
Abstract
Papillary muscle rupture is a life-threatening complication of acute myocardial infarction that most commonly occurs 2–7 days after the infarct. We present a rare case of acute partial anterolateral papillary muscle rupture following non-ST elevation myocardial infarction. Our patient was an elderly male who had a detached anterolateral papillary muscle, which required emergent mitral valve replacement. Papillary muscle rupture is a rare complication of acute myocardial infarction, and anterolateral muscle rupture occurs even less commonly. When papillary muscle rupture is diagnosed, patients need to be emergently referred to cardiothoracic surgery as mortality without surgery is over 90% within a week.
Keywords
Introduction
Papillary muscle rupture (PMR) with acute mitral regurgitation (MR) is a life-threatening complication of acute myocardial infarction (MI) that most commonly occurs 2–7 days after the infarct. Rupture of the posteromedial papillary muscle (supplied by the right coronary artery or dominant left circumflex) is much more common than anterolateral papillary muscle (with dual blood supply from the left anterior descending artery and left circumflex arteries) and can occur in both ST elevation and non-ST elevation MI (NSTEMI). 1 Mechanical complications of acute MI, such as PMR, can be preceded by an ischemic event days prior to the onset of the PMR. Here, we present a rare case of partial anterolateral PMR following acute NSTEMI.
Case presentation
A 66-year-old male with a history of coronary artery disease (CAD) and quadruple coronary artery bypass graft (CABG) surgery presented to MountainView Hospital on 19 March 2022 with an 8 h history of substernal chest pain without shortness of breath. Initial vital signs were blood pressure of 120/70 mmHg, pulse 76 beats/min, and pulse oximetry of 98% on room air. Physical examination was unremarkable. Electrocardiogram showed sinus rhythm with ST depressions in leads V3–V5 (Figure 1). Chest X-ray did not show any acute cardiopulmonary process (Figure 2). Laboratory