junctions. All the above changes in the body’s hemodynamics in conjunction with microvascular thrombosis (described earlier) can result in hypoperfusion of tissues and organs. Consequently, there is increased anaerobic glycolysis in cells resulting in the production of lactic acid. In addition, the reactive oxygen species (ROS) produced by the inflammatory response cause dysfunction of mitochondria and a drop in ATP levels. These mechanisms cause damage at the cellular level. The broader alterations described below that occur in the tissue and organs collectively and cumulatively contribute to much of the morbidity and mortality of sepsis.
There are significant alterations to the endothelium with disruption of its barrier function, vasodilation, increased leukocyte adhesion, and the creation of a procoagulant state. This results in accumulation of edema fluid in the interstitial spaces, body cavities, and subcutaneous tissue. In the lungs, there is disruption of the alveolar–endothelial barrier with accumulation of protein-rich fluid in the interstitial lung spaces and alveoli. This can cause a ventilation–perfusion mismatch, hypoxia, and decreased lung compliance producing acute respiratory distress syndrome (ARDS) in extreme cases. In the kidneys, a combination of reduced renal perfusion, acute tubular necrosis, and more subtle defects in the microvasculature and tubules together produce varying degrees of acute kidney injury. In the gastrointestinal tract, the increased permeability of the mucosal lining results both in bacterial translocation across the bowel well and autodigestion of the bowel by luminal enzymes. In the liver, there is a suppression of bilirubin clearance producing cholestasis. Altered mentation is commonly noted in sepsis and is indicative of CNS dysfunction. The endothelial changes described above undermine the blood–brain barrier, causing the entry of toxins, inflammatory cells, and cytokines. The ensuing changes of cerebral edema, neurotransmitter disruption, oxidative stress, and white matter damage give rise to a clinical spectrum of septic encephalopathy that varies from mild confusion to delirium and coma. Sepsis is known to produce a catabolic state. There is a rapid and significant breakdown of muscle to produce amino acids for gluconeogenesis that will fuel the immune cells. In addition, increased insulin resistance can result in a state of hyperglycemia.
Management of sepsis
Before 2001, there were no evidence-based guidelines for early management of severe sepsis and septic shock. 23 Previously, clinicians targeted supraphysiological values of cardiac index and oxygen delivery in critically ill patients with sepsis.24–26 However, Gattinoni et al. 25 concluded that such goal-oriented treatment does not reduce morbidity or mortality among critically ill patients. Several other studies also suggested that aggressive measures to achieve higher hemodynamic values for cardiac index and oxygen delivery did not improve patient outcomes.27,28
