
Abstract
Thoracic combined spinal epidural anaesthesia offers the ideal perioperative anaesthesia and analgesia. A 78-year-old female presented to our hospital with a hypertensive emergency, non-ST elevation myocardial infarction and pulmonary effusion. Then the patient had abdominal pain, constipation and vomiting. When examined, there was significant abdominal distention. During a colonoscopy, there was a fungating mass lesion 20 cm from the anal verge. A biopsy was taken and showed intramucosal adenoma within tubulovillous adenoma with high-grade dysplasia. The patient underwent exploratory laparoscopy and laparotomy (sigmoidectomy, colostomy) under thoracic combined spinal epidural anaesthesia at T9–T10 interspinous space. The patient was classified as ASA5 according to the American Society of Anesthesiologists physical status. The guidelines recommend utilizing regional anaesthesia instead of general anaesthesia for compromised elderly patients. In our case, we report the first case in Palestine of an ASA5 patient who successfully underwent abdominal surgery under thoracic combined spinal epidural anaesthesia.
Keywords
Introduction
Abdominal surgeries can be done either under general or regional anaesthesia (GA or RA). 1 The effects of GA can raise the risk of morbidity and mortality, especially for those with underlying medical conditions. Thus, a complete anaesthetic assessment and risk analysis are necessary when deciding whether to perform surgery on a patient who is comorbid with a poor functional baseline or who is systematically ill. 2
In 1981, Brownridge developed combined spinal and epidural anaesthesia, using the epidural and subarachnoid spaces. It is referred to as the ‘needle-through-needle’ method. 3 A case in the literature review showed that thoracic combined spinal anaesthesia can be used effectively for American Society of Anesthesiologists (ASA) I and ASA II patients with significant postoperative benefits. 4
We report a case that was managed successfully with thoracic combined spinal epidural anaesthesia (TCSEA) for an ASA5 patient undergoing exploratory laparoscopy and laparotomy.
Case presentation
A 78-year-old female came to our hospital as a case of hypertensive emergency, non-ST elevation myocardial infarction and pulmonary effusion. Afterwards, the patient developed abdominal pain, constipation and vomiting. A colononoscopy was done and showed a fungating mass lesion 20 cm from the anal verge (Figure 1). A biopsy was taken and showed intramucosal adenoma with high-grade dysplasia. After 1 week, an exploratory laparoscope was done, and it showed a gallbladder stone. Then a laparotomy (sigmoidectomy and colostomy) was done.
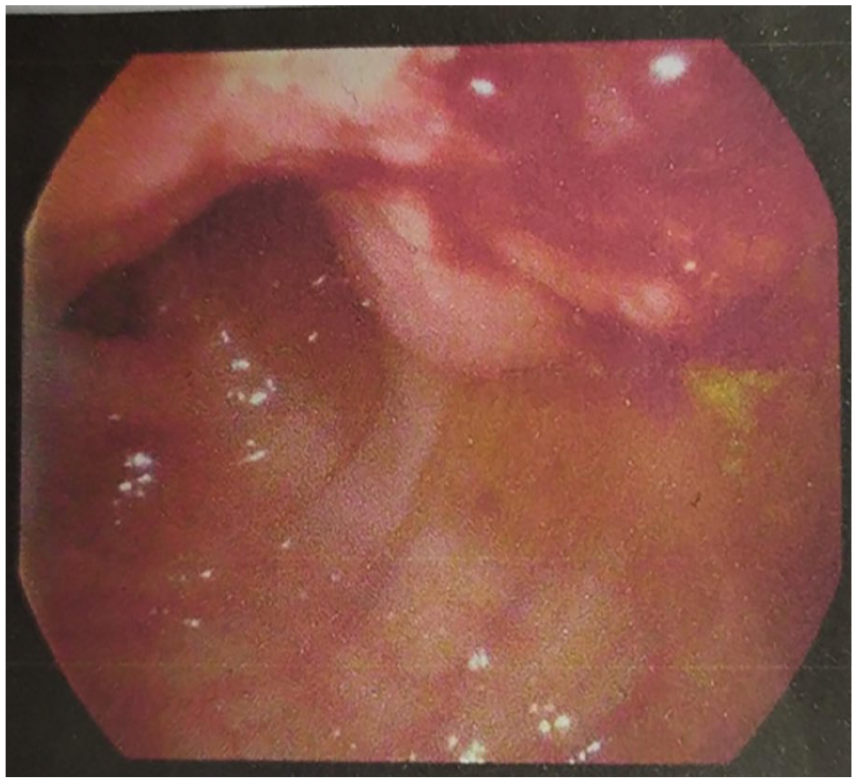
Colonoscopy shows fungating rectosigmoid mass lesion at 20 cm from anal verge measuring about 3–4 cm with central execration and without luminal narrowing.
