
Abstract
This case report presents an uncommon case of misdiagnosed groin pain in an elderly individual, highlighting the complexities of diagnosing overlapping symptoms in aging populations. With a growing elderly population, healthcare professionals must navigate complex medical histories to provide accurate diagnoses and effective treatment. This case emphasizes the importance of interdisciplinary collaboration and cost-effective diagnostic tools in delivering patient-centered care. We describe the case of an 87-year-old male with a history of heart disease and coronary angiography, who developed groin pain. After excluding a hernia, the patient was referred to our department for further evaluation. Through a thorough medical history and diagnostic tools, including computed tomography (CT) scan and intraarticular infiltration, the underlying cause of the pain was accurately identified and treated. An 87-year-old male with heart disease and previous coronary angiography presented with groin pain. Initially evaluated elsewhere for a potential hernia, the patient believed a foreign body in his muscles was the source of his pain. However, a planning X-ray failed to reveal this. Upon referral, a thorough medical history was taken, and a CT scan was performed to locate the foreign body and assess its proximity to the femoral nerve. The CT scan confirmed a broken angiography catheter (3–40 mm) near the femoral nerve. Additionally, severe fourth-grade coxarthrosis was identified. Despite the patient’s belief that the foreign body caused his pain, we determined coxarthrosis was the main issue. An intraarticular infiltration provided pain relief, confirming the diagnosis, and a total hip arthroplasty with catheter removal was performed, resulting in complete pain relief. This case underscores the need for thorough evaluation and interdisciplinary collaboration in diagnosing complex conditions in elderly patients. Intraarticular infiltration remains a valuable diagnostic tool, even alongside advanced imaging, helping prevent unnecessary procedures and improving patient outcomes.
Keywords
Introduction
With the aging patient population, healthcare professionals encounter more complex medical histories and challenging diagnostic cases. The elderly population is more susceptible to various medical conditions, which can cause overlapping symptoms and lead to diagnostic dilemmas. Understanding their interplay is crucial for accurate diagnosis and appropriate treatment. Misdirected patient admissions due to diagnostic errors can have fatal consequences. Avoidance of musculoskeletal hospital-based services due to age or a lack of knowledge highlights the importance of interdisciplinary and multiprofessional collaboration, correct triage, and the use of cost-effective diagnostic tools in the hands of specialists to provide effective and appropriate treatment to patients in need.1–4
Case description
Here, we describe the evaluation and management of an 87-year-old male with groin pain, who was presented to the surgeons by the general practitioner. Initially, the patient presented with groin pain radiating to the thigh and medial aspect of the leg, accompanied by restricted mobility. Notably, there was no palpable mass in the inguinal region upon clinical examination. Further clinical examination revealed a slight limitation in internal rotation, accompanied by mild pain at the end range of motion, with internal rotation measured at 15°. In comparison, the internal rotation of the contralateral hip was 20°.
Mildly obese, the patient was thought to have a hernia. Among other issues, the patient had a history of heart disease and had previously undergone coronary angiography. He knew very well of the presence of a foreign body due to the breakage of the catheter.
In order to rule out an inguinal hernia, aneurysm spurium following coronary angiography, irritation due to the yet not confirmed foreign body and other abdominal differential diagnosis, a computed tomography (CT) was ultimately performed. The CT scan revealed the presence of a broken part of the angiography catheter, measuring 3–40 mm in size and located at least 1.4 cm away from the femoral nerve and vessels, with no scare tissue irritating the major structures. There was no sign for an aneurysm or an inguinal hernia. However, coxarthrosis was identified as a further differential diagnosis.
Patient and general practitioner were not convinced that coxarthrosis could be the leading reason for the groin pain since the pain only came after the coronary angiography. Furthermore, the occurrence of painful coxarthrosis at the age of 87 seemed unlikely, especially because the patient denied any restriction in walking. They were certain that the foreign body or a possible hernia were responsible for the groin pain. However, before groin revision, the general surgeon wanted to obtain the opinion of an orthopedic surgeon.
Again, the patient had to undergo a thorough medical history and clinical examination. The onset of groin pain was far after the coronary angiography. Immediately after the coronary angiography and the breakage of the catheter, there were no signs of bleeding complications, irritations of the femoral nerve or problems with blood supply. Nevertheless, irritation from later developed scar tissue remained an explanation for his pain.
The patient revealed to have problems with mobilization, but thought it was due to his age. His radius of movement had decreased over the years, but no hip-associated pain was obvious. However, he admitted to have problems getting up in the morning or after standing up after sitting on a chair for a longer period. He was well adapted and accustomed to his coxarthrosis.
Clinical exams revealed no palpation pain, but immediate aggravation of his yet mild hip complaints with internal rotation of the flexed hip. Movements in the hip were only possible in flexion and extension with limited range of motion, abduction, and adduction were suspended.
Radiographs did not show the foreign body; it was hidden by the femur corticalis. However, there was a severe case coxarthrosis (Figure 1). The CT scan showed no impingement due to the foreign body, no other relevant diagnosis to explain the pain other than severe coxarthrosis (Figures 2 and 3). In summary, a long lasting but clinically mute coxarthrosis was the reason for the pain. The patient adapted over the years to his increasing restriction in range of motion while his heart problems got predominant in his daily life.

