
Abstract
Atrioventricular canal defects constitute about 3%–5% of total congenital heart defects, with a prevalence of 0.3–0.4/1000 live births. Mitral valve defects are associated with atrioventricular canal (septal) defects in most cases. Our case is of a 37-year-old male who underwent double patch closure of atrial and ventricular septal defects at the age of 24 years, now presenting with NYHA-III symptoms of severe mitral regurgitation and severe tricuspid regurgitation. The mitral valve was of atrio-ventricular canal type. We repaired both mitral and tricuspid valves using soft rings. Because of a deformed annulus, a soft ring was preferred.
Introduction
Atrioventricular (AV) canal defects constitute about 3%–5% of total congenital heart defects, with a prevalence of 0.3–0.4/1000 live births. Mitral valve (MV) defects 1 are associated with AV canal (septal) defects in most cases. Both complete and partial AV canal defects can be related to MV defects of varying severity since birth, starting from ‘small cleft to severe dysmorphism,’ causing severe mitral regurgitation (MR) or stenosis. Loss of β-catenin, 2 deletion of FRS2ά, 3 and ERP44 4 result in hypoplastic endocardial cushions due to reduced cell proliferation and impaired cell migration. Late presentation is not uncommon in incomplete AV canal defects, though rare in complete AV canal defects. MV and tricuspid valve (TV) regurgitation, 5 requiring reoperation after the repair of AV canal defect, happened in 5%–7% 6 of cases. Sometimes MV defects do not require any intervention at the time of the first corrective surgery of AV canal defect, but later in life, there is a need for redo surgery to correct that defect.
Case presentation
Our case is a 37-year-old male 7 who underwent double patch (Dacron, Getinge (Maquet) and Gore) closure of atrial and ventricular septal defect at the age of 24 years. He now presented with complaints of chest pain and easy fatigability (NYHA-III), for 1 month. On examination, pansystolic murmurs (grade 4/6) were present at the mitral and tricuspid areas. ECG and X-ray findings were correlated with severe MR and tricuspid regurgitation (TR). 2D-ECHO and transesophageal echocardiography (TEE) showed prolapse of both the anterior mitral leaflet (AML) and posterior mitral leaflet (PML) leading to severe MR, dilated tricuspid annulus (4.3 cm) leading to prolapse of the TV leaflets with moderate to severe TR. Global left ventricular (LV) hypokinesia was noted, with an Left Ventricular Ejection Fraction (LVEF) of 50%, and impaired Right Ventricle (RV) function (TAPSE [Tricuspid Annular Plane Systolic Excursion] 8.5 cm). All four chambers were dilated (LA [Left Atrium] /LV 5.8/5.4 cm). Coronary angiography showed normal coronaries. The patient underwent repair of both MV (trans-septal) and TV on CPB with an aortic cross-clamp time (ACCT) of 120 min. Intraoperatively, there were dense adhesions on all the surfaces and borders except diaphragmatic surface, there was a calcified atrial septum (Figure 1) with distorted and dysmorphic large mitral annulus with enlarged AML, PML, chordae, and MV commissures with two MR jets (Figure 2). The MV was of AV canal type. There was a large superior bridging leaflet component, medial part, prolapsing (Figures 3 and 4), and a small inferior bridging leaflet component (Figure 5). Nineteen annular sutures were taken, and the papillary muscle subtending the medial part was repositioned using Cardio Vascular Suture made up of Gore-tex material (CV) sutures on pledgets. The cleft between the superior and inferior bridging leaflets was closed, and a 29-mm annuloplasty (SJM Tailor, Abbott) ring was placed (Figure 6). In the TV, leakage was present at the place where the Ventricular Septal Defect (VSD) patch was present, and the leaflets were getting adhered at that place. The anterior tricuspid leaflet was rotated to meet the septal leaflet at the anteroseptal commissure and stitched with 6/0 prolene. A 31-mm SJM Tailor ring was placed. Intraoperative and immediate postoperative TEE showed adequately repaired MV with peak gradient (PG) and mean gradient (MG) of −7/4 mm Hg and TV with PG/MG 2.6/1.5 mm Hg, no residual MR and TR, Pulmonary artery systolic pressure (PASP) 24 mm Hg, LVEF 45%. The patient remained clinically and hemodynamically stable in the perioperative period. The initial rhythm was junctional, which converted to sinus on postoperative day 1. Postoperatively, tachycardia and pulmonary artery pressure were managed with beta-blockers, low-dose milrinone, and a nitroglycerine infusion. He got symptomatic relief after surgery, and at the time of discharge (sixth postoperative day), he was asymptomatic. Echocardiographic findings remained roughly the same even at 3- and 6-month follow-ups.