studies revealed elevated NT pro-BNP 18,999 pg/mL (reference 5–125 pg/mL), high sensitivity troponin were 12,441 ng/L and 15,265 ng/L (reference 0–22 ng/L), and elevated D-dimer 0.83 mg/L (reference <0.50 mg/L). Initial hemoglobin and platelet count were found to be within normal limits at 13.9 g/dL (reference 14.0–18.0 g/dL) and 280,000/µL (reference 150,000–450,000/µL), respectively. Urinalysis demonstrated large amounts of blood. Aspirin and empiric heparin infusion for NSTEMI were initiated.
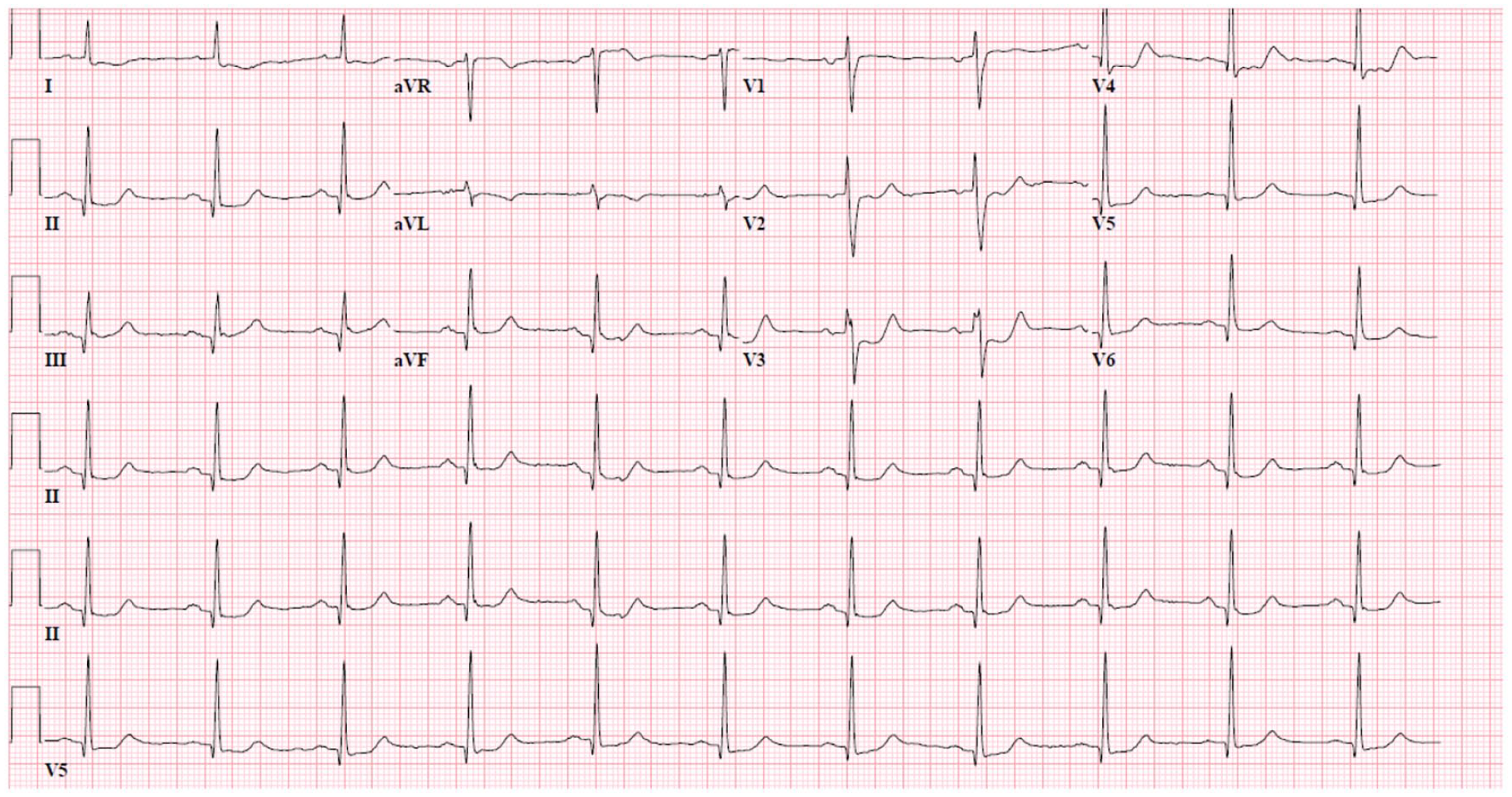
EKG on admission showing ST depressions in leads V3–V5.

Prominent cardiac silhouette status post median sternotomy.
At 12 h following admission, the patient developed sudden onset of emesis, diaphoresis, and worsening chest pain radiating to the back and neck. He became hypotensive with a blood pressure of 80/60 mmHg and tachycardic with a heart rate of 125 beats/min. He was resuscitated with intravenous fluid and taken emergently to the cardiac catheterization lab. Coronary angiogram revealed severe native multivessel CAD with patent left internal mammary artery to left anterior descending, vein graft to obtuse marginal and vein graft to right coronary artery. Thrombotic occlusion of the vein graft to diagonal was thought to be the culprit lesion with 80% occlusion (Figure 3(a)). After ballooning failed to restore flow, aspiration thrombectomy of the vein graft was performed followed by placement of a drug eluting stent. There was improvement of flow and TIMI-3 flow was restored (Figure 3(b)). His left ventricular end-diastolic pressure was 20 mmHg. Given the patient’s persistent hypotension and ongoing chest pain, an intra-aortic balloon pump (IABP) was placed with improvement of hemodynamic parameters. Post procedure, he was transferred to the intensive care unit and placed on dual antiplatelet therapy, as well as amiodarone infusion for wide complex tachycardia.

(a) Coronary angiography showed 80% occlusion of the vein graft to diagonal. (b) Restoration of flow demonstrated after placement of DES.