Beal and Cerra 29 recognized that transition of sepsis to multiple organ dysfunction could be prevented with rapid and appropriate resuscitation of shock. The idea that severe inflammatory response syndrome (SIRS), sepsis, and severe sepsis are parts of a continuous process and that SIRS can be limited if acted upon early formed the basis of early goal-directed therapy. Rivers et al., 30 described the critical “golden hours” of sepsis when there is abrupt transition to serious illness and initiation of early goal-directed therapy (EGDT). The fundamental principles of EGDT were identification of high-risk patients, appropriate cultures, source control, and early administration of appropriate antibiotics, which was then followed by early hemodynamic optimization of oxygen delivery and decreasing oxygen consumption. 26 The goals of initial resuscitation for sepsis-induced hypoperfusion included central venous pressure (CVP) of 8–12 mmHg, mean arterial pressure (MAP) of 65 mmHg, urine output of 0.5 mL kg−1 h−1, and superior vena cava oxygen saturation (ScvO2) or mixed venous saturation of 70% or 65%, respectively.30,31 Rivers et al. concluded that EGDT instituted during the first six hours, resulted in 15.9% absolute reduction in 28-day mortality rate when resuscitation targeted these physiological goals in patients with severe sepsis or septic shock presenting to the emergency department.30–32
Surviving Sepsis Campaign guidelines from 2004, thus incorporated the EGDT into the first 6-h sepsis resuscitation bundle.33–35 Several studies done thereafter reported similar reduction in 28-day mortality with EGDT or sepsis resuscitation bundle.36,37 Other investigators remained skeptical of the study design and treatment goals in EGDT. 38 An integral element of EGDT versus the standard care was central venous catheterization to monitor CVP and ScvO2 that guided the use of intravenous fluid, vasopressors, packed red cell transfusions, and dobutamine to achieve the set physiological targets.30,39 Nearly two decades after the Rivers trial, management of sepsis has evolved, and there has been an overall decline in the mortality from severe sepsis. 40
Care bundles
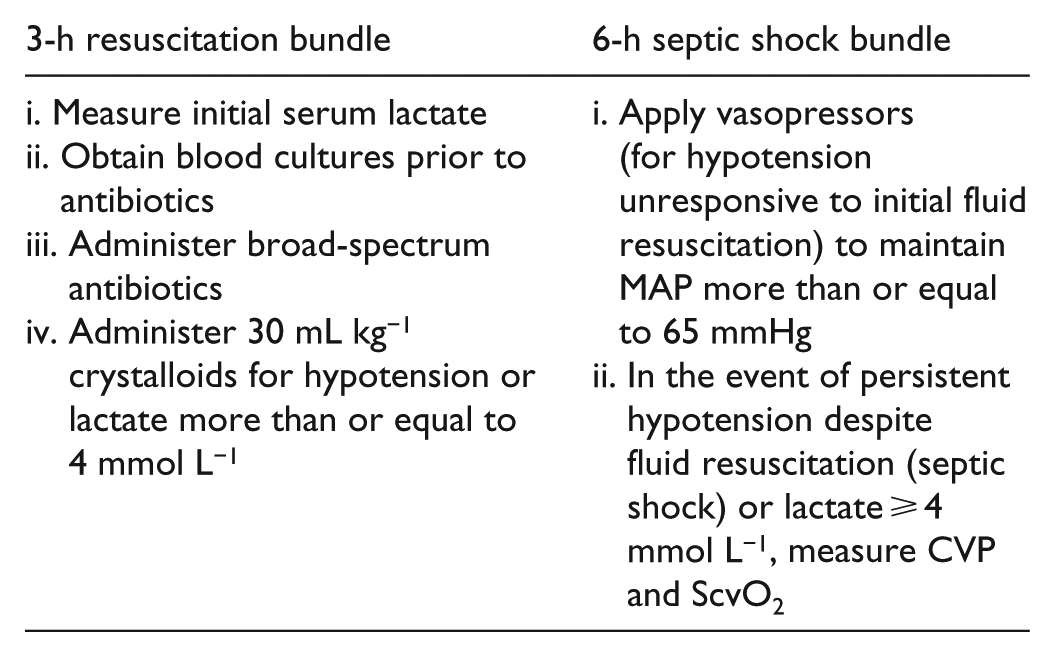
Bundles are the group of treatments that are built around the best evidence, and they have known to produce greater benefit when implemented together than as individual therapies. 41 Surviving Sepsis Campaign guidelines in 2008 incorporated sepsis resuscitation bundle to be achieved in 6 h and sepsis management bundle to be achieved in 24 h. In 2012, the 6-h resuscitation bundle was modified into two bundles: “the severe sepsis 3-hour resuscitation bundle” and “the 6-hour septic shock bundle,” which contain all therapeutic goals to be completed, respectively, within 3 and 6 h of presentation with septic shock. 42 In 2018, the 3- and 6-h bundles have been combined into a single 1-h bundle. 43
Despite implementation of Surviving Sepsis Campaign guidelines recommendations, there has been limited adoption of the care bundles in management of sepsis due to concerns about the external validity of the results, the complexity of the management, and the potential risks of central line placement required for measurement of CVP and ScvO2 monitoring.37,44 In 2014–2015, three large, multicenter, randomized controlled trials were performed in the United States (Protocolized Care for Early Septic Shock (ProCESS) trial), England (Protocolised Management in Sepsis (ProMISe) trial), and Australia (Australasian Resuscitation in Sepsis Evaluation (ARISE) trial). These studies showed that an early goal-directed protocol as described by Rivers et al. did not improve survival.37,39,44,45 Several systematic review and meta-analysis conducted thereafter also showed that EGDT did not reduce overall mortality.31,37 The most plausible explanation for this is the remarkable evolution of the usual standard of care.
