
Abstract
Medicolegal autopsies should be performed for sudden, unexpected, and suspicious deaths. Such autopsies should be performed by a knowledgeable Forensic Pathologist who has experience in performing traditional autopsy techniques, as well as having an understanding of how to supplement these techniques with more scientifically advanced techniques such as magnetic resonance imaging and postmortem computed tomography. In this case, we utilized the traditional Ghon technique to remove the urogenital system, combined with postmortem computed tomography of the coronary arteries and contrast imaging of the ureters. By combining a traditional autopsy technique with more advanced imaging techniques, we were able to definitively establish the cause of death as coronary artery occlusion and, by doing so, remove any suspicion of medical negligence committed by the treating physicians during ureteroscopic bilateral stone removal.
Keywords
Introduction
In sudden, suspicious, or unusual deaths, a thorough medicolegal autopsy should be performed to unequivocally establish the cause and manner of death. 1 To accomplish this, it can be very helpful to combine supplementary advanced imaging technologies, such as postmortem computed tomography angiography (PMCTA) and contrast imaging, with traditional autopsy techniques.2,3 The traditional autopsy techniques typically used in postmortem examinations are the Virchow, Rokitansky, Letulle, and the Ghon techniques. The Virchow technique employs organ removal one by one; the Rokitansky technique utilizes in-situ dissection of organs; the Letulle technique uses the removal of the cervical, thoracic, and abdominal organs in a single organ block (en masse); in the Ghon technique, the cervical and thoracic organs, organs of the abdomen, and the urogenital system undergo removal as separate organ blocks (en bloc). The imaging techniques commonly used in Forensic Medicine include X-ray imaging, computed tomography (CT), and magnetic resonance imaging (MRI). X-rays detect fractures, location of bullets, shrapnel, fragments of explosives, and help examine skeletal remains to determine age, sex, and height of the deceased, as well as confirming identity. They often serve as a precursor to advanced imaging techniques such as CT scans and MRI. There are few things to remember when deciding whether to use CT or MRI imaging in that both have strengths and weaknesses. CT scans offer superior resolution for identifying fractures, hemorrhages, and coronary calcification. When combined with angiography, they enhance the accuracy of detecting vascular pathologies. Additionally, CT is more widely accessible, cost-effective, and faster compared to MRI. However, postmortem CT (PMCT) has two definitive weaknesses. The first is it has relatively low soft-tissue contrast, especially in the parenchyma of the organs. The second is it has poor ability to view the vascular system. 4 The latter weakness is significant in that in the developed countries, cardiovascular disease is a major cause of unexpected natural death. 5 The limitations in visualizing the vascular system reduce the effectiveness of PMCT in diagnosing cardiovascular disease. MRI has demonstrated significant utility in pediatric pathology due to its superior ability to provide detailed images of soft tissues compared to CT. Additionally, MRI is more effective in detecting acute myocardial infarctions than CT. However, MRI is limited in its capacity to identify arterial occlusions. The errors commonly associated with CT and MRI imaging in determining a cause of death are ischemic heart disease, pulmonary embolism, pneumonia, and intra-abdominal lesions such as intestinal infarction. 6
To further show the advantages of PMCTA, in cases of natural death, only about half of the essential bone lesions (53.8%) and two-thirds of the essential soft tissue lesions (64.0%) were detected at autopsy, whereas PMCTA helped to detect 84.6% and 90.0%, respectively. In cases of violent death, more than half of the essential vascular findings were missed at autopsy (60.9%). Using PMCT without angiography, 87.8% of essential vascular findings were missed, whereas <1% were missed using PMCTA. However, slightly <30.6% and 63.4% of essential vascular lesions were detected at PMCT and autopsy, respectively. In one study, PMCTA was superior to autopsy for all findings except essential soft-tissue findings. 6
The best approach to performing a thorough postmortem examination is to combine traditional autopsy techniques with more advanced scientific techniques such as newer imagining technologies.7,8 In this autopsy, the Ghon technique was used, in which the urogenital system (kidney–ureter–bladder (KUB)) was removed en bloc combined with PMCTA of the coronary arteries and contrast imaging of the bilateral ureters along with histopathological findings to ensure accuracy as to cause and manner of death. In cases of suspected medical error, which this case was one of, 93.3% of essential vascular lesions were detected at PMCTA. This more involved approach to this autopsy was done in light of the accusation by the family of the deceased, that his death was due to medical negligence during ureteroscopic bilateral stone removal.
