
Abstract
Objectives:
Continuous and interval training have previously been compared in patients with cardiac diseases. However, data comparing the safety and effectiveness of the two exercise methods are lacking in patients early after coronary artery bypass grafting.
Methods:
In all, 120 patients were prospectively randomized in a 1:1 fashion approximately 17 days after coronary artery bypass grafting to an interval group or continuous group. All patients participated in bicycle ergometric training six times/week for 20 min each during a 3-week inpatient rehabilitation program. The combined primary endpoint was safety as defined by incidence of scar pain and cardiac events related to the exercise intervention. Secondary outcomes included the effect of the interventions on parameters such as heart rate and peak power output.
Results:
Four patients (12.1%) in the interval group reported pain on the saphenectomy scar as a result of the training intervention in comparison to six patients (20.0%) in the continuous group (χ2 (1, n = 63) = 0.73, p = 0.393). No cardiac events were related to exercise intervention. No effect on heart rate was found during the intervention, nor was a difference observed between the groups. Peak power output, as one of the analyzed markers, improved significantly in both groups, but no differences were found between groups.
Conclusion:
Ergometry training performed as interval or continuous training was safe and effective regarding increase in physical fitness early after coronary artery bypass grafting in an inpatient rehabilitation setting, with no differences observed between the groups.
Keywords
Introduction
In the secondary prevention of coronary heart disease (CHD), physical activity has shown positive effects on morbidity and mortality. In particular, an increase in cardiorespiratory fitness, which represents a main part of cardiac rehabilitation programs, appears to be associated with a decrease in mortality. 1
Electrocardiogram (ECG)-supported bicycle ergometric training constitutes a compulsory therapeutic tool in the cardiac rehabilitation of CHD. As this form of therapy offers the possibility to set and monitor the determined training heart rate and exercise intensity via a previously completed exercise ECG, such an intervention is a comparatively safe means of developing aerobic endurance. 2
Basically, two training methods are distinguished: among them, continuous method usually applies the target pulse approach. Here, the exercise heart rate is determined during an exercise ECG. Once this has been achieved, the computer-controlled training program regulates the pedaling force such that the patient’s training heart rate is not exceeded.
The second type is the interval method. In the exercise sciences, interval training is a methodology in use for elevating exercise intensity above what is possible with continuous training. The aim is to increase the exercise stimulus.3–5 With this approach, two different levels of pedaling force alternate in a fixed time window. The interval method has increasingly been used in the treatment of patients with chronic diseases. Meanwhile, the effectiveness of the interval method has also been well proven in patients with CHD and is considered safe in cardiac rehabilitation.3–6
After coronary artery bypass grafting (CABG), rehabilitation presents special challenges. In these patients, exercise tolerance is low at the beginning of the cardiac rehabilitation process in comparison to their preoperative physical condition. 7 Pain as a result of sternotomy and saphenectomy represents, in addition to the psychological effects, a typical complication with which a patient and the staff of the rehabilitation facility are confronted. 7 Furthermore, postoperative risks such as wound-healing disorders, graft occlusions, myocardial ischemia, or arrhythmias must be considered. Especially in the first eight postoperative weeks, these complications must be taken into consideration when performing muscular training exercises, and stretching and shearing movements of the thorax must be avoided. 6
For patients after CABG, the potential of interval training has not yet been sufficiently established. Indeed, the recommendations for rehabilitation of these patients are mostly derived from the guidelines for patients with other manifestations of CHD, 8 and most studies did not address immediate follow-up after acute cardiovascular treatment and did not consider the potential risks after CABG. Additionally, it is not known how continuous or interval aerobic training affects scar pain early in the wound-healing process. The purpose of the present study was to investigate whether the interval method represents a safe or even superior form of training compared to the continuous training method in patients early after CABG.
Methods
A total of 120 patients were randomized in a 1:1 fashion to the interval or continuous training group after CABG in this prospective, randomized, single-center, cohort study. A randomization list was created, with the randomization algorithm assigning the patient IDs to the two treatment groups. Randomization was carried out by the study team using previously sealed, opaque, and consecutively numbered envelopes after registering, informing, and receiving consent of the patients to participate in the study at the center.