Initial resuscitation
Sepsis and septic shock are medical emergencies. 39 Sepsis-induced tissue hypoperfusion is defined as acute organ dysfunction and/or persistent hypotension despite initial fluid resuscitation or blood lactate ⩾ 4 mmol L−1.35,46 Therefore, early aggressive fluid resuscitation forms the basis for stabilization of patients in severe sepsis/septic shock. Initial fluid resuscitation with crystalloids should be started to achieve minimum of 30 mL kg−1 of fluids in the first 3 h in patients with sepsis-induced tissue hypoperfusion.35,47,48 Despite lack of controlled data to support this volume and rate of fluid delivery, some interventional studies have described this as usual practice during initial resuscitation, and observed evidence supports this practice.46,49
After initial fluid resuscitation, further fluid management must be guided by clinical judgment based on ongoing reevaluation of the hemodynamic status (heart rate, blood pressure, arterial oxygen saturation, respiratory rate, temperature, urine output, and others as available). The use of CVP to monitor fluid resuscitation is no longer recommended.46,50
Crystalloid solution versus colloid solution in resuscitation
In sepsis, due to the release of several vasodilatory mediators, peripheral vasodilation and increased membrane permeability are observed. As a result, there is an intravascular fluid deficit. Studies have shown no clear benefit of resuscitation with colloid solutions over that with crystalloid solutions. 31 Cardiopulmonary resuscitation with hydroxyethyl starches (HES) showed an increased risk of acute kidney injury and need for renal replacement therapy in patients with severe sepsis and septic shock.51–53,54 One multicenter study found increased mortality rates in septic patients with 6% HES fluid resuscitation compared to Ringer’s acetate. 51 Thus, the evidence of harm observed with HES supported the recommendation against the use of this solution in severe sepsis and septic shock. 35 Gelatin was also found to be associated with increased mortality in one study. 55
Only albumin was found to be safe and as effective as isotonic saline.56,57 However, the Saline versus Albumin Fluid Evaluation (SAFE), Colloids Versus Crystalloids for the Resuscitation of the Critically Ill (CRISTAL), and Albumin Italian Outcome Sepsis (ALBIOS) trials did not show clear benefit with the use of albumin.56,58,59 Therefore, considering the increased cost of albumin and safety issues with the use of other colloids, Surviving Sepsis Campaign guidelines finally recommended crystalloids as the initial choice for fluid resuscitation for patients in sepsis.35,48 There is also low-level recommendation for intravenous albumin in fluid resuscitation for severe sepsis and septic shock when patients require significant amounts of crystalloids. 35
A meta-analysis in septic patients suggested that resuscitation with balanced crystalloids may be associated with a lower mortality rate than with normal saline. 55 However, there is limited evidence for choice of crystalloids in sepsis and septic shock.55,60
Vasopressors
Several factors in sepsis, such as volume depletion, low cardiac output, and/or inappropriate vasodilation, contribute to systemic hypotension and organ hypoperfusion. These lead to organ dysfunction in severe sepsis or septic shock. 61 While managing septic shock, it is crucial to restore and maintain adequate tissue perfusion. This can only be achieved with an adequate cardiac output and appropriate MAP. 61 MAP is the driving pressure of tissue perfusion. 46 Organ autoregulation tends to preserve the tissue perfusion over a range of organ perfusion pressure. Below this autoregulatory threshold, organ perfusion is linearly dependent on perfusion pressure. 62
When the initial fluid resuscitation fails to improve hypotension, vasopressors are used. 63 Most commonly used vasopressors in septic shock are norepinephrine, epinephrine, dopamine, phenylephrine, and vasopressin. Sepsis Occurrence in Acutely Ill Patients II (SOAP II) trial compared norepinephrine against dopamine in septic shock. The study observed that though there was no significant difference in mortality rates at 28 days, there were more adverse arrhythmic outcomes associated with dopamine. 64 De Backer et al. 65 in their meta-analysis found that dopamine use was associated with increased mortality compared to norepinephrine use. In another meta-analysis by Avni et al., 66 norepinephrine had more favorable hemodynamic profile (better urine output, decreased lactate levels, and increased CVP) than other vasopressors. Surviving Sepsis Campaign guidelines recommend norepinephrine as the vasopressor of choice for patients with septic shock. 46
The ideal MAP while managing septic shock is unknown. The Surviving Sepsis Campaign guidelines recommend an initial target of MAP of 65 mmHg in patients with septic shock requiring vasopressors. 46 The scientific basis for this recommendation comes from two different trials. Asfar et al. 67 in their multicenter, randomized trial concluded that there was no difference in all-cause mortality at 28 days or 90 days when targeting a higher MAP (80–85 mmHg) or a lower MAP (65–70 mmHg). Lamontagne et al. 63 in their Optimal Vasopressor Titration (OVATION) pilot trial found that lower MAP (60–65 mmHg) was associated with reduced mortality in patients aged 75 years and older. Thus, these formed the strong basis for favoring a lower MAP during initial management.