Transesophageal imaging showing the calcified patch and septum of previous surgery (marked with arrow).
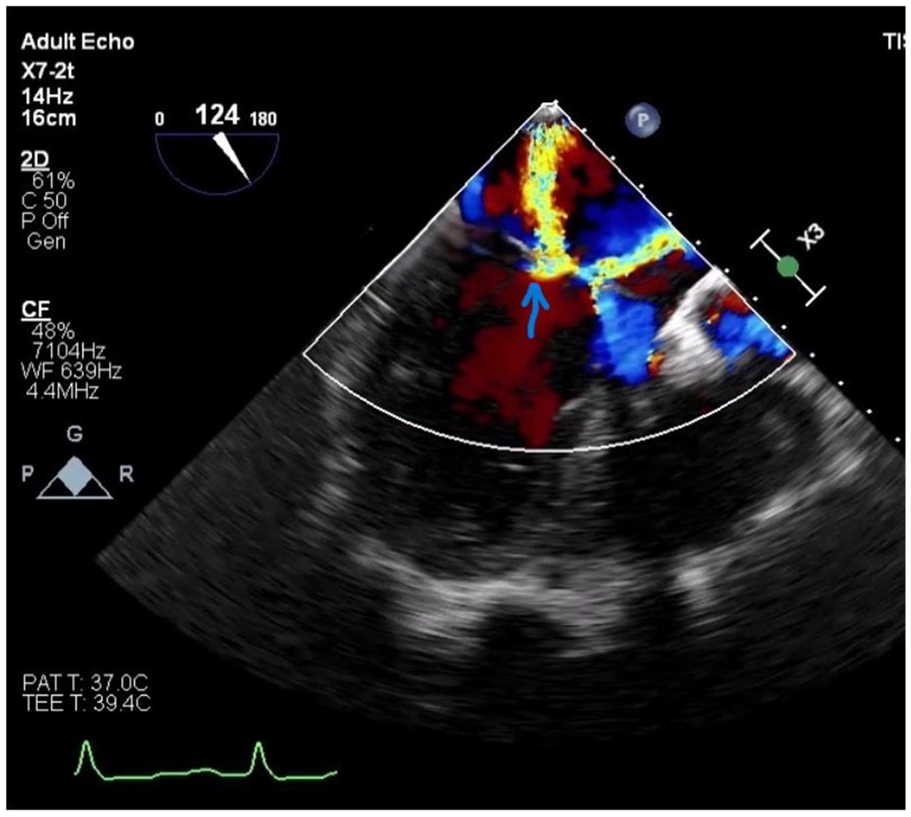
Two mitral regurgitation jets (marked with arrow) visible on TEE.

Dynamic prolapse of AML visible on 77° angle in TEE (marked with arrow).
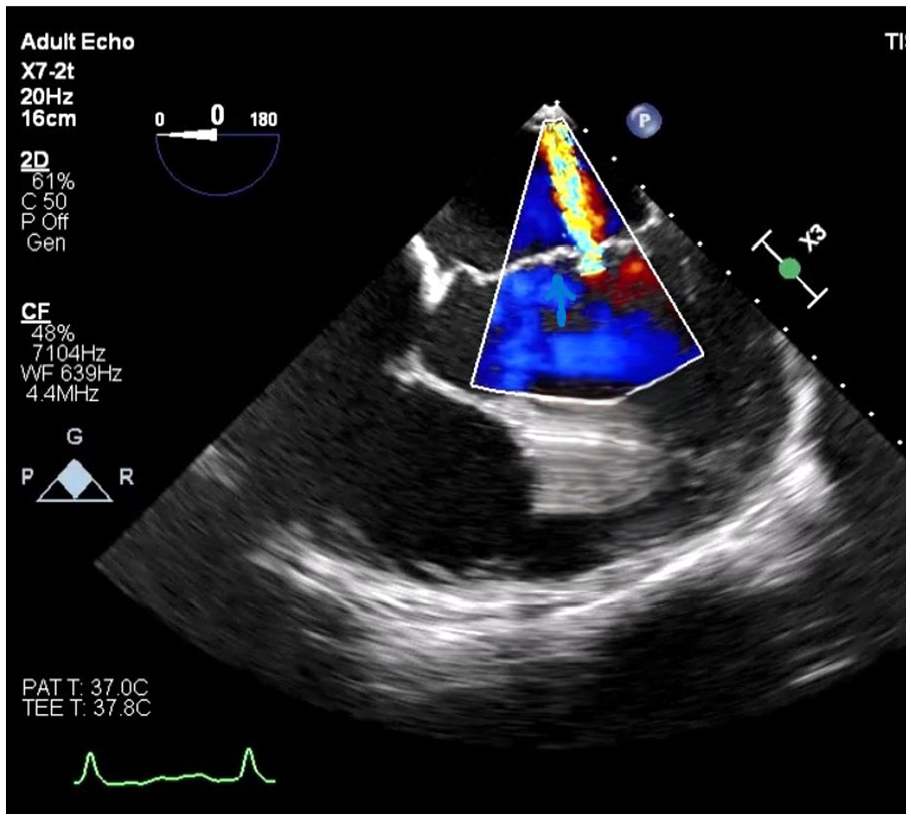
AML without prolapse on TEE at 0° with a single jet of mitral regurgitation (marked with arrow).
