
Abstract
This case report discusses the rare and complex occurrence of an advanced abdominal pregnancy in a 36-year-old multiparous woman at 26 weeks of gestation, compounded by chronic pelvic inflammatory disease and Fitz-Hugh–Curtis syndrome. The patient was presented with severe symptoms, including abdominal pain, fever, chills, constipation, and vaginal spotting, leading to her hospital admission. Diagnosis was challenging due to the advanced stage of the pregnancy and its abdominal location, particularly in the Douglas pouch, as detected through ultrasonography. According to anatomical standards, this is an intraperitoneal pregnancy rather than an intra-abdominal pregnancy because the fetus developed in the peritoneal cavity. This case is significant for illustrating the critical need for high clinical suspicion and skilled sonographic evaluation to identify such advanced abdominal pregnancies. The successful management of this case through laparotomy, despite the complexities of concurrent conditions, emphasizes the possibility of safe placental removal without increased hemorrhage risk. This report highlights the importance of awareness and expertise in handling rare presentations of ectopic pregnancies, underscoring the potential for positive outcomes with appropriate surgical intervention.
Keywords
Introduction
Abdominal ectopic pregnancy (AEP) is a rare occurrence where the pregnancy develops in the peritoneal cavity, outside the normal reproductive organs like the uterus, fallopian tubes, and ovaries. This condition is relatively uncommon, with its global prevalence ranging between 1 in 10,000 and 1 in 30,000 pregnancies. 1 According to the Centers for Disease Control and Prevention (CDC), the estimated incidence of abdominal pregnancy is 1 in 10,000 live births or 1.4% of all ectopic pregnancies. 2 Some cases are primary, resulting from intra-abdominal implantation, whereas others are secondary implantations of aborted tubal pregnancies. 3 The implantation sites include the omentum, the peritoneum, the pelvic sidewalls, the pouch of Douglas, and the various abdominal organs. 4 Because of the variable location in the abdomen, a wide range of signs and symptoms are described. Most often, abdominal pregnancy is misdiagnosed as a tubal ectopic pregnancy. 5 Only 20%–40% of cases are diagnosed preoperatively based on ultrasonographic findings. 6
Advanced abdominal pregnancy refers to pregnancies that have continued beyond 20 weeks of gestation with a live fetus, or showing signs of having once lived and developed in the peritoneal cavity. 7 These signs of having once lived include fetal movements felt by the mother, detectable fetal heartbeat, and development of fetal structures visible on ultrasound. It is mostly seen in women with a previous history of uterine surgery, dilatation and curettage, pelvic inflammatory disease (PID), or in vitro fertilization. 8 Advanced abdominal pregnancy is associated with a high risk of maternal mortality, about seven to eight times that of ectopic pregnancy, due to hemorrhagic shock and coagulopathy. 9
In this case report, we present the case of a multiparous woman with chronic PID and Fitz-Hugh–Curtis syndrome presenting with an advanced non-viable abdominal pregnancy. To the best of our knowledge, this is the first case of abdominal pregnancy diagnosed in Lebanon, and the first in literature to be associated with chronic PID and Fitz-Hugh–Curtis syndrome.
PID is an infection of the female reproductive organs, typically caused by sexually transmitted bacteria spreading from the vagina to the uterus, fallopian tubes, or ovaries. It can lead to chronic inflammation, scarring, and serious complications, including infertility, ectopic pregnancy, and chronic pelvic pain. 10 Although the Fitz-Hugh–Curtis syndrome is a rare complication of PID characterized by inflammation of the liver capsule, leading to the formation of violin-string adhesions between the liver and the abdominal wall. It often presents with right upper quadrant abdominal pain and can mimic other conditions such as gallbladder disease. 11
Case presentation
A 36-year-old patient, gravida 8, para 5, and aborta 2, at her 26th week of gestation by Last Menstrual Period (LMP), presented to the emergency department at Rafik Hariri University Hospital with an acute onset of severe abdominal pain that has been gradually increasing in intensity over the preceding 2 days, and associated with fever and chills. She mentioned constipation for the last 2 months prior to the presentation. She was not followed during her pregnancy and reported recent decreased fetal movements with some episodes of vaginal spotting. She is known to have chronic kidney disease and underwent one prior dilation and curettage procedure for a first trimester spontaneous abortion. Her family history was insignificant.
