
Abstract
Background:
Muscle atrophy and prolonged inactivity are associated with an increased sensation of fatigue and reduced functional capacity in the postoperative period in patients undergoing coronary artery bypass grafting. Cardiac rehabilitation after hospital discharge is highly recommended and contributes to improvement in functional capacity and quality of life. However, few studies have evaluated the effectiveness of early mobilization protocols during hospitalization on the patterns of physical activity and functional capacity after coronary artery bypass grafting.
Objective:
To investigate the effectiveness of an early mobilization program on the functional capacity of patients undergoing coronary artery bypass grafting in the short and long term.
Methods:
This is a prospective, randomized, controlled, single-blind trial protocol that will evaluate 66 consecutive patients undergoing coronary artery bypass grafting. Patients will be randomized into two training groups: the control group (N = 33), which will perform breathing exercises and the intervention group (N = 33), which will perform breathing exercises and aerobic exercises. The groups will receive treatment from first to the seventh postoperative day, twice daily. In the preoperative period, the following outcomes will be assessed: physical activity level (Baecke Questionnaire), Functional Independence Measure, and functional capacity (6-min walking test). Functional capacity will be reassessed after the 7th and 60th postoperative day. Pulmonary complications and length of hospital stay will also be evaluated. Statistical analysis will be calculated using linear mixed models and will be based on intention-to-treat. The level of significance will be set at α = 5%.
Background
Cardiac surgery is a well-established procedure worldwide with excellent results for efficacy and safety in treating heart patients. Among the different types of treatments, coronary artery bypass grafting (CABG) is considered an effective alternative for the treatment of ischemic heart disease. The indication for myocardial revascularization, especially in acute coronary syndromes (ACS), has as main objectives to improve ventricular function, reduce symptoms of myocardial ischemia, prevent progression to acute myocardial infarction (AMI), and reduce mortality.1–3
However, the combination of the complexity of the procedure and the use of cardiopulmonary bypass (CB) has had a very positive association with the incidence of complications in the postoperative period. 4 The CB produces a systemic inflammatory response through the release of substances that impair immune response and that are widely known to increase capillary permeability and its deleterious effects, 5 the main ones being atelectasis, pleural effusion, and pneumonia complications such as respiratory 6 acute kidney injury7,8 neuromuscular disorders, low cardiac output syndrome, postoperative bleeding, infection, and difficulty in glycemic control. 7
Systemic complications in the postoperative period increases the duration of mechanical ventilation and sedation 9 and promotes muscle weakness, 7 leading to a longer period in the intensive care unit (ICU) and a reduction in mobility.10,11 The deleterious effects of immobility include decreased protein synthesis, increased proteolysis, and loss of muscle mass and strength, compromising functional capacity and ability to perform activities of daily living.10,12–15 It is known that the likely consequences generated by immobility can last for months and even years after an ICU length of stay,16–19 preventing patients from fully returning to baseline functional ability 15 and increasing the risk of hospital readmission.20,21
The role of physical therapy in the ICU has been recently highlighted, as well as its importance in the practice of early mobilization22–26 and exercise protocols for surgical patients.27–30 It is feasible and safe to carry out a physical exercise protocol in the short term. 22 Physical therapy is also associated with decreased respiratory complications following cardiac surgery, 31 reduced loss of muscle strength, 32 decreased morbidity and mortality, 33 improved cognitive conditions, 34 and an increase in the number of days free of mechanical ventilation. 26
Despite reports of improvement in physical capacity due to early mobilization in patients after cardiac surgery, there is a lack of standardization regarding the intensity, type, frequency, and duration of exercise. 35 More studies are needed that concentrate on the importance of standardized protocols since the repercussions of these procedures can influence the patients for a long period after hospital discharge.36,37
Thus, this study aims first to assess the effectiveness of early mobilization on the functional capacity of patients undergoing CABG and subsequently evaluate the possible influence on the length of the hospital stay and the development of postoperative pulmonary complications (PPC), emphasizing the importance of identifying the need for specific protocols for continued rehabilitation and new physical therapy strategies. Our hypothesis is that patients undergoing the early mobilization program will have improved 6-min walking test (6MWT) results (walked distance) at discharge on the 60th postoperative day compared to the patients who only carry out the breathing exercise program.