Lactate clearance
In sepsis, oxygen debt ensues because of the mismatch between the oxygen demand and the delivery with global tissue hypoxia. Despite early guidelines for goal-directed volume hemodynamic resuscitation and monitoring, the optimal end points for resuscitation remain uncertain. It is generally accepted that the use of structured set of hemodynamic end points such as pulse rate, blood pressure, mean arterial pressure, or urine output significantly improve hospital mortality. 68 However, measures to determine tissue oxygen delivery have remained controversial. Central venous oxygen saturation (ScvO2) or mixed venous oxygen saturation has been used to assess the balance of tissue oxygen delivery and consumption. 35 But need for specialty equipment, training, and the resources required to monitor ScvO2 has led to search for an alternative marker for defining resuscitation adequacy that is less invasive. 69
Serum lactate has been established as a prognostic tool in patients with septic shock. 70 It is now used as a more objective surrogate marker for tissue perfusion than physical examination or urine output. 46 Increase in serum lactate concentration above approximately 1 mmol L−1 is independently associated with organ failure and mortality.70–73 In sepsis, serum lactate of more than 4 mmol L−1 indicates severe disease with a high risk of death.35,74
Lactate clearance is defined as the rate of decline in lactate concentration, and this has been recommended as an end point in early goal-directed therapy in critically ill patients in sepsis.71,72 Significant reduction in mortality have been seen in lactate-guided resuscitation than without lactate monitoring. 46 Thus, early lactate clearance strategy of at least 10% is now favored over ScvO2 normalization strategy (LACTATES TRIAL). 68
However, in recent times, the idea of resuscitation based on lactate clearance has been challenged. Marik et al., in their critical review on lactate clearance, have suggested that titrating treatment according to blood lactate level may be counterintuitive. The blood lactate elevation reflects the severity of illness and degree of activation of stress response than just anaerobic metabolism. Thus, fall in lactate concentration following treatment is likely due to improvement in the stress response than correction of oxygen debt. 71
Blood transfusion in severe sepsis
In sepsis, organ dysfunction is attributed to insufficient tissue perfusion and oxygen delivery. It seemed logical that such patients would benefit from packed red cell transfusion. However, this has been a subject of great debate as the benefit and harms of different hemoglobin thresholds are not clearly established.75,76
Patients with septic shock receive frequent blood transfusions. The Transfusion Requirement in Septic Shock (TRISS) trial defined the hemoglobin threshold for blood transfusion as it has been associated with increased mortality in subgroups of critically ill patients.76,77 This trial showed that the 90-day mortality, ischemic events, and use of life support were similar between the higher hemoglobin threshold group (9 g dL−1) and the lower hemoglobin threshold group (7 g dL−1). The lower threshold group received significantly less units of blood transfusion. In the subgroup analysis, the results were similar for cardiovascular disease, older age, or greater disease severity. Several other studies, like the ProCESS trial and Transfusion Requirement in Critical Care (TRICC), have shown similar results as the TRISS study. 78 There is strong evidence favoring a lower hemoglobin threshold for blood transfusion in septic shock. 79 Thus, it has been recommended that the RBC transfusion should occur only when hemoglobin concentration is <7 g dL−1 in adults in the absence of myocardial ischemia, severe hypoxemia, or acute hemorrhage. 46
Management of infection
An essential component of the initial management of sepsis is the prompt commencement of appropriate antibiotic therapy and source control. Choosing an appropriate regimen is often challenging and is influenced by a number of determinants including, but not limited to, previous infections and antibiotics received, local patterns of pathogen activity and antibiotic susceptibility, major clinical comorbidities, and underlying clinical syndrome. Pathogens most commonly associated with sepsis-related mortality were gram-positive cocci, followed by gram-negative bacilli. 80 Appropriate antibiotic therapy is defined as the use of at least one antibiotic with in vitro activity against the causative bacteria. Kumar et al. demonstrated a clear association between a delay in effective antibiotic initiation after the onset of hypotension and in-hospital mortality. Each hour of delay was associated with a decrease in survival of approximately 7% on average. The administration of antibiotics within the first hour of recognition of sepsis or septic shock resulted in survival rates of up to 80%. 