Physical examination revealed a conscious, cooperative, and oriented woman, with pallor and bad hygiene. She was afebrile but tachycardic. Her abdomen was soft, distended, with diffuse tenderness. Vaginal spotting was also noted. A bedside ultrasound identified a non-viable fetus but could not locate the placenta. The pelvic exam revealed a closed cervix. She was then referred for an official ultrasound by our maternal and fetal medicine specialist. This confirmed a non-viable pregnancy commensurate with 25 weeks of gestation. However, her pregnancy was not intra-uterine. The uterus appeared empty. Both the fetus and the placenta were seen posterior to the uterus, with anhydramnios (Figure 1). Abundant peritoneal fluid was also noted reaching Morrison’s pouch and interpreted as hemoperitoneum (Figure 2). A laparotomy was urgently arranged. Investigations revealed leukocytosis (WBC count = 18 × 109/L), elevated C-reactive protein (CRP = 300 mg/dl), and a normal hemoglobin level for a woman in her second trimester of pregnancy (Hb = 11.1 g/dl).
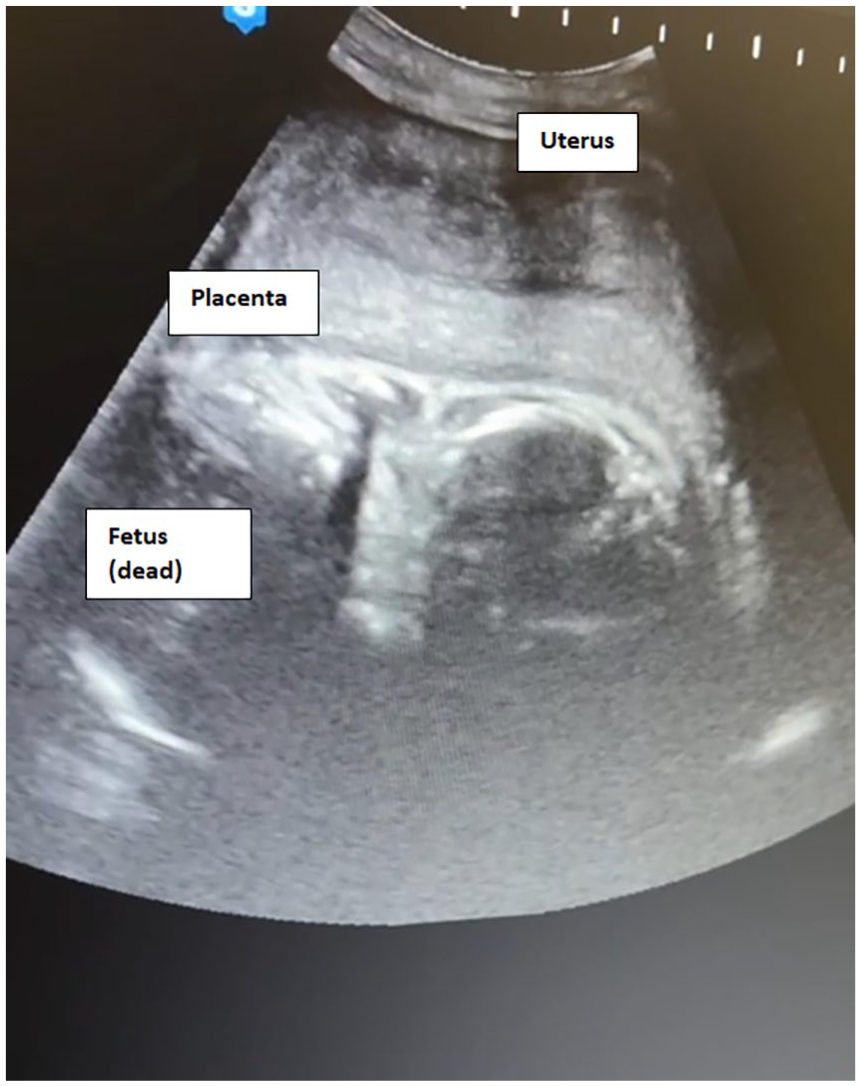
Transabdominal ultrasound. The fetus and placenta are seen posterior to an empty uterus.

Transabdominal ultrasound. The Morrison’s pouch is filled with abundant peritoneal fluid and violin-string adhesions suggestive of Fitz-Hugh–Curtis syndrome.