Methods
Study design
This study will be a randomized, controlled, single-blind trial. The study protocol was registered at Clinical Trials (NCT02312648) and approved by the local Ethics Committee (protocol number 34569214.5.0000.0064). This trial started recruiting patients on 2 February 2015, and data collection is likely to finish by February 2016. After signing the informed consent form, the patients will undergo a baseline assessment. Following surgery, patients extubated within 24 h will be randomly assigned into one of two groups: a control group (CG) or an intervention group (IG). At discharge, the groups will be assessed regarding functional capacity, PPC, and length of hospital stay. Functional capacity will be reevaluated 60 days after randomization (Figure 1).

Study design.
The randomization scheme will be generated by a computer and carried out by an investigator who is not involved in the recruitment and treatment of patients. The allocation of the patients will be concealed using sequentially numbered, sealed, and opaque envelopes. On the first day of treatment after surgery, the envelope allocated to the patient will be opened by the physical therapist who provided the treatments. The patients will be informed that they will receive one of two different physical therapy approaches.
Participants, therapists, center
This study protocol will include consecutive patients admitted for elective and conventional CABG in a tertiary hospital according to the following criteria: both genders, age between 18 and 80 years, body mass index (BMI) between 20 and 30 kg/m2, hemodynamic stability with or without use of positive inotropic drugs, absence of arrhythmias and angina, mean blood pressure (MBP) 60 ⩽ MBP ⩽ 100 mmHg, heart rate (HR) 60 ⩽ HR ⩽ 100 bpm without respiratory distress such as nasal flaring, the use of accessory muscles, thoracoabdominal asynchrony, and a respiratory rate (RR) ⩽ 20 without signs of infection.
The exclusion criteria are as follows: previous pulmonary disease and acute lung disease, mechanical ventilation >24 h, left ventricular ejection fraction (LVEF) <35% or >54%,36,37 surgical reintervention, intraoperative death or any contraindications for the proposed measurements and/or treatment, contraindications for the 6MWT or any proposed protocol, orthopedic impairments, unstable angina, HR >120 bpm at rest, and systolic blood pressure >180 mmHg or diastolic >100 mmHg.
All patients will be evaluated by the same investigator at three different times: preoperative period (first assessment), 7 days after the beginning of the protocol (second assessment), and 60 days after hospital discharge (third assessment). The first assessment will be performed up to 2 days before the operative procedure in the following sequence: demographic (age, weight, height, and BMI) and clinical data (ejection fraction, medications, and comorbidities) will be collected from medical records, lung function test (spirometry), physical activity level (Baecke Questionnaire), Functional Independence Measure (FIM), and functional capacity test (6MWT).
After the postoperative procedure, a randomization program will randomly assign patients extubated within 24 h into two groups: the CG, which will perform breathing exercises or an IG, which will perform breathing exercises and early mobilization. Both will receive preoperative orientation about the surgical procedure, the importance of early ambulation, and cough stimulation. Standardized physical therapy will be provided from the first to the seventh postoperative day. The sessions will take place twice a day with an average time of 30 min each.
After 30 days, the assessor will contact the patients by telephone to collect the following information: the presence of symptoms that suggest any cardiac abnormality, the need for hospitalization, and performing any physical activity. The second and third assessments will only measure functional capacity (6MWT) and will be performed by blinded assessors at hospital discharge and 60 days after discharge.
Intervention/control
A total of 52 patients will be randomly allocated to one of two groups: CG, which will perform a supervised respiratory exercise program (usual care), and IG, which will receive the same respiratory exercise program combined with an early mobilization program (Table 1). Following the standardized hospital protocol, all participants will perform exercises with bi-level positive airway pressure41,42 (BIPAP® Synchrony) with orofacial interfaces from 30 to 60 min immediately after tracheal extubation according to the needs of each patient.
Early mobilization protocol (days).