Plain radiographs of the pelvis in ap and axial view with the catheter hardly visible in anatomic relation to the right hip joint with a fourth degree coxarthosis.

CT with multiplanar reconstruction showing the catheter in relation to the major vessels. No aneurysm or hernia was detected. Again, the recognizable coxarthrosis on both sides.
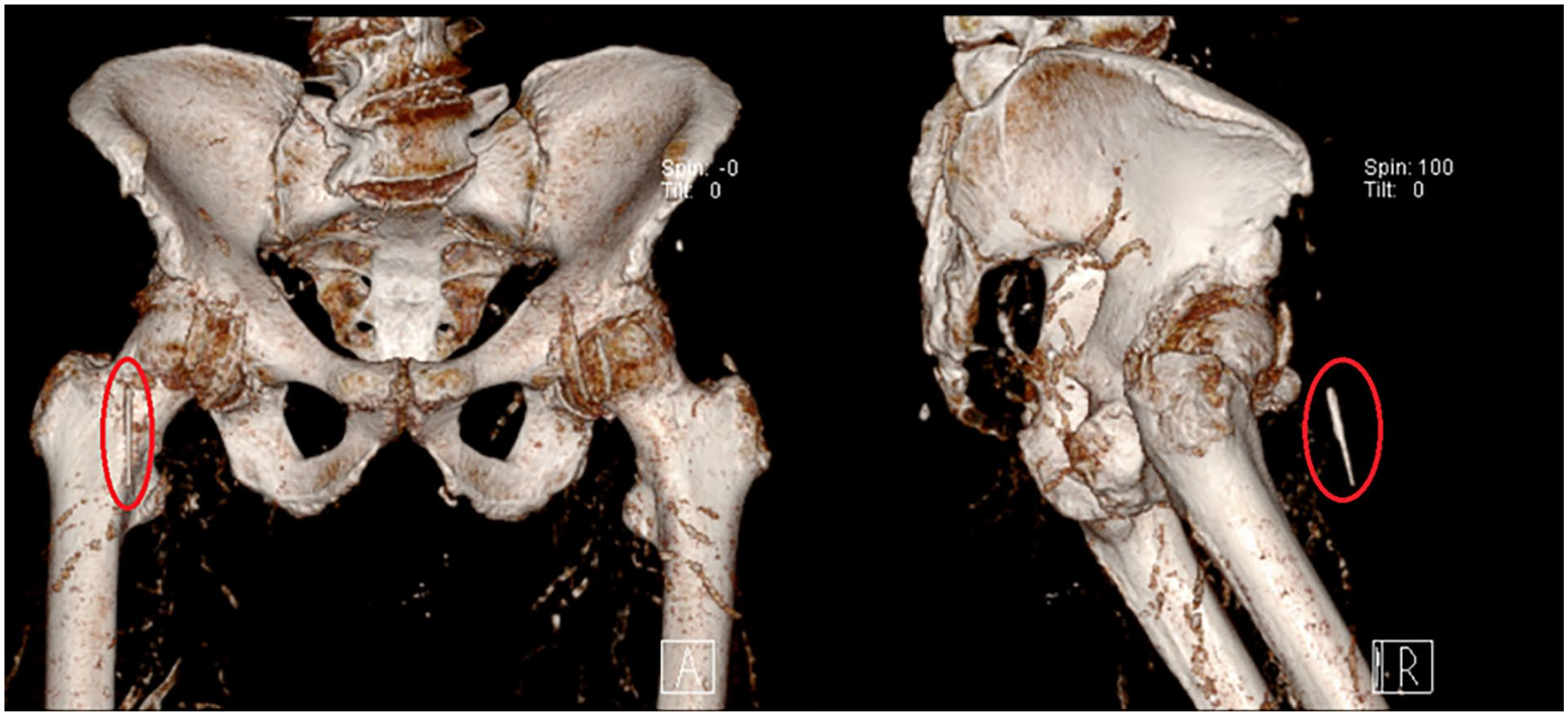
3D reconstruction for better visualization of the broken catheter part (the red circle indicates the catheter).
So, in addition, an intraarticular infiltration with local anesthesia was performed to provide immediate pain relief and to further evaluate the patient’s condition (Figure 4). Finally, an interdisciplinary case discussion led to the result that total hip replacement without further diagnostic tools was the best option for the patient. Groin revision, hernia repair, and foreign body removal was ruled out as appropriate treatment options. However, the patient agreed to hip replacement however, only accepting the procedure with additional removal of the foreign body (Figures 5 and 6).

Plain radiograph pelvis AP documenting the correct infiltration with Ropivacain.

Plain radiograph directly after performing the total hip replacement.