Case report
A 65-year-old male who passed away was transported to our mortuary for postmortem examination. The police and family members of the deceased reported that he had undergone a ureteroscopic bilateral stone removal procedure and placement of a double J (DJ) stent 2 days prior. Twenty-four hours after surgery, the patient was in a mobile state and conscious, cooperative, and oriented to time and place. On the second day after surgery, the patient went to the bathroom and fell to the floor when he was coming out. He was immediately resuscitated and transferred to the intensive care unit (ICU), where despite receiving appropriate care, he died shortly thereafter. On learning about his death, the family members of the deceased believed that the clinicians involved in his care were negligent and, thus, responsible for his death. Interestingly, the deceased had no notable medical history, which would have suggested that he was at risk of sudden unexpected death. During an external examination of the body, two iatrogenically induced needle puncture sites were noted on the right forearm. No other notable injuries were noted. Radiographic images of the pelvis and KUB performed during the postmortem examination revealed stents in the ureter (Figure 1). The skull cavity was opened, followed by the chest, abdomen, pelvis, and lastly, the neck. Upon opening of the skull, the brain was edematous and congested. The entire brain was fixed in 10% formalin for neuropathological analysis. Upon opening of the chest cavity, both lungs displayed congestion and edema. Tissue samples were collected from all five lobes. After removing the pericardial sac, the heart was extracted, along with the descending aorta. Before dissecting the heart and taking tissue samples, we performed PMCTA to identify pathological conditions. By carefully dissecting the ascending aorta, we identified the anterior and posterior coronary ostia at the root level of the ascending aorta. The right coronary artery originated from the anterior ostia, whereas the left coronary artery originated from the posterior ostia. A 17-gauge intravenous catheter was inserted into each ostium and loosely secured using ligature. Two syringes containing a mixture of 9 mL gastrografin (Mallinkrodt, Inc., St. Louis, MO, USA) and 1 mL dye (Stat Lab Medical Products, Inc., Lewisville, TX, USA) were attached to the catheters. Approximately 3–5 mL of the mixture was infused into both catheters until a slight resistance was encountered, after which the catheters were removed, and the vessels were ligated (Figure 2). The heart was placed in a box made of low-density polyethylene–polypropylene and exposed to a 120 kv mAs auto Field of View (FOV) 30 cm, 0.625 slice thickness GE optima CT660 having kernel standard for PMCTA. After completion, the intact heart was preserved for histopathological examination (HPE). Upon opening the abdomen, we ligated the antral and cardiac ends of the stomach and removed them from the abdominal cavity. No abnormalities were detected in the interior of the stomach. To visualize and completely remove the KUB apparatus, the duodenum was initially secured, and the small and large intestines were carefully dissected from the kidneys and rectum down to the proximal level of the distal portion of the abdominal aorta, ureters, bladder, and renal arteries while preserving their continuity. The entire masses of the ureters, bladder, and kidneys were removed from the remaining organs (Figure 3). Both ends of the ureteric-bladder junctions were ligated, and an intravenous catheter was introduced at the level of the renal hilum and extended toward the root of the ureter. Both the ureters were ligated at the level of the renal hilum. Two syringes filled with a mixture of 9 mL gastrografin and 1 mL dye were connected to the catheters. Approximately, 7–8 mL of the mixture was injected into both catheters until slight resistance was encountered. Subsequently, radiographic images of the KUB were obtained using a portable X-ray device of Fujifilm CR, Tokyo, Japan system manufactured in Japan. After imaging processes were finished, the bladder and ureters were carefully dissected. Upon visual inspection, no injuries were detected, and the stents were fully intact. No notable observations were made for the neck.