81 A retrospective cohort study of 760 patients admitted with severe sepsis and septic shock associated with gram-negative bacteremia demonstrated a statistically greater hospital mortality rate among those with inappropriate initial antibiotic therapy. 82 In addition, patients treated with an empiric combination antibiotic regimen active against gram-negative bacteria produced increased rates of appropriate initial antibiotic therapy when compared to monotherapy. This study suggested that aminoglycosides provided broader coverage than fluoroquinolones when combined with β-lactams such as piperacillin-tazobactam or cefepime. A moderate degree of suspicion should also be maintained for possible fungemia (specifically candidemia) in critically ill patients with persistent fevers despite empiric antibiotic therapy. The Infectious Diseases Society of America (IDSA) recommends initiation of empiric antifungal therapy with either an echinocandin or fluconazole in such cases. 83
A large meta-analysis of 64 clinical studies (n = 7586) by Paul et al. 84 found no difference in hospital mortality or the development of resistance in patients treated with monotherapy as compared to combination antimicrobials in sepsis. The current recommendations from the Surviving Sepsis Campaign are to limit empiric broad-spectrum therapy to 3–5 days except in specific cases such as neutropenic patients and in known multidrug-resistant pathogens, such as Acinetobacter and Pseudomonas, where a longer duration of empiric combination antibiotic therapy may be warranted. 82 Ultimately, the choice of empiric antibiotics is a patient-specific decision with input from local antibiotic susceptibility patterns and recommendations from the antibiotic stewardship committee.
Also integral to the successful management of sepsis is source control. It refers to any physical or surgical measure that can be used to control a focus of infection or alter the determinants promoting the spread or persistence of infection. 85 This can include anything from the drainage of infected fluid collections and the removal of potentially infected devices (e.g. central venous catheters) to the resection and anastomosis of a perforated bowel. With a few exceptions (infected pancreatic necrosis), current guidelines recommend the rapid institution of source control measures following initial resuscitation in all cases where there is a definite focus of infection that is amenable to such measures. 86 This is especially crucial in the setting of necrotizing soft tissue infections (NSTIs). One study showed that the mortality rate increased by 27% for each day of delay in surgical removal of infected tissue in NSTI patients presenting with sepsis. 87 An optimum source control method is chosen on the basis of a risk/benefit analysis of the intervention. Recent advances in radiological techniques and the development of percutaneous interventions have offered what is sometimes an equally effective and less invasive surgical alternative to source control. 88 Improvement in diagnostic modalities have also allowed for the early detection of clinically occult foci of infection.
Role of procalcitonin
Procalcitonin has received significant attention over the last two decades as a biomarker for sepsis. It is a precursor of calcitonin—a regulatory hormone involved in calcium homeostasis. It is usually undetectable in healthy individuals. Although the physiological role of procalcitonin has not yet been established, it has been suggested that it is produced by hepatocytes and macrophages in response to certain inciting factors like infection, trauma, surgery, and cancer. 89 It was first reported to be associated with the severity of pediatric infection by Assicot et al. 90 Since then, there has been significant interest and investigation of the different clinical applications of procalcitonin, including its use in diagnosis and prognosis of patients with severe infections. Evidence suggests that the procalcitonin level is a practical biomarker for the early diagnosis of sepsis but must be used in conjunction with other clinical evidence. 91 There is also evidence to suggest that there is an association between procalcitonin levels in early sepsis and survival. 92 However, this has not translated into any definite improvement in therapeutic decision making.
In 2010, the PRORATA trial demonstrated a decreased duration of antibiotic therapy in critically ill patients managed according to a procalcitonin level-guided antibiotic treatment algorithm, without a significant mortality benefit. 93 A recent systematic review appears to confirm the above conclusions with procalcitonin-based antibiotic algorithms showing no discernible effect on mortality but a significant reduction in duration of antimicrobials. 94 As such, there is still no consensus on the use of a procalcitonin-driven treatment protocol. The lack of a benefit on mortality, duration of inpatient and ICU stay, and rates of C. difficile colitis further limit the use of such strategies in the critical care setting.