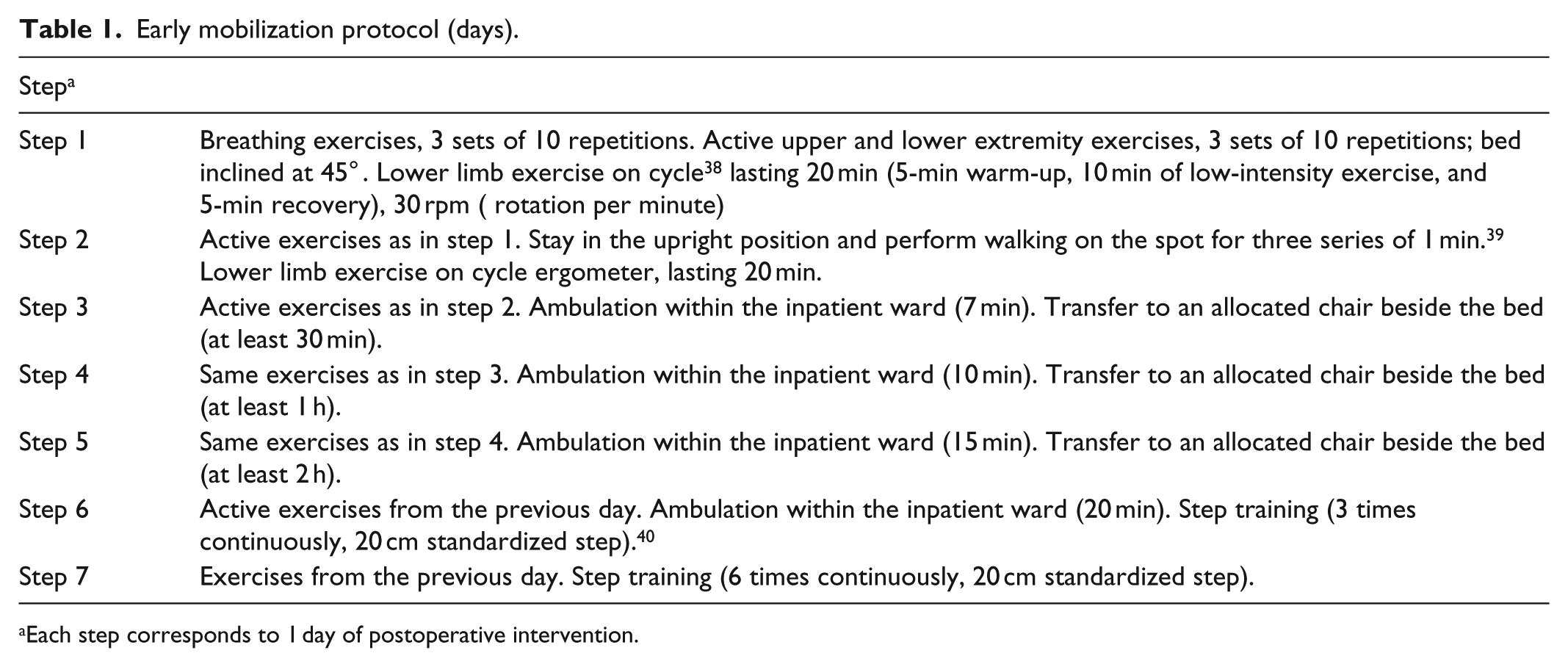
Each step corresponds to 1 day of postoperative intervention.
The predetermined parameters will be as follows: adequate inspiratory pressure to maintain an optimal tidal volume within 6 to 8 mL/kg and expiratory pressure of 6 cmH2O 41 plus supplemental oxygen to maintain oxygen saturation above 95%. The exercises will be supervised by a physical therapist in both groups. Before performing the exercises, the patients will be asked to quantify their pain and, if they describe an intensity of more than three on the visual analog scale (VAS), a prescription of analgesics (containing moderate opioids) will be requested from their physician and a break will be taken at that moment until the sensation of pain gets better. Medication use as well as the pain (VAS) will be quantified (drug, dose, and frequency) for comparison between groups.
Early mobilization program
This program will be conducted only in the IG as described below (Table 1) and with respective images in Table 2.
Intervention group protocol.

Outcomes measures
The primary outcome will be functional capacity (6MWT), which will be measured preoperatively, at discharge after 7 days of the protocol, and after 60 postoperative days. The secondary variables will be the incidence of PPC and the length of the hospital stay.