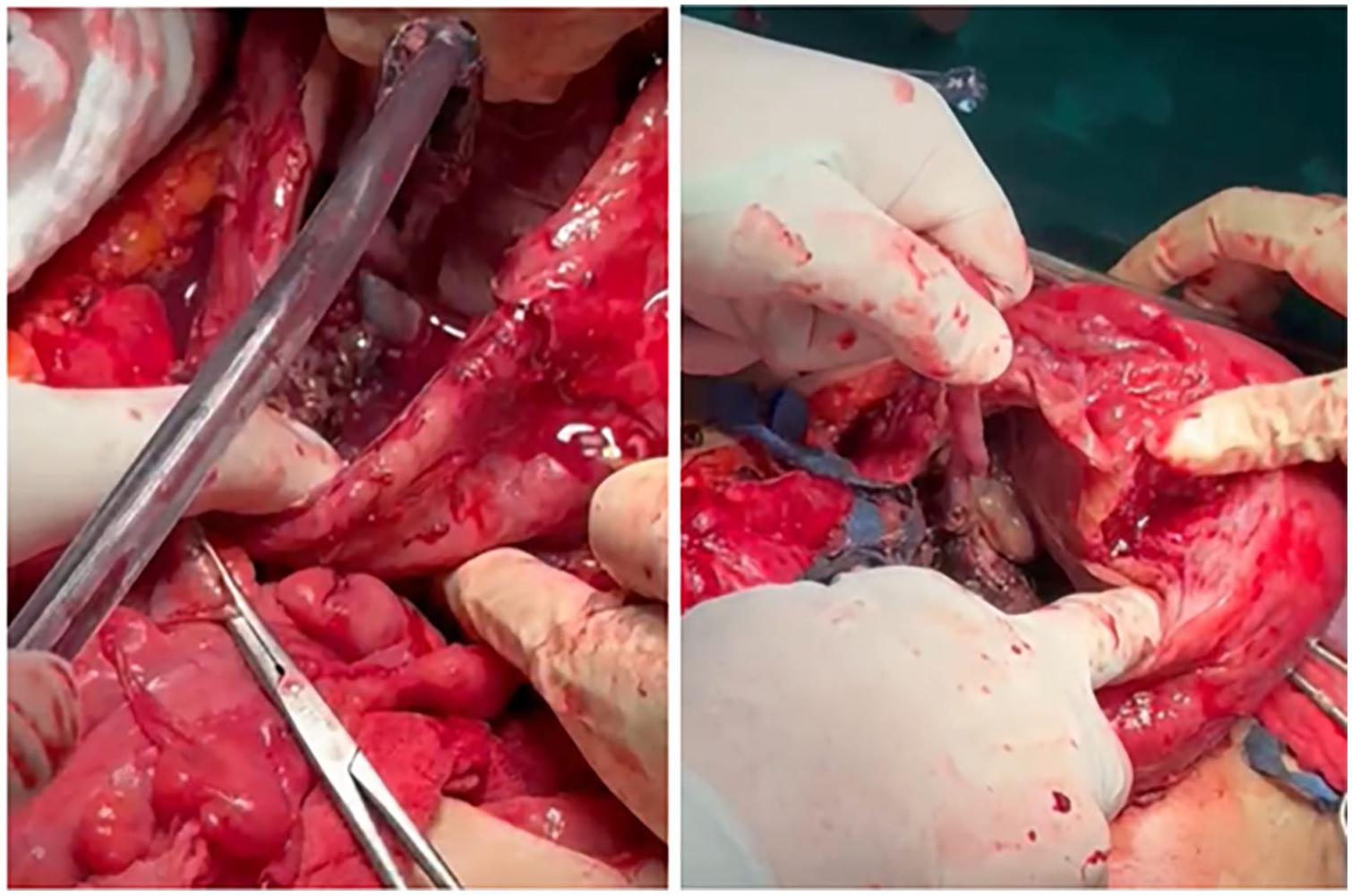
Intra-operatively, a large amount of blood-tinged peritoneal fluid with pus was suctioned from the peritoneal cavity and sent to culture. Extensive violin-string adhesions were observed at the liver capsule suggestive of Fitz-Hugh–Curtis syndrome. The uterus was noted to be boggy with an irregular anatomy. Its posterior wall showed an abnormal bulge that was firmly adherent to the nearby sigmoid colon (Figure 3). The left ovary was normal in size and contoured with ipsilateral hydrosalpinx (Figure 3). However, the right adnexa were engulfed by extensive intra-abdominal adhesions and could not be localized. Adhesiolysis was performed to free the adherent bowels, and this allowed a better visualization of the posterior uterine wall. The exact location of the pregnancy could not be identified due to the distorted anatomy; thus, the decision was to proceed with a fundal uterine incision extending downward and backward to the posterior bulge. This identified the non-viable female fetus and allowed its delivery (Figure 4), and revealed a severely infected, friable, and necrotic uterine cavity (Figure 5). During the operation, when we opened the peritoneum, we encountered a severely macerated fetus, which had contributed to the destruction and distortion of the normal anatomical landmarks, making it challenging to initially identify the exact location of the pregnancy. Although an incision was made in the fundal region of the uterus in an attempt to locate the pregnancy, the uterine cavity was found to be empty. This confirmed that the pregnancy was not intrauterine. The fetus was located outside the uterus within the peritoneal cavity, and the placenta was adherent to the posterior uterine wall. These findings support the diagnosis of an advanced abdominal pregnancy rather than an intrauterine pregnancy complicated by fetal demise and infection. The extensive adhesions, necrosis, and empty uterus observed intraoperatively align with the diagnosis of an intraperitoneal pregnancy, complicated by severe infection and distorted anatomy.