Markers of adverse outcome
As part of the Protein C Worldwide Evaluation in Severe Sepsis (PROWESS) trial completed in 2004, an analysis was performed of 19 biomarkers that are associated with systemic host response in sepsis and their relation to disease severity and outcome. 95 It did demonstrate significant correlations between general markers of coagulopathy and inflammation such as plasminogen activator inhibitor-1(PAI-1), D-dimer, prothrombin time (PT), activated partial thromboplastin time (APTT), thrombin-activatable fibrinolysis inhibitor (TAFI), and protein C and others (IL-6, IL-8, IL-10) with the severity of sepsis as measured by the Acute Physiology and Chronic Health Evaluation (APACHE) II score. Baseline levels and change in levels of these markers over the course of the disease indicated that 28-day survival in severe sepsis is associated with decreased inflammation, endothelial injury, and thrombin generation, as well as the replenishment of anticoagulant factors. Another study that looked specifically at thyroid function tests as potential predictors of poor outcome in sepsis failed to demonstrate any prognostic effect of the thyroid function panel. 96 Mesters et al. 97 examined PAI levels in sepsis occurring in leukocytopenic patients and found that PAI activity measurements were a sensitive marker of an unfavorable prognosis. Plasma BNP concentration has been found to function as a reliable biomarker for the identification of patients developing sepsis-induced myocardial depression. 98 More specifically, BNP levels on day 5 can be an effective prognostic marker to identify patients with elevated risk for an adverse outcome. At present, there is no single test that can be said to predict mortality with a high degree of sensitivity and specificity. The above described markers are still not ready to be deployed widely in various clinical settings.
Newer modalities of treatment
As discussed above, the severity of sepsis and the outcomes in sepsis and septic shock are dependent on the nature of infection and the inflammatory response it provokes. This has led to the development of targeted agents that limit the inflammatory and coagulatory cascade while preserving their benefits. The most well-known and widely used class of immunomodulatory agents is glucocorticoids, which have a generalized depressant effect on immune and vascular response to infection. Newer, more targeted modalities aimed at specific components of these pathways have been developed over the last two decades. One of the more promising of these agents had been recombinant activated protein C or drotrecogin α. Protein C is an endogenous protein produced as part of the coagulation cascade and its activated form has shown in vitro anti-inflammatory effect via the inhibition of TNFα, IL-1β, and IL-6, as well as limiting of neutrophil and monocyte adhesion to the endothelium. 99 In addition, it diminishes the procoagulant and antifibrinolytic response in SIRS. The PROWESS trial appeared to show an improved survival (28-day mortality of 24.7% vs 30.8% with placebo) when drotrecogin α was administered to patients with severe sepsis, but this was controversial given concerns over study design and side effects (especially bleeding). 100 The drug was still provisionally approved by the Food and Drug Administration (FDA) (as Xigris) in patients with severe sepsis and a high risk of death. However, follow-up studies on the drug, such as ENHANCE, ADDRESS, and especially the PROWESS-SHOCK trial, unequivocally demonstrated no mortality benefit in patients with severe sepsis, and it was eventually withdrawn from the market in 2011.101,102
Tumor necrosis factor-α (TNFα) has also been the subject of targeted therapy given its integral function in biochemical signaling in the inflammatory cascade. Series of trials, both national (NORASEPT and NORASEPT II) and international (INTERSEPT)evaluating the efficacy of a monoclonal antibody against TNF in sepsis were conducted in the 1990s.103,104 However, they failed to show any demonstrable improvement in mortality. In 2012, AstraZeneca decided to stop further development of Cytofab (a polyclonal ovine anti-TNF antibody) after failure of the drug to show improvement in primary end points (ventilator-free ICU days or mortality) in a Stage IIB trial (ClinicalTrials.gov number NCT01145560). Other agents including platelet activating factor(PAF) and IL-1 receptor antagonists have also failed to show significant benefit.
A combination of vitamin C, hydrocortisone, and thiamine as an adjunctive therapy in sepsis has shown promising results in recent experimental and clinical studies. Vitamin C is known to have antioxidant properties, hydrocortisone has a known theoretical synergistic effect with vitamin C, and thiamine prevents vitamin C crystallization at high doses. A retrospective study published in Chest in 2017 105 demonstrated a reduction in overall sepsis mortality (8.5% versus 40.4% in non-treated group) in septic shock patients who were treated with the vitamin C regimen. It was also noted to facilitate the more rapid weaning of vasopressors and prevented progression of multiorgan dysfunction, especially acute kidney injury. However, prospective, multicenter, randomized clinical trials are still required before proper recommendations on the use of the vitamin C protocol in sepsis can be issued. However, given the promising results with what are inexpensive, relatively safe and readily available medications, further investigation is certainly warranted.
