
Abstract
Cardiac tamponade is a medical condition that occurs when there is an accumulation of blood, pus, fluid, or gas in the area around the heart (i.e. the pericardial cavity), leading to increased pressure within the pericardium. In forensic practice, sudden natural deaths are mostly related to cardiovascular conditions including cardiac tamponade. Owing to the sudden and rapid nature of its progression and fatal outcome, CT is often diagnosed during postmortem examination. In this case report, we discuss the sudden death of a 54-year-old male deceased due to a sudden collapse. No external or internal injuries were observed. On internal examination, in the mediastinum, a “Blue dome” sign of the heart was present; 600 g of liquid and clotted blood were present in the pericardial cavity. The etiology was not ventricular free wall rupture; rather, it was coronary artery rupture, which is a rare cause of such tamponade. Postmortem histopathology revealed significant atherosclerotic changes in the coronary arteries, leading to atherosclerotic plaque rupture. This etiology was first reported in this case, causing fatal cardiac tamponade.
Keywords
Introduction
Cardiac tamponade (CT) is a medical condition characterized by the accumulation of blood, pus, fluids, or gas in the area surrounding the heart, resulting in increased pressure within the pericardium. The rising pericardial pressure surpasses the central venous pressure, limiting venous blood flow to the heart. This condition is nearly always lethal and can result in abrupt fatality unless pressure is reduced through either immediate surgical intervention or needle pericardiocentesis.1,2 Various factors such as trauma, infection, or certain medical conditions such as cancer, an old infarct, or acute myocardial infarction leading to ventricular free wall rupture can cause cardiac tamponade. The symptoms of CT typically include sudden collapse, shortness of breath, chest pain, a sudden fall in blood pressure, and a rapid heartbeat. Early diagnosis and prompt treatment are crucial to prevent further complications and improve survival.3,4 In forensic practice, it is frequently encountered in cases of sudden and unexpected deaths caused by cardiovascular factors. Previous literature has revealed that CT is a contributing factor to sudden cardiac mortality, with a prevalence ranging from 25% to 30% in cases of significant pericardial effusions.5,6 Compared to pericardial fluid accumulation, which gradually increases in volume (500–2000 mL) over a short duration of time, the rapidity of accumulation (200–300 mL per min) is often the deciding factor for fatality due to CT. This is because the latter allows a greater volume of fluid to accumulate within the pericardial sac owing to gradual distension. CT can be caused by a variety of factors, including active or passive pericardial effusion, hemopericardium (HP) resulting from trauma, iatrogenic intervention, the rupture of an acute myocardial infarction (RAMI), or a separating ascending aortic aneurysm within the pericardium. 7 HP usually follows the rupture of acute myocardial infarction, the rupture of dissecting aortic aneurysm, or trauma.8,9 It has also been linked to malignancy, 9 chemotherapy, 10 homicide, 11 injury during the insertion of pacing wires or angioplasty or central venous catheters,12,13 endocardial biopsy, 14 open heart surgery, 15 interventional coronary artery procedures, 16 exercise stress tests, 17 electroconvulsive therapy, 18 coronary artery vasculitis, 19 dissecting aneurysm, 20 myocardial abscess, 21 infective endocarditis, 9 and rarely during amniocentesis 22 or the prenatal period. 23 Owing to the sudden and swift manner in which it presents itself, as well as its potentially lethal outcome, CT is often suspected, and diagnosis is made during postmortem examination. In this report, we discuss a case of cardiac tamponade due to massive hemopericardium caused by spontaneous rupture of a coronary artery, leading to sudden collapse and death.
Case report
A 54-year-old man was found unconscious in the bathroom of his home. He was brought to a tertiary healthcare facility and was declared dead. Furthermore, the deceased individual was shifted to a mortuary to conduct a postmortem examination. No history of diabetes, hypertension, or chronic disease was noted. Written informed consent was obtained from a legally authorized representative for anonymized patient information to be published in this article.
Autopsy findings
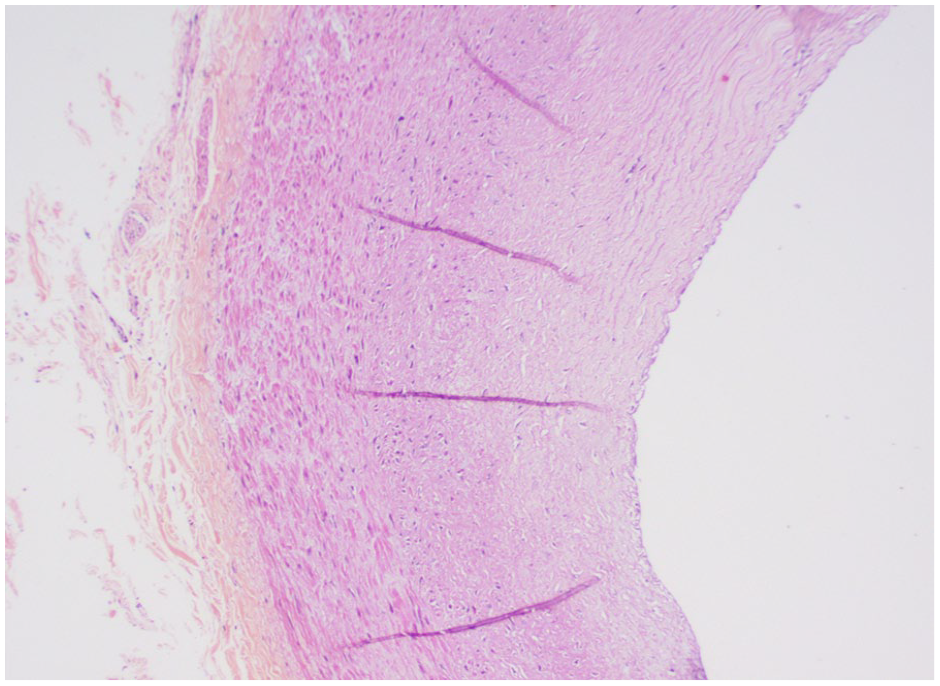
External examination revealed no visible bodily injuries, except for notable bluish facial and nailbed discoloration. Upon the opening of the thoracic cavity, the presence of the “Blue dome” sign of the heart and an elongated pericardial sac raised the suspicion of possible cardiac tamponade (Figure 1). The pericardium was elevated from both sides of the base using forceps and a nick was created on the anterior surface of the pericardium. Curved blunt head scissors were used to create an incision in the shape of an inverted “Y” on the anterior side of the pericardium to expose the epicardial surface of the heart. Upon opening the pericardial cavity, 600 g of clotted and partially liquid blood was to cover almost the whole heart’s outer surface. The weight of the heart was 454 g. During the examination of the heart, an area of epicardium measuring 0.5 cm × 0.5 cm at the left border of the heart overlying the area on the course of the left coronary artery was found to be ruptured (Figure 2). Further dissection was performed to determine the source of the hemorrhage. All the coronary arteries were narrowed and sclerosed. Right, left, left anterior descending, left circumflex, and diagonal branches of left coronaries were meticulously dissected. The diagonal branch of the left coronary artery over the left border of the heart. A rupture area was observed at the level of the corresponding area (Figure 3). Tissues from different parts of the heart around the diagonal branch of the left coronary artery were sent for histopathological examination. Histopathological examination revealed a diagonal branch of the left coronary artery with Grade V atherosclerosis (Figure 4) and Grade IV atherosclerosis over the arch of the aorta, the right coronary artery left circumflex artery (Figure 5), and the left coronary artery (Figure 6) showed Grade IV atherosclerosis. The cross-section of the coronary artery showed large atheromatous plaque having central necrotic lipid-laden cores and with foci of blotchy calcification. Tunica media is partly thinned out and tunica adventitial shows a sprinkling of chronic inflammatory cells (H&E 4×) (Figure 4). No elastic staining was performed. H/E stain was done.