Posterior uterine wall. Abdominal pregnancy posterior to the uterus, and adherent to the adjacent sigmoid colon. (a) Posterior uterine wall, (b) abdominal pregnancy, (c) sigmoid colon, and (d) left fallopian tube.

Fetal delivery. The fetus and underlying placenta posterior to the uterus.

Uterine cavity. Necrotic endometrial tissue and pus filling the endometrial cavity of the uterus.
Figure 4 provides the surgical procedure involving the removal of a fetus from an advanced abdominal pregnancy. The fetus and the underlying placenta were located posterior to the uterus, within the peritoneal cavity. During the surgery, the baby was removed from the abdominal cavity (intraperitoneally). The umbilical cord was attached to the placenta, which was connected to the uterus. However, it is crucial to clarify that the placenta was not inside the uterine cavity. Instead, the placenta was external to the uterus, specifically attached to the posterior wall of the uterus. This situation can create a complex and misleading appearance during surgery. The fetus developed outside the uterus, and the placenta was adhered to the serosal surface of the posterior uterine wall, making it appear as though it might be within or closely associated with the uterine cavity. However, careful examination confirmed that the placenta was indeed external, and the pregnancy was intraperitoneal, not intrauterine.
After clamping the cord, the necrotic placenta was seen in the Douglas pouch (Figure 6). All placental tissue was removed with caution, and without any injuries to the nearby rectum. Careful exploration clarified that the peritoneum was surrounding the abdominal pregnancy in the posterior uterine wall and Douglas pouch. It was fused with the posterior uterine wall serosa, forming a pseudo-sac around the fetus. Total hysterectomy with bilateral salpingectomy and right oophorectomy was then performed to remove the necrotic and infected uterus. In this case, a right oophorectomy was deemed necessary for the 36-year-old patient due to the acute abdomen presentation, with mixed and distorted anatomy, and the presence of significant necrosis and pus. The fetus was located within the peritoneal cavity, leading to a complex surgical environment. The extensive infection and necrosis required thorough debridement, and the right ovary was involved in the inflammatory and infectious process, necessitating its removal to prevent further complications and ensure comprehensive treatment of the infected and necrotic tissues. All tissues and products of conception were sent to pathology. Two large intra-abdominal drains were inserted.
Placenta. Necrotic placental tissue in the Douglas pouch.
Postoperatively, the patient was hemodynamically stable and afebrile. She received broad-spectrum antibiotics for her PID. She refused workup for sexually transmitted diseases. Her drains were removed on day 5 postoperatively after their output became insignificant. Pathological examination confirmed an abdominal pregnancy and showed an ischemic and inflamed placenta.
Discussion
Abdominal pregnancy can implant anywhere within the peritoneal cavity, exclusive of the tubal, ovarian, or broad ligament locations. The Douglas pouch is the most common location, followed by the mesosalpinx and omentum.7,12 Re-implantation of a tubal pregnancy in the peritoneum is the most common cause, allowing the growth of a secondary abdominal pregnancy. 13 However, a primary abdominal pregnancy results from intra-abdominal fertilization and implantation. 4 The diagnosis of primary abdominal pregnancy is made by fulfilling the Studdiford’s criteria, which include (a) normal bilateral fallopian tubes and ovaries, (b) the absence of a uteroplacental fistula, and (c) pregnancy related exclusively to the peritoneal surface and early enough to eliminate the possibility of secondary implantation. 14 Watrowski et al. 15 recently expanded the classic Studdiford’s criteria after they reported a case of omental pregnancy invading the Douglas pouch.