Another novel therapy aimed at mitigating the effects of the sympathetic adrenergic response in sepsis is short-acting β blockade therapy with esmolol. A meta-analysis of five randomized controlled trials (RCTs) on this subject by Liu et al. 106 did show that esmolol infusion was able to significantly increase survival rate (Relative risk = 2.06, p = 0.006) and decrease heart rate and troponin I.
The use of polyclonal intravenous immunoglobulins (IVIg) has been studied over the last two decades with a number of clinical trials aimed at assessing their efficacy in sepsis and septic shock. A recent Cochrane meta-analysis of these trials 107 has been unable to demonstrate a clear and definite mortality benefit with the use of polyclonal immunoglobulins in well-designed trials. Only the trials designated with a high-risk of bias appeared to show a mortality benefit. Trials involving IgM-enhanced polyclonal immunoglobulin therapy did appear to show some reduction in mortality (28-day mortality of 24.7% in IVIgM-enhanced group versus 37.5% in placebo group, relative risk (RR) of 0.66, 95% confidence interval (CI): 0.51–0.85). These trials have been limited by their small size and significant heterogeneity. The only large-scale clinical trial involving IVIg 108 did not show any mortality benefit with its use. Based on the above, the Surviving Sepsis Campaign guidelines of 2016 recommend against the use of intravenous immunoglobulins in sepsis.
Blood purification through the removal or inactivation of endotoxins and inflammatory cytokines has also been investigated to determine if it can be used as additional supportive therapy in sepsis. The most studied method is hemoadsorption, in which blood is passed through adsorbent membranes (most commonly polymyxin B) for the removal of endotoxins. A systematic review 109 did show that this technique improved mortality in sepsis with polymyxin B (PMX-B) hemoadsorption (RR, 0.57; 95% CI, 0.45–0.72; p < 0.001). However, the mortality data seems to be heavily weighted by polymyxin B hemoadsorption studies from Japan. Other smaller, non-blinded trials have shown no benefit. A recent, blinded multicenter RCT evaluating PMX-B hemoadsorption in sepsis called the EUPHRATES trial is currently ongoing. Other techniques of blood purification include plasma exchange in which plasma is separated from whole blood, removed, and then replaced with crystalloids and coupled plasma filtration adsorption (CPFA) which is a combination of plasma filtration and hemadsorption. CPFA did not show a beneficial effect on hospital mortality or other end points like organ dysfunction in septic shock. 110 Due to the above limitations, there are no current official recommendations for or against blood purification techniques by the Surviving Sepsis Campaign group.
Immunostimulation is another potential area for future drug development. Immunostimulatory therapy is predicated on the theory that sepsis and critical illness produces an immunosuppressed state and the resulting nosocomial infections contribute significantly to overall mortality. In a small study of nine patients, Docke et al. 111 demonstrated restoration of monocyte function and resolution of sepsis in eight of them, indicating potential usefulness of type II interferon (IFNγ) therapy in selected septic patients. Granulocyte colony-stimulating factor(G-CSF) therapy is known to augment neutrophil function and number and thereby enhance the immune defenses of the host. However, multiple studies have found no overall benefit in G-CSF therapy in patients with pneumonia and sepsis.
Conclusion
Sepsis remains a significant burden on health systems worldwide. However, the advances made in understanding its pathogenesis and the extensive efforts at framing guidelines for its effective management in the last 20 years exceed anything that has been done before. There has been no magic bullet for the management of sepsis. However, measures such as prompt use of antibiotics and hemodynamic resuscitation, appropriate ventilator use, and judicious transfusion of blood products have played a significant role in decreasing morbidity and mortality. The use of newer, precision modalities like immunomodulators, while currently in a nascent stage of development, offer a promising field of inquiry. Development of scores such as the APACHE-II and sequential organ failure assessment (SOFA) have provided simple but useful clinical tools in the assessment and prognostication of sepsis. The definition of sepsis continues to be a contested subject with the latest guidelines abandoning the previously used SIRS criteria and proposing a more complex definition based on multiorgan dysfunction and SOFA scores. It is hoped that this will improve the accuracy of sepsis diagnosis for clinical, epidemiological, and hospital coding purposes. It remains to be seen if there will be wider adoption and implementation of these recommendations by healthcare facilities and providers.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.