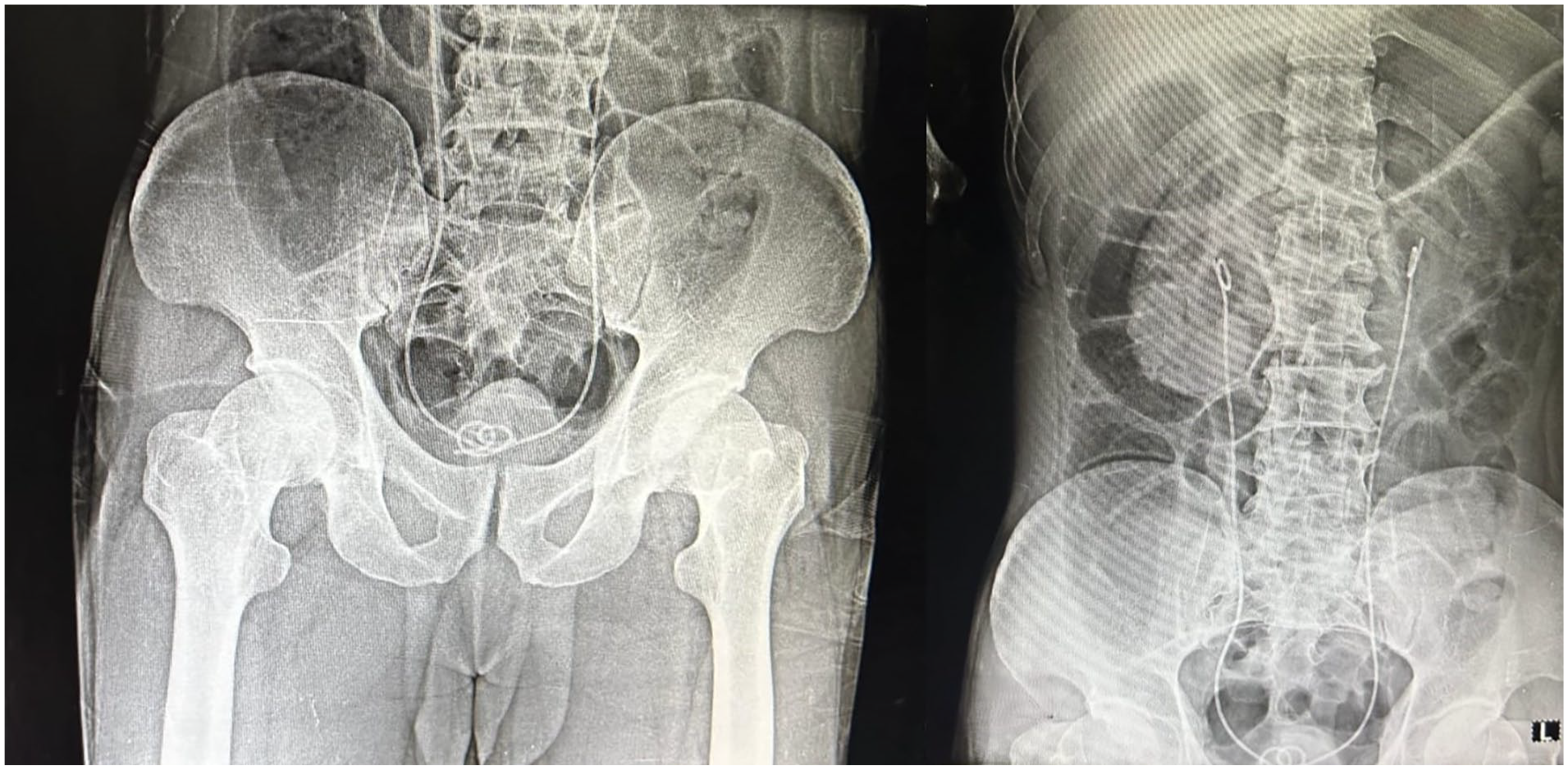
X-ray image of KUB before contrast injection.