Transthoracic echocardiogram (TTE) revealed left ventricular ejection fraction (LVEF) 55% with evidence of left atrial enlargement and partially detached papillary muscle (Figure 4(a) and (b)). There was mild annular calcification and systolic bowing of the anterior mitral leaflet resulting in severe MR. Chest computed tomography demonstrated trace bilateral pleural effusions. Repeat TTE showed LVEF 50%–55%, moderate flail motion of the anterior mitral leaflet and evidence for rupture of the anterolateral papillary muscle head. At this time, cardiothoracic surgery was consulted for acute PMR. Three days after stopping ticagrelor, the patient underwent bioprosthetic mitral valve replacement and removal of IABP. Preoperative transesophageal echocardiogram (TEE) confirmed the PMR and postoperative TEE demonstrated no evidence of residual MR or decreased LVEF (Figure 5). Direct inspection of surgical specimen revealed 95% ruptured anteromedial papillary muscle, without leaflet vegetations or perforations. Microscopic pathologic evaluation showed mitral valve with degenerative changes with myocyte necrosis and chronic inflammation.
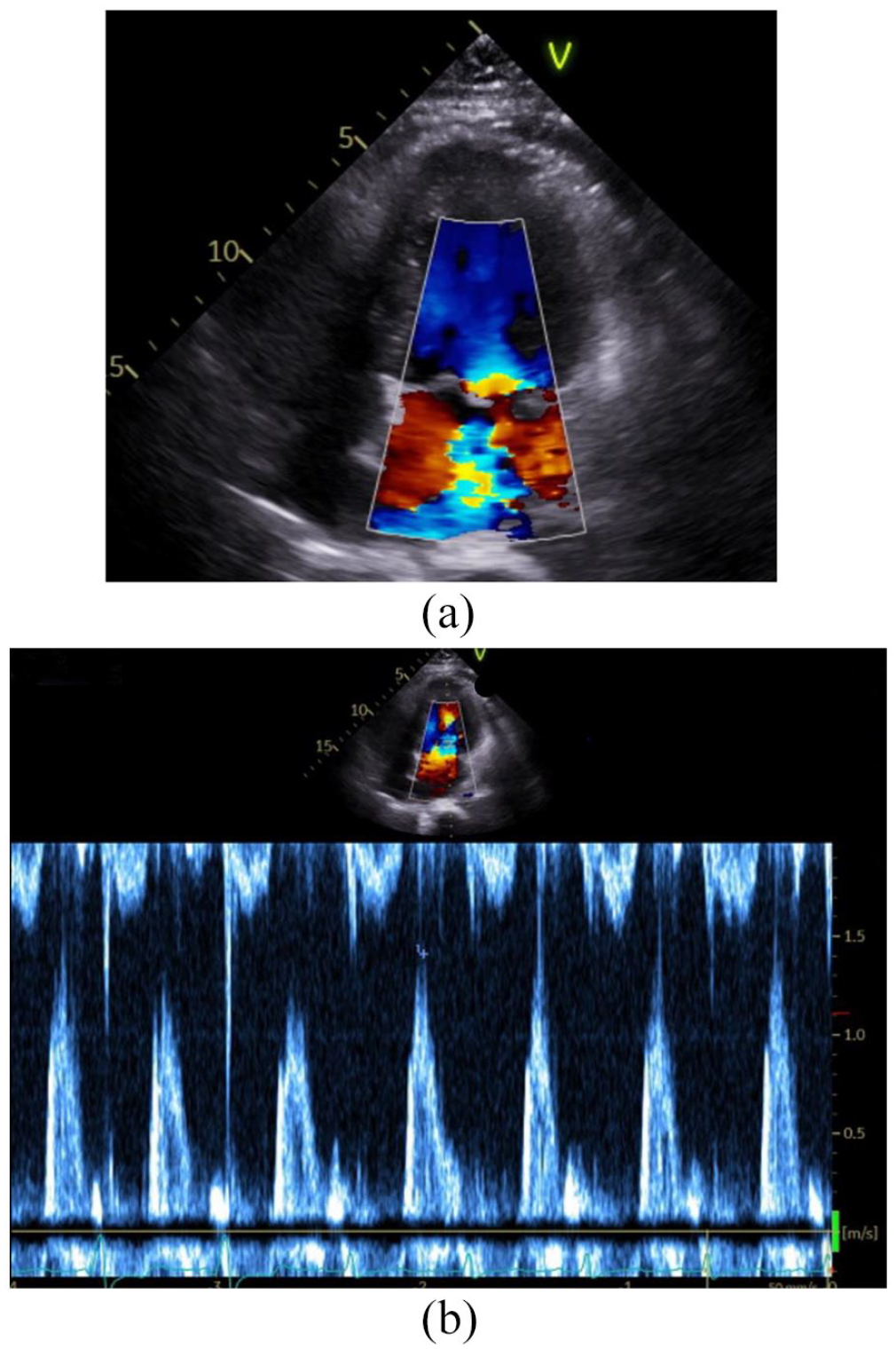
(a) Color Doppler demonstrating severity of mitral regurgitation with (b) ECG tracing of cardiac cycle.