Patients at the Paracelsus-Harz Clinic, Quedlinburg, Germany, aged ⩾ 18 years were included in the study early (less than 3 weeks) after CABG after giving written informed consent. The study was approved by the Ethics Committee of the Medical Association of Saxony-Anhalt.
The primary outcome was safety, which included the incidence of scar pain, cardiac arrhythmia, symptomatic blood pressure fluctuations, or syncope/presyncope related to the exercise intervention. The extent of exercise-related pain in the wound-healing areas was determined by Faces Pain Scale–Revised (FPS-R).9,10
Secondary outcomes of this study were heart rate, peak power output, peak power output in relation to body weight, and maximum performance in relation to age and gender as a percentage of target performance in the comparison of exercise ECG at the start of the study period and second exercise ECG after the last training session.
The cardiac and performance-related measurement parameters were recorded with two ERG 911 BP loading ergometers (Schiller®). To record the cardiac measurement parameters, the 12-lead ECG and spiroergometry device AT-10 plus was used. The bicycle ergometric training was carried out in a facility with eight ergoselect 200 devices from ergoline®. Training control software ERS1 was used for training control and to record the training data.
The maximum pedaling power was a result of the first exercise ECG, which was performed according to the World Health Organization (WHO) recommendations, starting with 25 W and increasing stepwise by 25 W each 2 min. The result after reaching the maximum of 100 W for 2 min as suggested for patients after CABG formed the basis for calculating the initial exercise intensity in both exercise groups. During interval training, 80% of the maximum pedaling power was completed in the exercise phase, as determined in the initial exercise ECG. For the exercise phase in endurance training, 50% of the maximum pedaling power was set. The active recovery phase of the interval group was performed at 30% of the maximum pedaling power.
During the first training session, training loads were determined in both groups based on training heart rate and subjective perception of exertion. Exercise heart rate was defined as a heart rate reserve (HRR) at 70%. The following formula was applied: HRR = HR at rest + 0.7 × (HRmax − HR rest). The subjective perception of exertion was rated from 6 to 20 using the classic rated perceived exertion (RPE) scale. 11 The aim was to achieve a scale value of 15. The underlying rationale for using both control parameters for intensity control was the notion that, in this way, a sufficient stimulus could be achieved.12,13
The exercise frequency we selected corresponds to the tolerance range of three to seven exercise units per week, according to the recommendations for endurance training in patients with CHD.1,6 Each session consisted of a total of 20 min, of which 3 min corresponded to the warm-up phase, 16 min to the main load phase, and 1 min to the cool-down phase. In the main load phase of the interval training, 16 intervals were completed, in which the loading phase comprised a duration of 20 s and the recovery phase a duration of 40 s. The chosen duration and the resulting ratio between the two interval phases of 1:2 correspond to the guideline on physical activity in secondary prevention and therapy of cardiovascular diseases established by Bjarnason-Wehrens and her working group. 6
Statistical analysis
The sample size was determined on the basis of a preliminary examination during which the effect on heart rate at a defined exercise level was examined as part of a 3-week bicycle ergometric training in patients after CABG.
Assuming a test strength of 0.80 and a two-sided significance level of 0.05, a case number of n = 49 per group was calculated. Taking into account a dropout rate of 20%, the overall sample size for this study was n = 120.
Depending on the scaling type and the prerequisites for statistical analysis methods, parametric and nonparametric tests were used to compare samples. For nominally scaled variables, the chi-square independence test was used. After considering the underlying assumptions, variance analysis methods were applied for metric variables, using the general linear model (GLM) with repeated measures or without repeated measures. In order to calculate time and interaction effects, we employed the GLM with repeated measures.