In this case, although the pregnancy developed outside of the uterus, the uterine cavity was opened during the operation due to the complex and altered anatomy observed intraoperatively. The patient presented with an acute abdomen with significant necrosis and pus within the peritoneal cavity. The extensive infection and inflammation affected the uterus, leading to an abnormal bulge on its posterior wall adherent to the nearby sigmoid colon. Although there was no uteroplacental fistula, the necrotic material inside the uterus necessitated its removal to control the infection and prevent further complications.
The uterine cavity was explored to ensure complete removal of the infected and necrotic tissues. Thus, the decision to perform a total hysterectomy with bilateral salpingectomy and right oophorectomy was made based on the need to manage the extensive infection and altered anatomy, rather than the presence of a uteroplacental fistula. This case highlights the complexity of abdominal pregnancies and the necessity for individualized surgical approaches based on the specific intraoperative findings.
Additionally, the significance of regular screening programs for the prevention of gynecological malignancies cannot be overstated. Early identification and management of conditions like PID can prevent complications such as ectopic pregnancies and associated complex presentations. According to Ferrari and Giannini, 16 approaches to the prevention of gynecological malignancies through regular screenings and early interventions are crucial in improving reproductive health outcomes and reducing the risk of malignancies. Furthermore, recognizing predictors of pain development following procedures like laparoscopic adnexectomy is essential for optimizing patient outcomes in gynecological surgery. 17
They concluded that secondary implantation can occur after primary implantation at any ectopic site, and not only the fallopian tubes. 15 With the inability to fulfill these criteria, in our case, a diagnosis of secondary abdominal pregnancy was made.
The clinical presentation of advanced abdominal pregnancy varies, but severe abdominal pain with distention are the most consistent findings, as seen in our patient. 18 Other clinical findings include suprapubic pain, missed periods, bloody vaginal discharge, gastrointestinal symptoms such as constipation, and bogginess in the Douglas pouch. PID, which is commonly diagnosed in women with multiple sexual partners, is a risk factor for ectopic pregnancy, including abdominal pregnancy. 19 In this case, the patient had symptoms that increased the suspicion of advanced abdominal pregnancy such as abdominal pain, cessation of fetal movements, recent vaginal spotting, and a closed and uneffaced cervix. The latter is a condition in which the liver capsule becomes involved with inflammatory exudate that will later on leave violin-string shaped adhesions. 20 Recent data indicate that chlamydia trachomatis, in addition to Neisseria gonorrhea, may play an important role in this peri-hepatitis.
Ultrasonography remains the first-line tool for diagnosing abdominal pregnancy. Outlined the sonographic criteria for diagnosing abdominal pregnancy which include (a) demonstration of a fetus in a gestational sac outside the uterus, or depiction of an abdominal or pelvic mass identifiable as the uterus separate from the fetus, (b) failure to see a uterine wall between the fetus and urinary bladder, (c) recognition of a close approximation of the fetus to the maternal abdominal wall, and (d) localization of the placenta outside the uterine cavity. 21 Other findings include oligohydramnios and an unusual fetal lie. 22 Most of these sonographic criteria were met in our case. MRI can be used as an alternative imaging modality. It can delineate the exact anatomical relationships of the fetus, placenta, and maternal intra-abdominal organs, and also detail the vascular and placental organ invasion for preoperative planning. 23
In this case, fetal non-viability was diagnosed sonographically by a negative fetal heart rate. The fetal mortality rate in advanced abdominal pregnancy is very high, reported at 75%–95%. 24 A non-viable advanced abdominal pregnancy can be misdiagnosed as a non-viable intrauterine pregnancy, and medical termination may be attempted. 25 Failure of medical termination could have hazardous effects and increase the risk of maternal mortality from severe hemorrhage. Hence, the sonographer’s experience and a high index of suspicion are of utmost importance in case of questionable findings to avoid the consequences of failed medical termination.