TEE demonstrates the partially detached anterolateral papillary muscle head.
He was continued on dual antiplatelet therapy and beta-blocker upon discharge. A month following hospital discharge, the patient was asymptomatic and the TTE performed showed a normal LVEF and a functional bioprosthetic mitral valve without valvular or paravalvular leaks.
Discussion
PMR has occurred in roughly 1% of reported cases following an acute NSTEMI. 2 Mechanical complications of MI in patients who present with cardiogenic shock or pulmonary edema are rarely attributed to PMR due to its scarcity (0.5%–5%). 3 About half of reported cases of PMR have a small infarction, with preserved ejection fraction, which leads to increased shearing stress at the site of rupture.4,5 The most common cause of acute PMR is an infarction upstream to the coronary artery supplying the papillary muscle. Given the single blood supply (posterior descending artery) to the posteromedial papillary muscle, it is more frequently ruptured compared with the anterolateral papillary muscle, which has a dual blood supply from the left anterior descending and left circumflex arteries. 6 Given the pathological findings, ongoing ischemia was evident days prior to his presentation. As coagulative necrosis progressed in the myocardium supplied by the diagonal artery from his vein graft, the anterolateral papillary muscle was partially detached due to stress.
PMR on TTE is likely to reveal a ruptured head prolapsing into the left atrium and a hyperdynamic left ventricular function. 7 Our patient did not have significant multiorgan failure despite waiting for 2–3 additional days for surgery. Support with IABP provided LV decompression resulting in augmentation of diastolic and coronary perfusion. 8 Considering he was in cardiogenic shock due to acute MR, IABP improved the hemodynamic profile by increasing mean arterial pressure and cardiac output. In addition, IABP counterpulsation reduced afterload and wall stress which led to a fall in myocardial oxygen consumption, a goal of treatment of patients with myocardial ischemia. 9 The limited degree of regurgitation allowed pressures within the left atrium and pulmonary circulation to accommodate and hemodynamics improve with support. 10 This allowed further medical optimization in our patient, including discontinuing his antiplatelet therapy.
We postulate several mechanisms to the partial detachment of anterolateral papillary muscles as opposed to its complete rupture: (1) early diagnosis, (2) dual blood supply, and (3) lower ventricular wall stress provided by insertion of IABP. The rupture of the anterolateral muscle is less common, occurring in 25% of cases, as it has dual blood supplies. Partial PMR is commonly seen in small area infarctions, often with mild-to-moderate coronary disease. 11 Early identification and preserved ventricular function via IABP resulted in a lower shear force on the ischemic papillary muscle, thus rupture occurred at one of the muscle heads. Although our patient did well with IABP and surgery, the same cannot be said for all cases. Some patients will present with Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS) Profile 1 and very severe multiorgan failure. These patients will need more advanced forms of mechanical circulatory support (i.e. Impella, ECMO, ECPELLA) to survive until the surgery and sustain the postoperative period.
Short-term prognosis of cardiogenic shock is directly related to the severity of the hemodynamic disorder. There is limited evidence on the long-term outcomes of patients with cardiogenic shock treated by contemporary practice. The IABP-SHOCK II trial reported IABP having no effect on all-cause mortality at 6-year long-term follow-up. Mortality remains high, with two-thirds of patients with cardiogenic shock dying despite treatment with revascularization therapy. 12
Conclusion
NSTEMI in the case of total occlusion can cause significant structural damage to the heart, such as acute partial PMR. It is paramount for clinicians to have a high index of suspicion in patients presenting in cardiogenic shock following acute MI.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported (in whole or in part) by HCA Healthcare and/or an HCA Healthcare affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.