
Abstract
Post femtosecond laser-assisted in situ keratomileusis corneal flap inversion trauma is an exceptionally rare and challenging complication in ophthalmology, highlighted by a case involving a 29-year-old woman who suffered an eye injury from ice chips 10 months after undergoing bilateral femtosecond laser-assisted in situ keratomileusis surgery. The injury led to a corneal flap inversion and melting, exacerbated by a delay in seeking treatment due to the pandemic. When she finally presented for medical attention, her vision was severely compromised, with dense epithelial ingrowth obstructing the visual axis or blocking the pupillary entrance. Despite these complications, medical interventions to remove the epithelial cells and attempts to reposition the corneal flap were carried out. Although the flap could not be fully anatomically restored due to scarring and stromal melt, the patient experienced a remarkable recovery in vision, achieving 20/17 visual acuity 6 months post-surgery. This case illustrates that satisfactory visual outcomes can be achieved even when perfect anatomical restoration is not possible. It challenges the traditional focus on anatomical perfection in corneal surgery and highlights the potential for functional recovery to take precedence over anatomical correction, reducing the need for further risky procedures. The outcome stresses the importance of tailored patient management and careful assessment of the risks and benefits in complex surgical cases.
Introduction
Femtosecond laser-assisted in situ keratomileusis (FS-LASIK) is known for its long-term safety and stability.1,2 Despite this, complications like corneal flap displacement and epithelial ingrowth can arise years after the procedure, especially after trauma. These issues, extensively documented in literature, pose a significant risk to vision.3,4
Prompt treatment is crucial for managing FS-LASIK complications, though the approach should be tailored to individual cases, considering both the potential benefits and risks of immediate surgical intervention.5,6 This case illustrates a unique scenario where a patient, after suffering from a corneal flap tear and inversion without immediate treatment, leading to scarring and epithelial ingrowth in the inverted area, sought medical attention 2 months post-injury. At this point, surgical intervention was conducted despite the scarring preventing anatomical repositioning of the flap. Remarkably, the patient still achieved good visual outcomes. This case is crucial for understanding post-FS-LASIK complications, offering insights into alternative approaches when traditional methods are not suitable, especially highlighting the importance of tailored surgical decisions to prevent additional complications.
Case report
A 29-year-old female patient underwent bilateral FS-LASIK at the beginning of 2022. Postoperatively, her vision improved significantly, with uncorrected visual acuity (UCVA) of 20/17 in each eye. On October 17, 2022, while cleaning her refrigerator, her right eye was struck by a piece of ice. Due to the pandemic, she did not immediately seek medical attention at our hospital. Instead, she treated herself with levofloxacin eye drops and calf blood extract eye solution. She returned to our department for a follow-up visit at the end of December, more than 2 months after the injury.
At the time of her visit, the visual acuity in her right eye had significantly decreased to 20/33. Anterior segment photography of the injured eye revealed a dense cream-colored epithelial implantation focus on the temporal side of the pupil area surrounded by several scattered smaller implantation foci (Figure 1(a)). The red area is suspected to be a corneal flap tear injury and flap defect area, while the yellow area shows the corneal flap inverted inward (Figure 1(b)). Due to the prolonged period after injury and the presence of epithelial implantation, these two areas were asymmetrical in size suggesting edge melting of the corneal flap. High-definition optical coherence tomography (HD-OCT) (Figure 2) showed high-reflective epithelial implantation foci between corneal layers.