To estimate and compare the effect sizes, the effect sizes (Cohen’s d) and the partial eta squared
Results
After CABG, 120 patients were randomized in equal proportions to the interval group and continuous group. The interval group consisted of 54 men and 6 women (mean age: 60.5 ± 9.4 years) and the continuous group consisted of 50 men and 10 women (mean age: 61.9 ± 9.0 years). No differences between gender distribution and age were found between the two groups, χ2 (1, n = 120) = 1.15, p = 0.283 and F (1, 119) < 1, p = 0.388,
Furthermore, body mass index (BMI; 29.1 ± 5.8 kg/m2 I-group vs 29.0 ± 4.1 kg/m2 continuous group, F (1, 119) < 1, p = 0.920,
The interval between surgery and admission to rehabilitation was 17.0 ± 6.9 days for the interval group and 17.8 ± 12.4 days for the continuous group (F (1.119) < 1, p = 0.668,
Moreover, all other baseline parameters were comparable in the two groups (Table 1).
Baseline parameters.
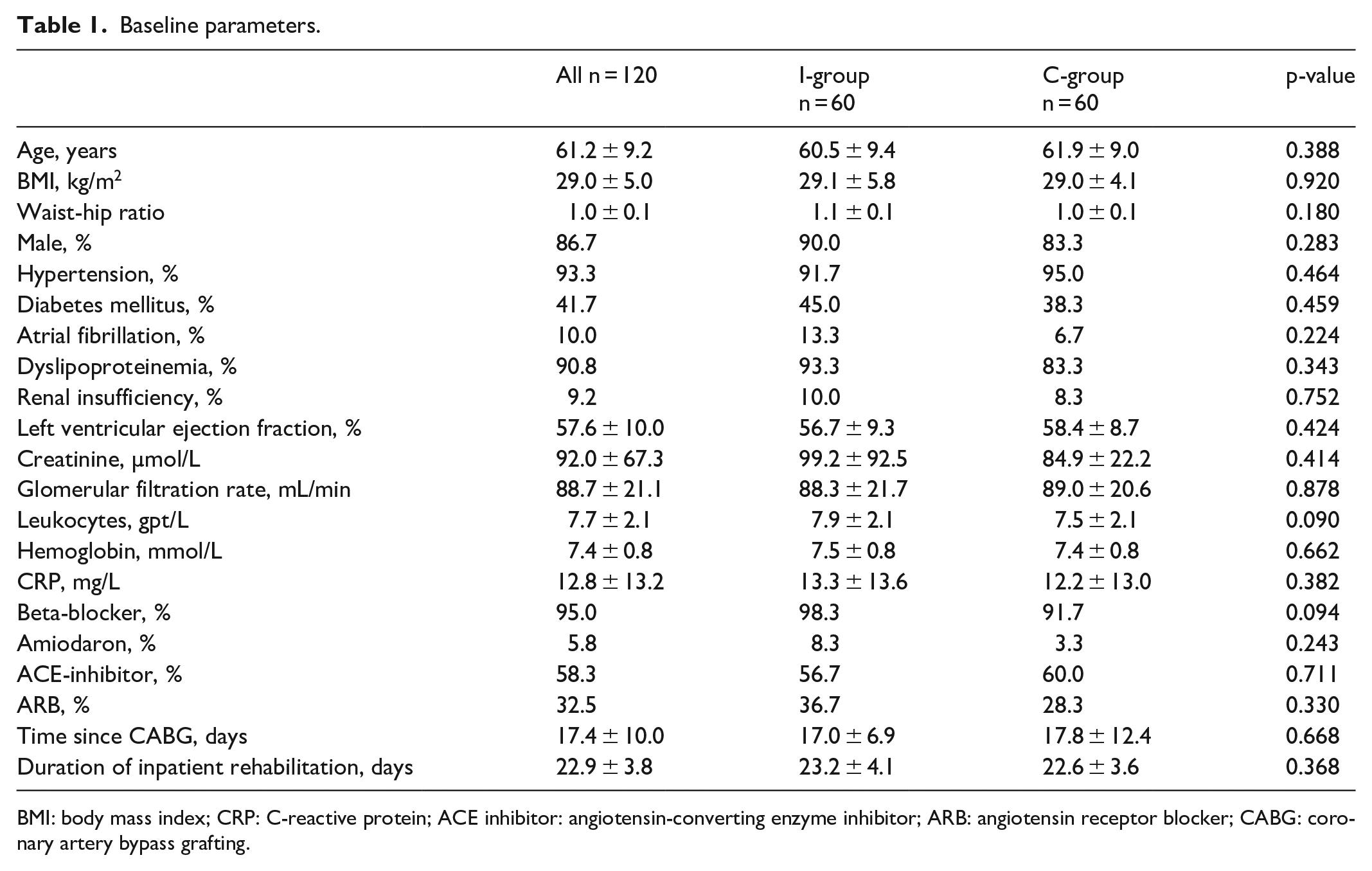
BMI: body mass index; CRP: C-reactive protein; ACE inhibitor: angiotensin-converting enzyme inhibitor; ARB: angiotensin receptor blocker; CABG: coronary artery bypass grafting.