Steps for introducing contrast in coronaries.

Separation of KUB from other organs.
PMCTA findings: There was no opacification of the contrast beyond Segment II, suggesting a complete thrombotic occlusion (Figure 4).
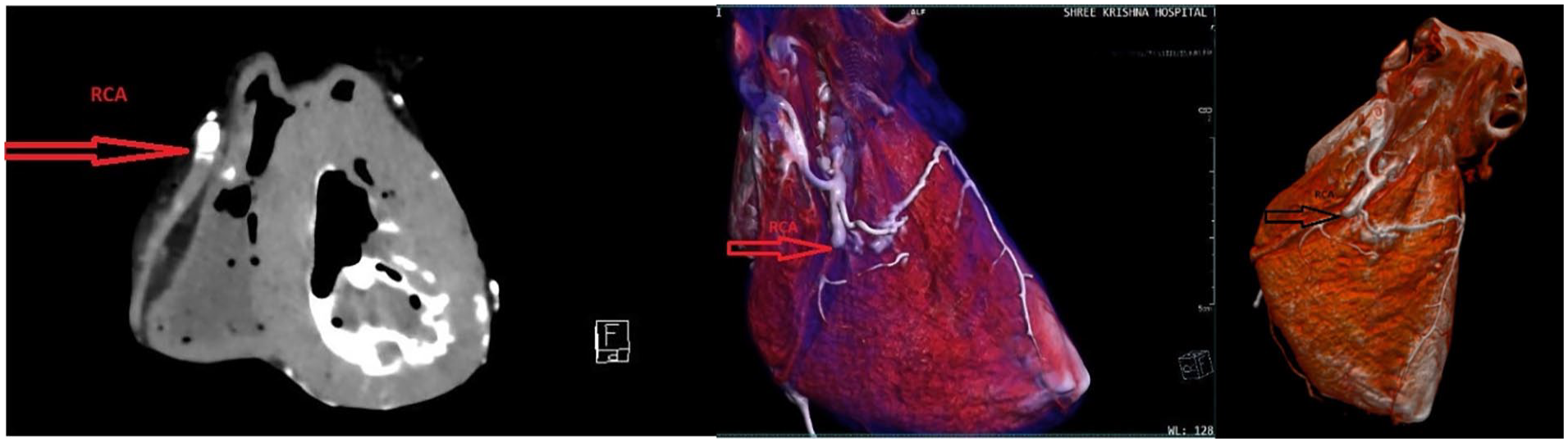
PMCTA image of the right coronary artery showing occlusion.
Contrast X-ray imaging of KUB findings: The contrast was uniformly opacified in both ureters by using an in-situ DJ stent (Figure 5).

X-ray image of the ureters after contrast injection.
Histopathological findings: The left coronary and left circumflex arteries showed Grade IV atherosclerosis, and the right coronary artery showed Grade V atherosclerosis (Figure 6). Histopathological findings revealed an antemortem thrombus in the lumen of the right coronary artery (Figure 7). The walls of the right atrium, right ventricles, and posterior part of the interventricular septum showed muscle fiber waviness, disarray, and degenerated myocytes with interstitial edema (Figure 8). No other significant findings were evident in other viscera.