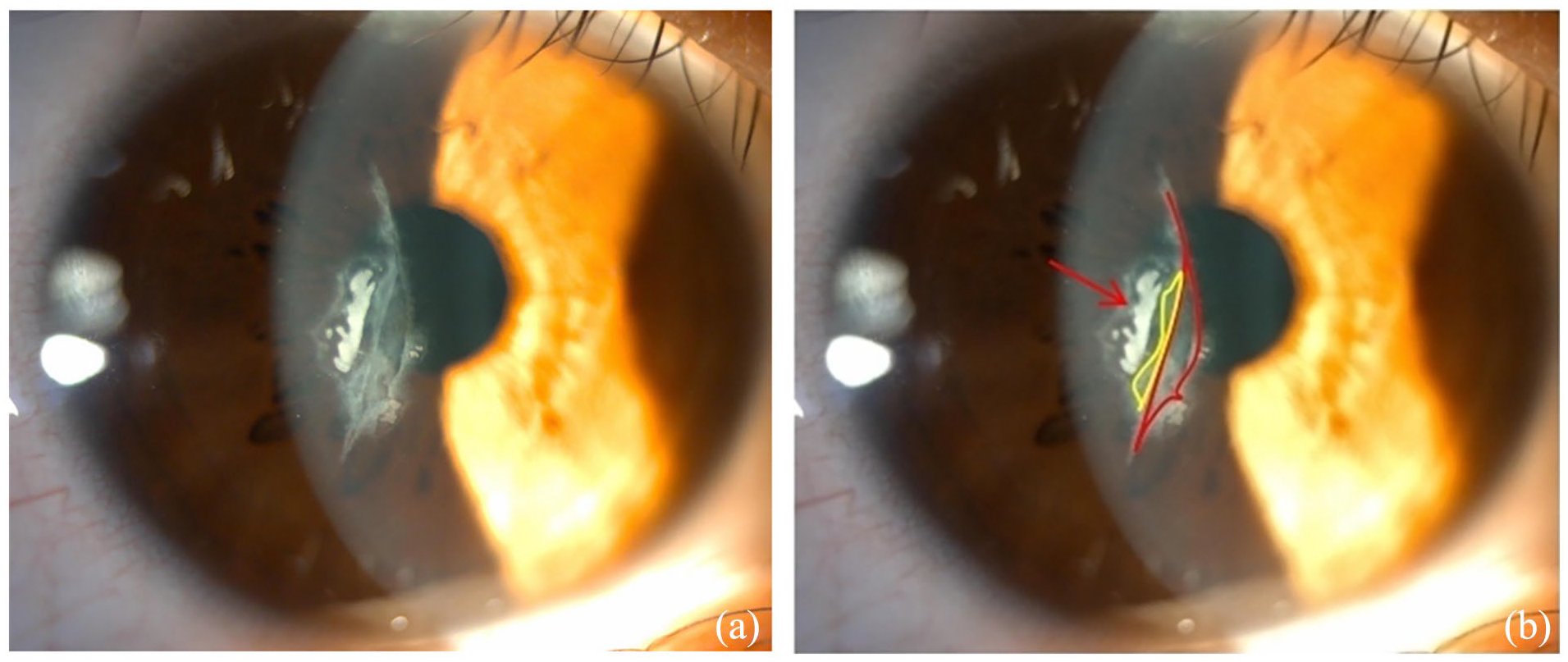
(a) Anterior segment photography of the right corneal trauma, showing the extent of the injury. (b) The arrow indicates a corneal epithelial implantation lesion. The red area is suspected to be a corneal flap tear injury and defect, while the yellow area shows the corneal flap inverted inward, highlighting the severity of the trauma.

Optical coherence tomography showing high-reflective epithelial implantation foci between the corneal layers, indicating the presence of significant epithelial ingrowth.
The patient was diagnosed with traumatic corneal flap epithelial implantation, traumatic corneal flap inversion, and flap melting, occurring after bilateral femtosecond surgery. Although it is generally recommended to promptly address such cases, the patient did not seek medical attention until 2 months post-injury due to the pandemic. In early January 2023, after assessing the dense epithelial implantation in the pupil area, we proceeded with the removal of the epithelial ingrowth and attempted to reposition the corneal flap. During the surgery, significant resistance was encountered when separating the epithelial implantation area, although removal from the corneal stroma bed was relatively smooth. However, repositioning the inverted corneal flap area was difficult due to stromal melt and scarring from the prolonged duration of the injury. Therefore, we decided to halt further attempts and instead opted for observation.
Postoperatively, we prescribed the patient tobramycin dexamethasone eye drops six times a day, gradually tapering off, and continued long-term medication until the stable period of corneal epithelial implantation, ulcerative keratitis, and melting had passed. The first day post-surgery photos showed that the epithelial implantation was effectively managed (Figure 3), with UCVA in the right eye of 20/40. HD-OCT images clearly showed the condition of the corneal flap inversion (Figure 4(a)), especially in the area marked with a red line (Figure 4(b)). A week later, her vision gradually improved to 20/25, and the refraction test showed a trend toward regularization. One month after surgery, the right eye UCVA recovered to 20/20. Six months post-surgery, the right eye UCVA reached 20/17. The previous imaging shows increased transparency in the lesion area of the patient’s right cornea (Figure 5). Changes in corneal light density clearly showed the cornea becoming more transparent (Figure 6). Two months post-trauma to 6 months post-surgery, the maximum corneal densitometry value of the right eye decreased from 53 grayscale units (GSU) to 26 GSU.

Photos taken on the first day post-surgery, demonstrating that the epithelial implantation was effectively managed, with a notable reduction in the implantation foci.

Corneal optical coherence tomography imaging 1 day after trauma surgery. (a) The arrow indicates the corneal epithelium is not completely filled. (b) The area marked with a red line suggests that the inverted corneal flap has not been repositioned.

The previous imaging shows increased transparency in the lesion area of the patient’s right cornea.