Procedures
Pulmonary function
The patients will perform spirometry according to the American Thoracic Society and European Respiratory Society guidelines. 43 The variables considered will be the forced expiratory volume in the first second (FEV1) and the forced expiratory volume/forced vital capacity (FEV/FVC) ratio in absolute values and as a percentage of the predicted values according to the prediction equations described for the Brazilian population. 44
Physical activity level
The Baecke Habitual Physical Activity Questionnaire consists of 16 questions concerning three components from the past 12 months: occupational activities score (8 questions), physical exercise during leisure activities score (4 questions), and leisure and locomotion physical activities score (4 questions).45,46 The patients will be considered sedentary when the score is <9, active when the score is between 9 and 16, and athletic when the score is >16. 45
FIM
The FIM is an instrument that assesses the disability level of patients with functional restrictions of different origins. Its primary objective is to quantitatively evaluate the level of assistance required for a person to perform a series of motor and cognitive tasks needed for daily living. The evaluated activities include self-care, mobility, walking, toileting, communication, and cognition, including memory, social interaction, and problem solving. 47 Each of these activities is assessed and receives a score of 1 (total dependence) to 7 (complete independence), thus the total score ranges from 18 to 126.47,48
Borg perception test
The perceived level of respiratory discomfort during physical effort will be evaluated by the modified Borg scale, ranging from 0 (least effort) to 10 (most effort). The patient will be instructed regarding the use of the scale and prompted for the spontaneous choice of a value. 49
Primary outcome
Functional capacity
The 6MWT will be performed according to the recommendations of the American Thoracic Society. 50 The patients will be instructed to walk the greatest distance at the highest speed possible for a period of 6 min. The walking course must be 30 m in length. An assessor will provide standardized encouragement every minute. The patient will be allowed to rest during the test if required and this time will be included in the total time of the test. The test will be performed twice with a 1-h interval between tests. The best distance will be recorded. Normal predicted values of the 6MWT distance (p6MWD) will be calculated using the equations proposed by Britto et al. 51 The minimum clinically significant difference considered will be 25 m. 52
Secondary outcomes
PPC
PPC will be diagnosed by the clinician if one or more of the following criteria are present: (1) pneumonia 53 —presence of radiological evidence of pulmonary infiltration associated with at least two signs, including purulent sputum, elevated body temperature (>38.0°C) or leukocytosis (⩾25% above baseline preoperative value); (2) tracheobronchitis—marked increase in sputum production or presence of purulent sputum in a patient with a normal chest X-ray; (3) atelectasis with clinical repercussions 54 —radiological evidence of lung atelectasis associated with dyspnea; (4) hypoxemia under SpO2 <85% and a need for oxygen; 55 (5) Acute respiratory failure—acute deficiency of gas exchange with need for invasive or noninvasive mechanical ventilation.
Length of the hospital stay and mortality will be evaluated. Postoperative analgesia will be managed by the medical staff, and the VAS will be used before each treatment session to evaluate the need for medication.
Data analysis
Sample size calculation will be based on the main outcome (functional capacity, walked distance in the 6MWT), considering a previous study with 93 patients that aimed to determine whether a physiotherapy-supervised walking program might improve walking capacity of patients undergoing CABG surgery, 41 and estimating a minimal difference between groups of 25 m with a standard deviation of 32 m, with a power of 80% and an alpha of 5%. The result will be a sample size of 33 participants per group. The data will be double entered, and the intention-to-treat analysis will be performed. The effects of the intervention on patient functionality will be calculated using a linear mixed model, which will incorporate the terms for the treatment, time, and treatment by time interactions. The level of significance will be set at α = 5%. The data will be analyzed using the Statistical Package for Social Sciences (SPSS) 21.
Expected results
It is expected that, after the performance of the mobilization protocol, started earlier, the patients in the IG will have an improvement in the distance walked in the 6MWT, which will be assessed during 7 postoperative days and 60 days after hospital discharge, and will have less time in ICU and lower prevalence of pulmonary complications, when compared to the CG. It is also expected that with the results obtained from this study, it will be possible to introduce an early mobilization protocol in the ICU routinely unit and sensitize the medical board about the importance of proper physiotherapy conduct.
Potential study limitations
As the protocol has already been registered, we cannot change or add any variables, for example, the level of pain and the adherence of the patients to the therapy after discharge. We will need to control the variables to avoid possible future bias.
The physical therapists from the hospital team will be trained to do the same evaluations with all patients, but it is clear to us (the authors) that because there are a large number of physical therapists inside the hospital, this could be also a bias. Each intervention will be controlled to guarantee the best quality of the study.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Ethical Committee from Universidade Cidade de São Paulo (UNICID), with approval no. CAAE: 34569214.5.0000.0064.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study.