Broken catheter tip after removal.
Discussion
Misdiagnosis of groin pain in elderly patients is a well-recognized clinical challenge, particularly when distinguishing between inguinal hernia and hip osteoarthritis. Both conditions frequently present with overlapping symptoms such as groin pain, reduced mobility, and discomfort during weight-bearing activities. In elderly individuals, degenerative changes in the hip joint are common, which may lead to a bias toward diagnosing hip pathology, while subtle inguinal hernias—especially those without a palpable mass—may be overlooked. Conversely, a hernia may mimic intra-articular hip disease, leading to delays in the correct diagnosis and appropriate management. This overlap highlights the importance of a thorough clinical examination, detailed patient history, and appropriate use of imaging modalities to avoid misdiagnosis and ensure timely and effective treatment.
Collaboration in interdisciplinary and/or multiprofessional teams or boards is a well-accepted concept in medicine. There are interdisciplinary wards and specialized centers with certified structures and programs where, for example, visceral surgeons and gastroenterologists together care for their patients, discuss treatment options, and clinical pathways. Centers like these are an answer to the increasing complexity of cases and diversity of treatments, with the aim to find the best individual help. These centers are normally hospital-based with adjunct outpatient ambulatories.
With the aging population, more complex medical situations become a challenge for healthcare professionals. These patients are mostly treated in the outpatient setting to reduce complications like hospital-acquired infections or delirium. Overlapping, misinterpreted, or symptoms masked by medication, patient self-assessment, adaptation, and habituation may lead to diagnostic challenges and dilemmas, leading to a variety of doctor contacts. However, this is still no guarantee for the right treatment and is often combined with increased costs and time.
This case serves as a statement highlighting the importance of interdisciplinary collaborations in the outpatient setting for the older population. It is crucial to have a well-established network of specialists and general practitioners for optimal and cost-effective evaluation of patients. Such frameworks are ideally spatially located next to each other.
Our collaboration with general practitioners and being a multidisciplinary hospital team with a highly frequented outpatient clinic allows us to establish a network that fosters earlier detection of health issues in elderly and morbid patients. This can be time-saving and reduces doctor contacts as well as costs. The essence of cooperation lies in the development of personalized care plans for each patient. General practitioners, who often have long-standing relationships with their patients, can contribute vital insights into the patient’s medical history, preferences, and unique needs. Multidisciplinary hospital teams can then tailor their treatment strategies to optimize outcomes.
Timely intervention can prevent complications, reduce hospital readmissions, and enhance the quality of life for these individuals.
In this case, the patient had multiple doctor contacts before he came to our outpatient clinic, leading to different clinical and diagnostic investigations with plain radiographs and a CT scan. The CT scan finally confirmed the presence of a foreign object, which later appeared to be a broken part of the angiography catheter, and revealed the presence of a severe case of coxarthrosis (Figure 2). The patient’s detailed personal history revealed almost all signs of coxarthrosis, including starting pain after rest, pain after 20 min of exercise, restricted motion, and limping, without any signs of sensorimotor disorders.
Despite the patient’s certainty that his pain was due to the foreign particle, we were able to convince him, due to intra-articular infiltration, that the main cause of his pain was his coxarthrosis. The infiltration provided immediate pain relief, and the patient reported significant improvement in his symptoms thereafter, leading to the decision to perform a total hip arthroplasty with the removal of the foreign object in one procedure (Figures 5 and 6).
The challenge in this case was to find the true cause of the complaints and then to convince the patient of the benefits of a hip prosthesis. Intra-articular infiltration was of the utmost importance here. Right after the procedure, the patient was pain-free, and his walking abilities increased with time. At 6 weeks follow-up, his general condition and his mobility had increased remarkably, no longer needing crutches, with a pain-free walking time of 60 min (Figure 7).

Plain radiograph pelvis AP and hip axial by the follow up 6 weeks after the operation.
Conclusions
As the population ages, we are likely to encounter more patients with complex medical histories, and overlapping symptoms could lead to unnecessary operations. This case highlights the importance of thorough evaluation and collaboration among healthcare professionals in multidisciplinary and multiprofessional teams when diagnosing complex medical conditions in older patients. Interdisciplinary collaboration among healthcare professionals is crucial to differentiate between different types of pain, lead to correct diagnosis, and ultimately save money in modern healthcare systems. Collaborative care models between general practitioners, specialists in private practice, and multidisciplinary hospitals can take a holistic approach by considering all aspects of a patient’s health, leading to more comprehensive and patient-centered care. Intra-articular infiltration prior to joint replacement remains a valuable and cost-effective diagnostic tool, even in the era of advanced imaging techniques such as MRI and SPECT-CT.
Footnotes
Acknowledgements
Our sincere appreciation is extended to Mrs. Tamara Horn Lang for her invaluable support in refining the manuscript, offering indispensable writing and providing astute critical remarks.
Ethical considerations
Ethics committee approval is not required for the presentation of a case report derived from a retrospective analysis and the progression of a patient’s medical history.
Consent to participate
This certifies that the patient has voluntarily provided written informed consent to participate in the study, including permission to disclose radiological examinations. The patient affirms that they have been fully informed about the study’s purpose, procedures, potential risks, and anticipated benefits, and that they understand this information.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.