Blue dome sign of heart and elongated pericardial sac.

Ruptured left border of the heart.

Ruptured diagonal branch of the left coronary artery.

Grade 5 atherosclerosis in the diagonal branch of the left coronary artery.
Grade 4 atherosclerosis in the left circumflex coronary artery.

Grade 4 atherosclerosis in the left coronary artery.
Figure 5 also shows histological features of part of an artery with an atheromatous plaque, along with the presence of cholesterol clefts in the intimal layer. The adventitial layer shows a sprinkling of inflammatory cells (H&E 10×). In this case, the cause of death was cardiac tamponade due to the rupture of a diagonal branch of the left coronary artery.
Discussion
The pericardium consists mainly of dense fibrous tissue that protects the heart. The pericardial cavity contains approximately 50 mL of fluid that cushions the cardiac activity. The accumulation of fluid within the pericardial cavity can have life-threatening consequences that hamper cardiac movements. Although the cavity can generally accommodate gradual fluid buildup, sudden accumulation of a larger amount of fluid (e.g., 200–300 mL or more) can result in fatal complications. This is because the fluid compresses the heart, preventing proper movement and impairing the ventricular filling and cardiac output. Increased pressure also restricts coronary blood flow to the myocardium, which, in turn, can damage the heart muscles. Furthermore, high intrapericardial pressure inhibits venous return to the heart, leading to the rapid accumulation of fluid in the pericardial cavity. If left untreated, this fluid volume can significantly reduce the systemic venous-right atrial pressure gradient, which is essential for adequate cardiac filling. As a result, heart output becomes insufficient to maintain the coronary artery and systemic perfusion, leading to cardiovascular collapse. 24 Myocardial rupture, most commonly due to ventricular free-wall rupture, can also cause massive hemopericardium with fatal outcomes. 8 A common risk factor is hypertension in a female aged > 60 years. In the present case, no evidence was present.
This case illustrates sudden death due to spontaneous rupture of the atherosclerotic plaque of the diagonal branch of the left coronary artery associated with the rupture of the left ventricular epicardial wall to open in the pericardial cavity, providing a free potential space for the escape of blood to accumulate. This etiology is not only rare but also the first reported in any medical literature. The patient was a male with no prior history of hypertension. However, upon examination of the histopathological findings, significant alterations were observed in the diagonal branches of the left coronary artery, aorta, right coronary artery, left coronary artery, and left circumflex artery. Several studies have discussed various nontraumatic factors associated with the development of hemopericardium and subsequent cardiac tamponade.8–10,17–21 Kashiwase et al. reported a case in which cardiac tamponade developed due to the rupture of a diagonal branch of the left coronary artery because of elective percutaneous coronary intervention which is traumatic in nature. 25 Several studies have also reported that cardiac tamponade due to rupture of the coronary artery occurred because of angioplasty complications.16,26–28 In this case, rupture of the diagonal branch of the left coronary artery occurred due to the advanced stage of atherosclerosis developed “Blue Dome” sign of heart.
Conclusion
In forensic medicine, our case underscores the importance of recognizing cardiac tamponade as a potential cause of sudden death. Rupture of the diagonal branch of the left coronary artery, attributed to advanced atherosclerosis, highlights the significance of thorough postmortem examinations in determining the etiology, leading to the diagnosis of the exact cause of death. This emphasizes the necessity of forensic experts to consider cardiovascular factors, such as atherosclerosis, when investigating sudden and unexpected deaths, ultimately contributing to more accurate determinations of the cause and manner of death.