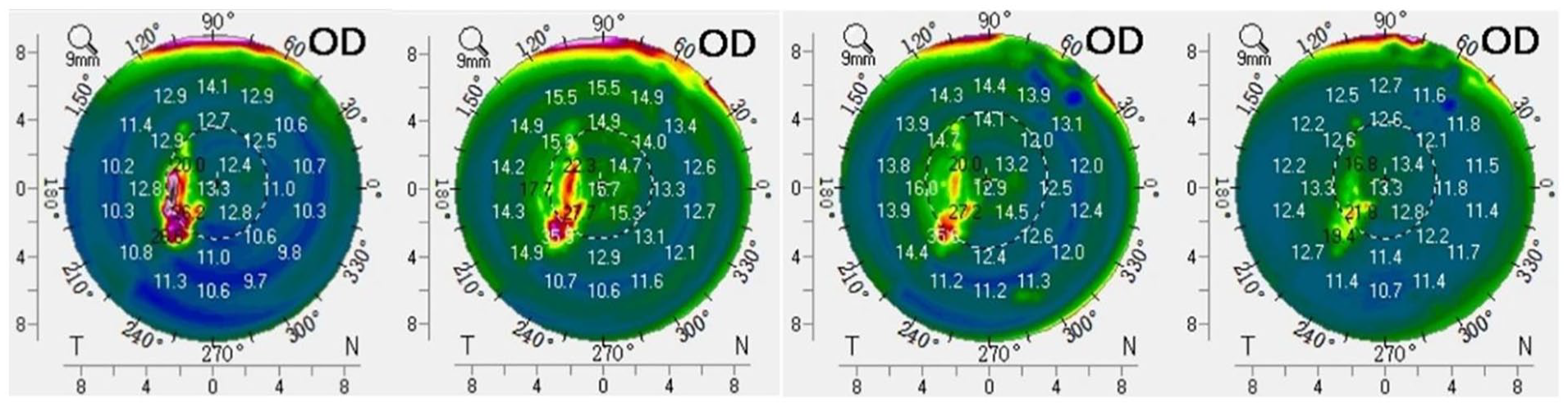
The patient’s right corneal optical density changes over time. (a) 2 months after trauma, showing significant opacity. (b) 1 week post-surgery, indicating initial improvement. (c) 3 months post-surgery, with further clarity. (d) 6 months post-surgery, showing significant recovery with reduced optical density, indicating successful restoration of corneal transparency.
Discussion
After LASIK surgery, reports of traumatic corneal flap dislocations, ruptures, folds, and epithelial ingrowth are quite common, with a variety of causes for these injuries. Delayed treatment can lead to complications such as epithelial ingrowth, flap striae, and scarring. Ting and Danjoux 7 highlights the paramount importance of early diagnosis and treatment for vision restoration. The sooner the treatment is initiated, the greater the likelihood of vision recovery, emphasizing the necessity for swift surgical intervention.
In the study conducted by Leccisotti et al., 8 a retrospective analysis of 37,315 eyes from 19,602 patients with flap dislocation or avulsion due to trauma revealed that while such traumatic flap complications are rare (occurring in only nine eyes), timely and appropriate treatment can lead to favorable anatomical and visual outcomes. This study underscores the importance of prompt treatment to achieve full recovery of UCVA.
Further, the research by Fernández-Barrientos et al. 6 focuses on the efficacy and safety of surgically managing late traumatic LASIK flap displacements in 66 cases. This study assesses the visual outcomes and complications associated with these displacements, highlighting the importance of immediate surgical intervention to improve visual results and minimize risks such as epithelial ingrowth. The findings suggest that although LASIK is generally safe, complications like flap displacement can occur, necessitating prompt and effective management to ensure favorable visual outcomes.
Overall, timely diagnosis and appropriate management are essential for achieving favorable visual outcomes, though not all cases require immediate intervention. These studies provide significant clinical lessons for ophthalmologists: to take decisive and effective treatment measures when dealing with potential traumatic complications following LASIK surgery.
In cases where epithelial ingrowth extends to the visual axis or edge of the pupil, or there is flap elevation or flap melting, surgical intervention is also required. As noted by Epstein et al., 9 in a case series of late flap removal after complicated LASIK, many patients with unsalvageable flaps showed good long-term outcomes. This finding is consistent with our observations that, despite the lack of ideal anatomical repositioning, the patient still achieved significant visual recovery. In this case, the patient experienced a corneal flap tear in the pupillary zone, and the corneal flap was folded over for an extended period without treatment, leading to corneal stromal necrosis and thinning, perhaps melting and scarring in the folded area of the corneal flap. 10 Consequently, ideal anatomical repositioning was not achieved during the initial repair procedure. We were also concerned about the potential need for a subsequent surgery. Upon analyzing the risks associated with a second intervention, we first noted that the patient’s pupillary zone corneal flap tear could be exacerbated by additional surgical procedures, potentially leading to decreased vision, increased risk of corneal flap melting, and infection. Furthermore, based on the experience from the initial procedure, the adhesion in the folded area of the corneal flap was tight, which would make repositioning challenging in any subsequent surgery. Fortunately, the patient’s vision stabilized. It is well-known that patients can achieve good visual acuity even without perfect anatomical restoration, as many cases involving corneal scars, haze, or lacerations affecting the visual axis still result in satisfactory vision. This case reinforces the importance of individualized patient management and careful assessment of risks and benefits in complex ophthalmic surgeries. This case provides valuable insights into achieving satisfactory outcomes through non-traditional means, especially when traditional surgical goals cannot be met.