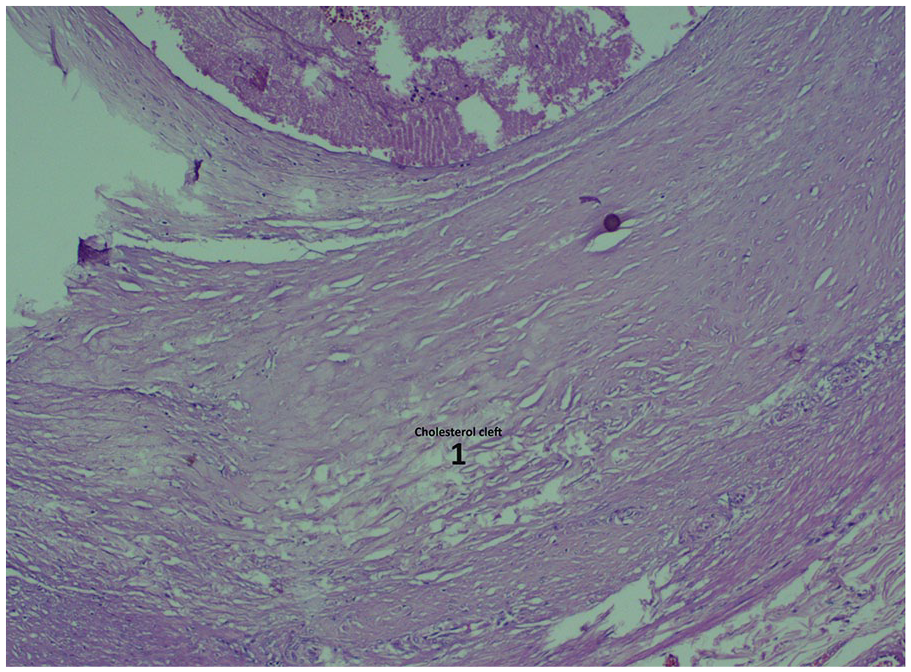
Grade V atherosclerosis of the right coronary artery.

Thrombus in the right coronary artery.

Histopathological findings from the wall of the right ventricle.
Cause of death: Acute ischemic heart disease as a result of right coronary artery occlusion in a patient with coronary artery disease.
Overall, CT proved to be a more accurate imaging technique than MRI for determining the cause of death. Both CT and MRI have limitations in diagnosing vascular lesions; however, in this case, we combined PMCT with contrast imaging of the coronary arteries and contrast X-ray of KUB.
Discussion
A physician should keep learning by utilizing recent medical scientific advances, provide relevant information to patients, peers, and the public, seek appropriate advice, and collaborate with other healthcare professionals, especially in the performance of autopsies. 9 An effective and unified method, such as modified and innovative techniques for performing postmortem assessments, is necessary to guarantee impartiality and strict compliance with evidence-based medicine. 10 Modern postmortem techniques involve more than just tissue dissection and microscopic examinations. Pathologists have a wide range of ancillary techniques and procedures that can be used to diagnose the cause of death, including postmortem chemistry, immunohistochemistry, PMCT, PMCTA, and MRI. 11 Selected procedures and recent techniques can supplement traditional autopsy techniques, demonstrating disease processes or injuries more effectively. 7 Using a contrast agent in the coronary arteries can reveal subtle signs of cardiac disease in cases of sudden death. Contrast agents are also helpful in forensic settings where extensive dissection may cause artifacts. 8 In the current instance of sudden death, we performed a PMCTA on the coronaries, which revealed the presence of a suspected thrombus in the right coronary artery. The intact heart was sent for HPE to prevent the potential dislodgement of the suspected thrombus. HPE confirmed an antemortem thrombus in the right coronary artery, with grade V atherosclerosis and changes in acute myocardial ischemia. In this case, 48 h before death, the deceased underwent ureteroscopic stone removal and bilateral DJ stent placement. DJ stents are widely used in urological procedures, including endoscopic and open surgery, for retroperitoneal tumors, fibrosis, ureteral strictures, and reno-ureteral stone treatment. 12 Some of the typical complications associated with ureteral stone removal through DJ stenting include the risk of stent malpositioning, obstruction, lumbar pain, urinary tract infection, stent fragmentation, and damage to the ureter. 13 To rule out any injuries, the KUB must be examined during the postmortem examination. As described by Otto Saphir, the sigmoid colon was cut through a double ligature at its mid-portion, and the kidneys along with the distal portion of the abdominal aorta, ureters, bladder, prostate, rectum, and distal part of the sigmoid were removed en masse from the remaining organs. 13 Brenda L. Waters discussed a method for surgically excising the KUB and rectum while simultaneously cannulating the ureter for urography. 14 As discussed by Otto Saphir and Brenda L Waters, we refined this method by omitting the sigmoid colon and rectum. Radiography of the ureters with and without contrast showed that the intact stent was properly placed without injury or perforation.14,15 It is noteworthy that while routine intraoperative cystoscopy greatly enhances the identification of urinary tract injuries during surgery, it seems to have little impact on the detection rates of such injuries after the operation. This indicates that some injuries might not be immediately visible, even with thorough examination during the procedure. 15 In forensic investigations, examining the urinary tract after death is vital for ascertaining the cause of death and detecting any surgical complications. For example, a study involving surgical ICU patients who succumbed to sepsis or septic shock found that postmortem examinations identified kidney or urinary tract pathologies in 60% of the cases, with 6% of patients having pyelonephritis as a persistent septic source. 16 These findings highlight the importance of thorough postmortem ureteric analysis in understanding the progression of disease and potential complications in critically ill patients.