Dropouts
Among the total number of 29 dropouts, 16 patients were from the interval group and 13 patients from the continuous group (χ2 (1, n = 120) = 1.41, p = 0.522).
Patients excluded from data analysis were those in whom a second exercise ECG was not conducted and/or had less than 180 min of training intervention throughout the course of rehabilitation, for example. In two patients, an evaluation was not possible due to data loss.
Safety
All patients had received a sternotomy. In 33 patients (75.0%) of the interval group and 30 patients (63.8%) of the continuous group, saphenectomies had been performed.
Of the interval group, a total of four patients (12.1%) reported pain on the saphenectomy scar as a result of the training intervention. In the continuous group, a total of six patients reported pain (20.0%) (χ2 (1, n = 63) = 0.73, p = 0.393). In one patient in the interval group (2.3%) and six patients in the continuous group (12.8%), a radial artery graft was used. None of the patients reported exercise-related pain in the scar area of the lower arm (Figure 1).

Frequency (numbers of patients reporting) of exercise-induced pain intensity: (a) Sternotomy and (b) Saphenectomy.
None of the patients had to interrupt or stop a training session due to scar pain and none of the patients experienced cardiac arrhythmia, symptomatic blood pressure fluctuations, or syncope/presyncope related to the exercise intervention.
Training results
The results of the training sessions showed that, taking into account the total intervention time, the number of training minutes in the interval group at 265 ± 62 min did not differ from that of the continuous group at 287 ± 72 min (z = −0.81, p = 0.417) (Figure 2(a)).

(a) Mean training duration during the 3-week rehabilitation period and (b) mean physical work during the 3-week rehabilitation period.
No effect on mean heart rate during training sessions was found during the intervention (F (2.130) = 1.58, p = 0.209,

Development of mean heart rate during training sessions (a) and mean physical work (b) in the two groups during the 3-week inpatient rehabilitation. The main phase included 16 min of exercise during each training session in which the calculated exercise frequency was reached.
With regard to the physical work performed during the study period, comparable results were found (see Figure 2(b)). At 707 ± 284 KJ, the mean physical work of the interval group did not differ from that of the continuous group with 771 ± 330 KJ (F (1.90) < 1, p = 0.325) (Figure 2(b)).
The 3-week rehabilitation program showed a statistically significant effect with respect to mean improvement in physical work in both groups (F (2.132) = 86.84, p < 0.001,
The peak power output (maximum pedaling power) in the interval group increased from 86.6 ± 16.6 to 112.2 ± 27.5 W, with an effect size of d = 1.13, and in the continuous group from 83.9 ± 17.0 to 108.4 ± 21.5 W, with an effect size of d = 1.36 during 3-week inpatient rehabilitation in both groups (F (1.88) = 153.58, p < 0.001,

Peak power output depend on time and groups.
The peak power output in relation to body weight increased in the interval group from 0.98 ± 0.19 W/kg to 1.27 ± 0.31 W/kg, with an effect size of d = 1.13. For the continuous group, an increase from 1.00 ± 0.19 W/kg to 1.32 ± 0.24 W/kg was observed (d = 1.39). This increase was significant in both groups (F (1.89) = 138.25, p < 0.001,
Discussion
In the present study, two bicycle ergometric methods—13–14 sessions of interval or continuous training performed for 20 min each—were compared during a 3-week inpatient rehabilitation period in 120 patients early after CABG surgery, with the aim of comparing the two methods with regard to their safety and effectiveness.