Once an advanced abdominal pregnancy is diagnosed, open laparotomy is usually required to allow better exposure and access to the fetus and the placental implantation, and to allow better control of bleeding. 22 Laparoscopic surgery is reserved for early abdominal pregnancies. 26 Depending on the placental insertion site, the placenta may be removed or left in situ. 22 The latter option is best in cases of extensive adherence to the bowels, and with high risk of hemorrhage. 25 However, if the placenta was left in situ, serial serum beta human chorionic gonadotrophin (β-HCG) levels should be obtained. The β-HCG level can regress to a normal value within a few months postpartum. 27 The use of adjuvant methotrexate is still controversial, although some consider it helpful in accelerating placental involution. 28 Close monitoring and follow-up are required in case the placenta was left in situ because maternal morbidity and mortality are increased, and this is usually linked to severe hemorrhage, bowel obstruction, bowel perforation, fistula formation, or disseminated intravascular coagulopathy. 18 In our case, a secondary abdominal pregnancy was determined due to the inability to satisfy all of Studdiford’s criteria, notably the absence of a uteroplacental fistula and the pregnancy’s exclusive relation to the peritoneal surface. Our patient’s presentation, including severe abdominal pain and a history of chronic PID and Fitz-Hugh–Curtis syndrome, increased the suspicion of advanced abdominal pregnancy. Sonographic findings aligning with Allibone’s criteria supported this diagnosis, and the decision for laparotomy was made. The careful removal of all placental tissue without increasing hemorrhage risk was successfully achieved in this case.
Fortunately, in our case, all placental tissue was successfully removed from the Douglas pouch, and the patient did not experience any of the aforementioned complications.
Additionally, in this case, the presence of chronic PID, a known risk factor for ectopic pregnancies, was instrumental in the pathogenesis of the advanced abdominal pregnancy. The patient’s history of chronic PID, combined with her past dilation and curettage (D&C) procedures, likely contributed to the altered anatomy and inflammatory environment conducive to ectopic implantation.
Chronic PID leads to inflammation and scarring of the reproductive organs, which can create an environment where a fertilized egg is more likely to implant outside the uterine cavity. The scarring and adhesions from PID can disrupt normal tubal function and facilitate abnormal implantation sites, such as the peritoneal cavity, leading to an abdominal pregnancy.
Differential Diagnosis
In this complex case, the differential diagnosis included several possibilities. One possibility was in utero fetal demise with subsequent infection. The patient’s presentation with severe abdominal pain, fever, and chills, combined with a non-viable fetus identified on ultrasound, suggested intrauterine fetal demise followed by an infection. This scenario was consistent with the findings of necrosis and pus in the peritoneal cavity.
Another potential diagnosis was placenta percreta. Initially, there was a concern that the condition might be placenta percreta, a severe form of placenta accreta where the placenta invades through the uterine wall and potentially attaches to other organs. This hypothesis was considered due to the extensive inflammation and the abnormal adherence of the placenta to the posterior uterine wall and nearby structures. However, during the surgical procedure, after removing the uterus and other affected organs, it became apparent that the removal of the placenta was not as complicated as expected. The placenta, although connected to the organs, did not exhibit the typical invasive characteristics of placenta percreta, where detachment would usually be more challenging and associated with significant bleeding. The relatively straightforward removal process indicated that the placenta was more superficially attached rather than deeply invasive.
The results of this study provide valuable insights into the management of advanced abdominal pregnancies, particularly in patients with chronic PID. This case report underscores the importance of high clinical suspicion and skilled sonographic evaluation in accurately diagnosing abdominal pregnancies, which are rare and often present with complex clinical pictures.
The successful surgical management of this case, including the safe removal of the placenta without significant hemorrhage, demonstrates that with careful planning and execution, positive outcomes are achievable even in challenging scenarios involving extensive infection and altered anatomy.
Furthermore, the study emphasizes the role of chronic PID as a significant risk factor for ectopic pregnancies, illustrating how past medical history can impact the pathogenesis of such conditions. Chronic inflammation of the bowel can lead to chronic PID as a complication, and PID is a crucial part of the pathophysiology of abdominal pregnancies.
Finally, it highlights the critical importance of preventive screening programs in gynecology. Early identification and management of PID through routine screenings can prevent complications such as ectopic pregnancies, improving overall reproductive health outcomes.