Intraoperatively prolapsed AML (marked with arrow) on saline test.

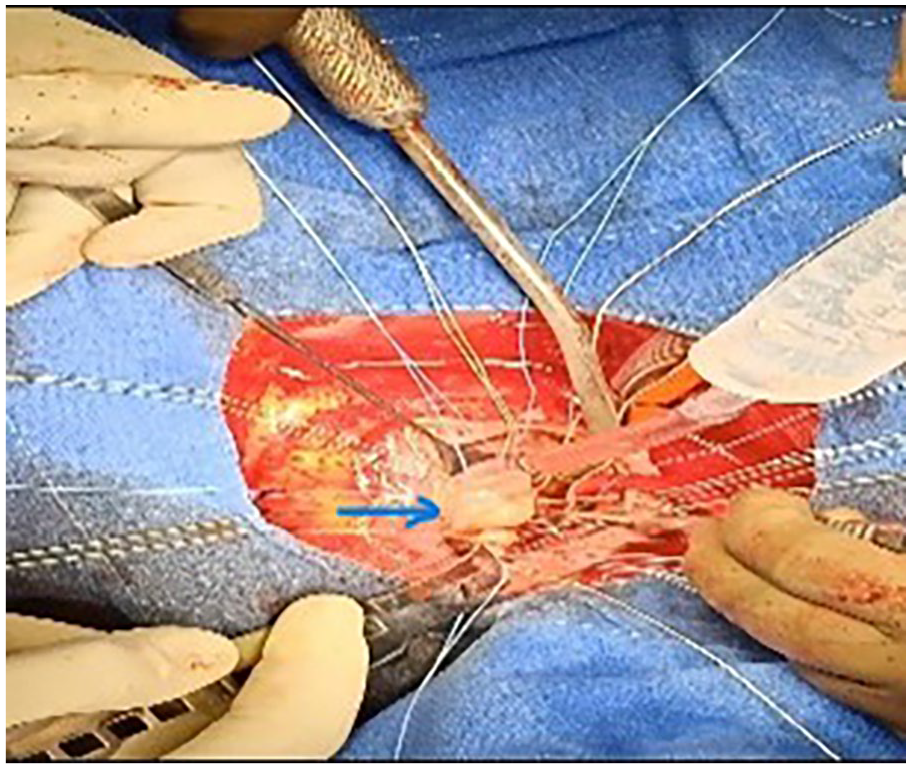
Post repair soft ring in situ (marked with arrow) at mitral position.
Discussion
Usually, annuloplasty or valve replacement is not recommended in AV canal type of MV because of the absence of a fibrous skeleton (endocardial cushion defect). Since the valve frame or rigid ring will push into the LV outflow tract to obstruct it. In the region of the coronary sinus, the ring sutures were placed very close to the annulus or almost into the leaflet to prevent conduction bundle damage. Because of a deformed annulus, a soft ring was preferred. Hemodynamically significant MR with a need for reoperation occurs in 4% to 15% of patients after repair of AV canal (septal) defects, and it is the primary cause for reoperation. Kanani et al. 8 showed that in children, the primary cause of early re-repair (<1 year) is because of leaflet tears or dysplasia, while late re-repair has multiple areas of valvar leakage, including central incompetence, as seen in our case also. Moore et al. 9 found that there are increased chances of successful re-repair in certain congenital anomalies (e.g., partially opened anterior mitral cleft after previous AV canal reconstruction) if the leaflet size is preserved.
Conclusion
MV repair surgeries via redo sternotomy required later in life are fairly challenging in these kinds of dysmorphic valves, but can be done with better results than replacement.
Footnotes
Acknowledgements
We would like to acknowledge the contribution of our perfusion team, perioperative nursing team, and support staff for the successful outcome of this surgery.
Ethical considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent to participate
Written informed consent was obtained from the patient before surgery.
Consent for publication
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Author contributions
All the authors were part of the surgery and contributed equally to this manuscript’s preparation.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data are taken from patient records.