Safety
Although patients began rehabilitation treatment soon after surgery, both the interval method and the continuous training method performed for 13–14 moderate exercise sessions over 20 min each during the 3 weeks of inpatient rehabilitation can be considered safe according to our study.
The primary aim of this study was to examine the occurrence of pain in surgical scars caused by the exercise stress and cardiovascular complications during ergometry training. The main result was that, irrespective of the training method, patients experienced pain after individual training sessions both in the wound area of the sternotomy and in the saphenectomy scars. Although the patients reported scar pain, it did not affect their decision to continue the training intervention (data not presented), which is in line with the results of another recent study. 14
Furthermore, no cardiac arrhythmias, symptomatic blood pressure changes, or syncope/presyncope attributable to the training intervention were found in either group. This positive result underpins the data on the cardiovascular safety of interval and continuous training in comparative methodological studies involving patients with CHD.
Previous studies with comparable designs have shown the same results.5,12,15–17 However, the present study is the only investigation that has compared interval and continuous training in patients early (mean 17.4 days) after CABG although a very recent study showed in patients early after CABG that “conventional physical therapy combined with peripheral muscle strength training and respiratory muscle strength training may reduce inspiratory muscle strength loss and improve pain and vitality perception in the immediate postoperative period after CABG.” 18
Efficiency
Ergometry training in addition to other therapeutic interventions during a 3-week inpatient rehabilitation increases physical ability in patients early after CABG. Efficiency, as the result of functional adaptations of the heart during endurance training, lowers cardiac stress at identical workloads. The present study showed an approximately 30% increase in maximum efficiency and an approximately 30% increase in maximum performance in relation to body weight in both groups, which is consistent with the results of other studies.5,19–24
However, as the main secondary outcome, differences in heart rate adaptations during exercise were not found during the 3-week inpatient rehabilitation in either group.
Comparison of interval training versus continuous training
We expected higher exercise intensity in the interval group than in the continuous group after training for 3 weeks according to the results of other groups.20,21 However, interval training was not superior to continuous training in patients early after CABG regarding improvement in physical performance in this study. Existing meta-analyses of studies comparing interval and continuous training in patients with CHD showed that study parameters and designs diverge greatly. Thus, the interpretation and comparability of these studies are limited.25–29 However, looking at comparable studies in detail, four studies did not find the interval method to be superior in terms of increasing maximal endurance capacity5,19,22,23 whereas three studies found interval training to be superior to continuous training.20,21,24
This raises the question of how to interpret the results of the current study in the light of previous studies. In addition to comparing the training methods, it might be informative to examine the intensity differences between the exercise and recovery phases of interval training. Neither great differences21–23 nor small differences in intensity16,17,30,31 between the phases showed that interval training, in terms of maximum power improvement, was clearly superior to the continuous method. Thus, intensity cannot be the only parameter affecting the assessment of the interval method in some studies.
In comparable studies, the study designs vary greatly since the majority of the protocol features differ considerably from each other. In addition, these studies were much smaller (18 and 45 patients) and the duration of exercise longer (approximately 750 min in both studies), which might best explain the differing results.16,21
Limitations
The single-center study design, which may involve local characteristics, limits the generalizability of the results. Furthermore, the higher participation rate of men than women represent a limitation, although gender-specific differences with regard to training-associated pain and training discontinuations could not be determined (data not presented).
Other important limitations are as follows: first, the difference between calculating sample size by heart rate and the primary endpoint and, second, according to a relatively low event rate in the literature the study was underpowered with regard to drawing conclusions on the impact of moderate exercise training on safety.
Conclusion
Pulse-controlled ergometry training performed as interval or continuous training during inpatient rehabilitation was safe according to reports of pain with equal training intensities and effective regarding an increase in physical fitness early after CABG in patients with CHD, but no differences between the methods were found.
Footnotes
Author contributions
All authors contributed significantly to the submitted work.
Availability of data and materials
The dataset analyzed during the current study is available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Ethics Committee of the Medical Association of Saxony-Anhalt (63/12).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written consent was obtained from all patients before inclusion in the study.