Scraping ice from the refrigerator may seem like a trivial task in daily life, yet it is exactly these types of activities that should be approached with caution by patients who have recently undergone eye surgery. On the one hand, there is a need for patients to increase their awareness of the potential risks associated with seemingly harmless household tasks. On the other hand, effective post-operative patient education is essential to reduce the risk of complications with the corneal flap. Alerting patients to the risks they may encounter after surgery and educating them on the precautions to take in case of an eye injury are key to preventing these complications. Ensuring that patients are well-informed about which activities to handle with care or avoid entirely during their recovery period is crucial for preventing these complications.
In this case, due to special circumstances, the patient was unable to seek medical attention in time, leading to the corneal flap in the pupillary zone remaining folded after the repositioning surgery, failing to achieve “anatomical repositioning.” However, after effectively removing the implanted epithelium and postoperatively administering corticosteroid eye drops, intraocular pressure-lowering eye drops, and artificial tears, no epithelial implantation was observed during a 6-month follow-up. The condition was well controlled and vision gradually improved with the right eye’s vision recovering to 20/17. Another reason for the improvement in visual acuity, despite the lack of anatomical success, could be not only the removal of epithelial ingrowth, the use of corticosteroids, or controlling inflammation, but also epithelial hyperplasia and remodeling. These processes can sometimes mask and cover up many of the irregularities seen in patients with corneal lacerations, tears, and other abnormalities. The significant vision recovery can be attributed to the following factors: timely and effective surgical intervention, which, despite not achieving perfect anatomical repositioning, successfully removed the epithelial ingrowth and reduced obstruction to the visual axis; a reasonable postoperative medication regimen, particularly the use of corticosteroid eye drops, which controlled inflammation and scarring; and long-term postoperative observation and appropriate medication adjustments, ensuring corneal transparency and functional recovery. A study by Janiszewska-Bil et al. 11 demonstrated that changes in corneal cap thickness after small incision lenticule extraction (SMILE) surgery are crucial for the recovery of corneal biomechanics postoperatively. Similarly, in our case, although complete anatomical restoration was not achieved, the patient’s vision significantly improved, highlighting the critical role of corneal thickness and biomechanics in postoperative recovery. This flexible treatment strategy provides valuable experience and new insights for managing similar cases in the future. This suggests that surgeons might consider a temporary “functional repositioning” in certain special circumstances, observing before deciding on further treatment plans. This flexible treatment strategy, although deviating from the conventional path, proved effective and provides us with valuable experience, offering new insights for treating similar cases in the future.
Conclusion
Despite the presence of scarring, the patient’s vision improved significantly, achieving 20/17 visual acuity 6 months post-surgery. This case demonstrates that in special circumstances, adopting a flexible treatment strategy can still achieve the best possible outcome, challenging the traditional focus on anatomical perfection in corneal surgery.
Footnotes
Acknowledgements
We express our gratitude to the patient for her enthusiastic participation in the study.
Author contributions
H.X.W. and X.Z. were responsible for the study design and critical manuscript revisions. H.X.W. and W.J.L. conducted HD-OCT and anterior segment photography evaluations. X.W.G. and W.J.L. performed literature reviews. All authors read and approved the final manuscript.
Data availability statement
All data generated or analyzed during this study are included in the published article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Youth cultivation project from Xinjiang 474 Hospital (the former 474 Hospital of the People’s Liberation Army), which supported the scientific research projects. Associated grant numbers: 2022jzbjl103. Science and Technology Plan Project of the Urumqi Municipal Health and Wellness Committee, with the grant number 202361, and the General Program of the Natural Science Foundation of the Xinjiang Uygur Autonomous Region, with the grant number 2023D01A99.This fund supports collection, analysis, and interpretation of data.
Ethics statement and informed consent
This study received approval from the Ethics Committee of the General Hospital of Xinjiang 474 Hospital (formerly 474 Hospital of the People’s Liberation Army) with approval number A2024-084, and adhered to the Declaration of Helsinki. Informed consent was signed by all participants prior to the study. Written informed consent for publication of this case report and any accompanying images was obtained from the patient. A copy of the written consent is available for review by the journal’s editor.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article