CT’s poor ability to view the vascular system can be augmented by combining it with angiography using intravenous contrast agents. Probably the most widespread single approach for postmortem angiography is the multiphase PMCTA,11,12 first described in 2011. 9 This technique uses a specific perfusion device and an oil-based contrast agent of specific viscosity. It is recommended when considering the use of PMCT with or without angiography that the postmortem examination be performed in a stepwise manner, beginning with an in-depth review of the circumstances of death followed by a thorough external examination of the body. The next step should be to perform PMCT, which may be sufficient to confirm a suspected cause and manner of death. The PMCT results will help determine whether PMCTA and targeted histologic analysis is necessary to ascertain a definitive cause and manner of death. In this case, the use of PMCTA proved conclusively no medical error was committed. Postmortem angiography was used extensively in the development of the “virtual autopsy” (VA) now referred to as “Virtopsy.” The concept of the VA was developed at the University of Bern’s Institute of Forensic Medicine in Switzerland with the work of Dr. Richard Dirnohofer and Dr. Michael Thali, in the late 1990s. Despite the evolution of imaging studies and the development of the “Virtopsy,” at this time, the traditional autopsy techniques remain the standard of practice. 10
In this case, our findings enabled us to eliminate intraoperative mistakes and thus absolve the treating clinicians from being accused of medical negligence. Also, this approach addresses a significant obstacle in PMCT by providing detailed information about coronary arteries, which has been a limitation in considering whether PMCT could replace conventional invasive autopsies. 17
Conclusion
Supplementing traditional autopsy techniques with advanced postmortem radiological imaging can provide helpful information that more accurately determines the cause of death and thus absolves the accused of wrongdoing, whether that be criminal or civil. By combining the Ghon technique with PMCTA of the coronary arteries and contrast imaging of the ureters, we were able to prove conclusively to the family that the death of their loved one was not due to medical negligence during the ureteroscopic removal.
A high-quality postmortem examination is important not only in forensic cases but also for the evaluation of the quality of clinical diagnosis and therapy in clinical pathologic analysis. It is thus an important instrument for both justice and medical quality control, which is what this case was all about. The use of PMCT and PMCTA might be feasible ways to increase the number of high-quality postmortem examinations.
Footnotes
Ethical considerations
Approval from the ethics committee has been secured for publishing these cases (IEC/BU/2024/Cr.65/354/2024 dated October 15, 2024; Institute Ethical Committee Registration – DHR Reg No – EC/NEW/INST/2021/592).
Consent to participate
Written informed consent was taken from the legal guardian of the deceased.
Consent for publication
Written informed consent was obtained from a legally authorized representative for anonymized patient information to be published in this article.
Author contributions
Arijit Datta was very keen and focused on conceptualizing ideas in the case report design, interpreting the data, and reviewing the manuscript. Darshan Galoria contributed to drafting and reviewing manuscript portions. Shridhar Dave was instrumental in interpreting radiological data and reviewing the manuscript. William A. Cox contributed to the drafting and manuscript review. Prashant Verma contributed to reviewing the manuscript and interpreting the postmortem data. Srushti Shukla was instrumental in data collection, drafting, and reviewing the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.