In clinical practice, this case underscores the need for high clinical suspicion and skilled sonographic evaluation in diagnosing advanced abdominal pregnancies. Clinicians should be vigilant, especially with patients presenting atypical symptoms and a history of PID. Successful management demonstrates the importance of meticulous surgical planning and specialized training to achieve positive outcomes, even in cases with extensive infection and altered anatomy.
For future research, this case highlights several areas of interest. Further studies could explore the pathophysiological mechanisms linking chronic PID and abdominal pregnancies in greater detail. Investigating the effectiveness of various screening and intervention strategies for PID in preventing ectopic pregnancies could provide valuable insights into improving clinical outcomes. Additionally, examining the long-term reproductive health outcomes of patients who have experienced advanced abdominal pregnancies could contribute to a deeper understanding of the implications and management of such cases.
Strengths
This case report provides valuable insights into the management of advanced abdominal pregnancies, particularly in the context of chronic PID. It underscores the critical importance of high clinical suspicion, skilled sonographic evaluation, and meticulous surgical planning. The successful surgical outcome despite the complexities involved demonstrates the potential for positive outcomes with appropriate expertise and intervention. Additionally, this case highlights the role of chronic PID in the pathophysiology of abdominal pregnancies, contributing to a deeper understanding of the condition.
Limitations
One significant limitation of this case report is the lack of detailed prenatal care information due to the patient’s absence of follow-up during pregnancy until her emergency presentation. This limitation underscores the challenge in managing patients who, for various reasons, do not seek regular prenatal care. The absence of this information restricted our ability to fully understand the progression of the abdominal pregnancy and potentially identify earlier intervention opportunities. Additionally, the initial difficulty in locating the placenta highlights the challenges and limitations in diagnosing complex ectopic pregnancies, even with advanced imaging techniques.
Another limitation was the impact of the ongoing crisis in Lebanon, which constrained the hospital's resources. There was a lack of instruments and materials, which could have influenced the management and outcomes of the case. These limitations emphasize the need for increased awareness and education on the importance of prenatal care, as well as further research into improving diagnostic capabilities for rare and complex pregnancy cases like abdominal pregnancies.
Conclusion
Our case underscores the rarity and clinical intricacies of advanced abdominal pregnancy, especially when associated with chronic PID and Fitz-Hugh–Curtis syndrome. Despite advancements in imaging technologies, diagnosing abdominal pregnancy remains a significant challenge. It is crucial to understand the causal relationship between chronic PID and the development of Fitz-Hugh–Curtis syndrome, which subsequently increases the risk of ectopic pregnancies. This case reiterates the importance for obstetricians and gynecologists to maintain vigilance for abdominal pregnancy and consult experienced sonographers for accurate diagnosis. When feasible, and without risk of hemorrhage or bowel injury, safe removal of the placenta is recommended in such complex cases.
Footnotes
Acknowledgements
We extend our heartfelt thanks to Hamza Nakib for his invaluable contribution to the editing and formatting of our manuscript. His meticulous attention to detail, expertise in enhancing the clarity and flow of our writing, and dedication to ensuring the manuscript meets the highest standards of English language and formatting have significantly elevated the quality of our work. His efforts have been instrumental in preparing our manuscript for submission, and we deeply appreciate his commitment to excellence.
Author contributions
Charlotte El Hajjar: Provided overall supervision and guidance throughout the research and manuscript preparation phases. Hawraa Mohamad: Responsible for writing the initial draft of the manuscript, laying the foundation for subsequent contributions. Khouloud Demachkie: Offered supervision and played a pivotal role in the conceptualization of the study. Georges Yared: Provided supervision and valuable advice, contributing to the development of the research framework. Mohammad Siblini: Provided critical supervision during the surgical operation, ensuring procedural precision and patient safety throughout the intervention. His expertise significantly contributed to the successful outcome of the surgery. Mohamad Ramadan: Offered supervision and consultation, ensuring the research methodology and analysis were rigorously applied. Jihad El Hassan: Contributed to the project through supervision, ensuring the study’s objectives were met and upheld. Kariman Ghazal: Played a multifaceted role including supervision, writing, data correction, and overall manuscript preparation, ensuring the study’s findings were accurately and effectively communicated. Hassan Barakat: Provided supervision and was responsible for the clinical case, playing a critical role in the study’s conception and design.
Data availability statement
The data supporting the findings of this study are available upon request from the corresponding author.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval to report this case series was obtained from Rafik Hariri Hospital by Dr. Georges Yared.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.