The patient’s body mass index was 64.5; she was bedridden with a background of hypertension, type 2 diabetes mellitus, chronic kidney disease, ischaemic heart disease, heart failure, severe metabolic acidosis, pulmonary oedema, lower limb oedema and scoliosis. On chest auscultation, air entry was decreased bilaterally with bilateral basal crepitations. A chest X-ray was done, and it showed pulmonary effusion (Figure 2). Also, an abdominal computerized tomography was done, showing gallbladder hyperdensities, mostly stones, a few non-obstructive renal gravels and multiple renal cysts, mild-moderate cardiomegaly and degenerative changes of the spine and both sacroiliac joints (Figure 3). We decided to proceed with surgery under TCSEA to minimize potential chest complications. The patient’s baseline heart rate was 77 beats per minute, blood pressure was 166/107 mmHg and oxygen saturation was 88% on room air. Complete blood count shows WBC: 8.6, Hb%: 8.3 and platelets: 211.

The chest X-ray shows pulmonary effusion.

An abdominal CT scan shows gallbladder hyperdensities, multiple renal cysts, left parailiac lymph nodes, cardiomegaly, degenerative changes of the spine and sacroiliac joints and vascular calcification.
Combined spinal epidural anaesthesia (CSEA) was done. The patient was in a setting position while during surgery she was in a supine position with a 45° head elevation. We use 5 l of O2 through a nasal cannula and 100 ml of sodium bicarbonate, which is 8.4% due to metabolic acidosis (pH = 7.056, HCO2 = 13.2). The pressure of the peritoneum during laparoscopic surgery is 12–13 mmHg with a midline approach at T9–T10 interspinous space by using a Portex CSEA set that includes an epidural catheter, a 27-gauge Whitacre spinal needle and an 18-gauge Tuohy epidural needle. Through ‘loss of resistance’ to air, the epidural space was located at a distance of 4 cm from the skin; it was determined by measuring the length of the needle that protruded from the skin. A 27-gauge, pencil-point Whitacre spinal needle was inserted into the epidural space through the Tuohy needle until the dura mater’s resistance was felt. This allowed the distance between the dura mater and the Tuohy needle tip to be measured.
After piercing the dura, a locking device was used to keep the two needles attached and prevent the spinal needle from moving beyond the Tuohy needle’s tip. After the confirmation of a clear and unobstructed flow of Cerebrospinal fluid, 25 μg of fentanyl and 2 ml of preservative-free isobaric levobupivacaine 0.5% were given, and the spinal needle was taken out. Then the epidural catheter was fixed at 10 cm within the epidural space, the epidural was used by infusion, and 0.125% of Bupivacaine was used at a rate 6 ml/h. Surgery was started immediately after the target sensory block T4–T12, which was determined by a pinprick, was obtained. At the same time, a modified Bromage scale was used to evaluate the motor block. 5 Immediate hemodynamic changes following the administration of CSEA were mild hypotension (100/50), and the heart rate declined to 55 bpm. So we use IV fluid (500 ml of Ringer lactate) and 5–10 mg of ephedrine.
Intraoperatively, furosemide 40 mg was used; sodium bicarbonate 100 ml (8.4%) was used to correct severe metabolic acidosis; and midazolam injection boluses 0.5 mg were used to manage intraoperative anxiety. The patient was moved to the surgical intensive care unit to be monitored. On the third day after the surgery, the epidural catheter was taken out. Postoperatively, 0.125% of Bupivacaine was used at a rate 6 ml/h by infusion. All lab tests were done, including invasive monitoring in a semi-setting position and keeping the Mean arterial pressure above 65. Chest physiotherapy was done with an incentive spirometer. Arterial blood gas were done every 3 h. The patient was Nothing by mouth with laxatives. Random blood sugar is kept below 180. Limb exercise was done postoperatively. Follow-up was done at the critical care unit. Furosemide 60 mg three times was used, and anticoagulants (aspirin and Clopidogrel) were also used. By now, there is no need for surgical intervention; only medical management is needed.
Discussion
GA is useful as it reduces intraoperative patient awareness, allows the use of muscle relaxants and controls the airway, breathing and circulation. However, RA is advised in patients with comorbidities such as cardiac and pulmonary compromise. 6
CSEA has become popular. The capacity of a CSEA to combine the quick onset of the spinal block with the potential to prolong the regional block both intraoperatively and postoperatively is the primary cause of this development. 7 The CSEA is becoming a dependable and effective technique in the anesthesiologist’s toolbox. The method has proven to be better in Caesarean sections for analgesia during labour. It is successfully applied to various kinds of surgeries, but particularly to abdominal surgery. 3
The guidelines advise using RA rather than GA for compromised elderly patients. 8 Elderly patients frequently have no teeth, which makes mask ventilation more difficult, and they have less cervical extension, which makes direct laryngoscopy difficult. Our patient had scoliosis, which makes GA avoidable. Additionally, a variety of hypotensive and hypertensive reactions to induction drugs and to laryngoscopy are seen in those patients. 8
The patient had metabolic syndrome, described as ‘truncal’ obesity with insulin resistance, hyperglycemia, low High density lipoprotein (HDL), high triglyceride and hypertension. According to reports, there is an increased risk of surgery under GA for patients with metabolic syndrome. The most common perioperative complications include intubation problems and post-intubation respiratory distress caused by pulmonary atelectasis, due to a decrease in the vital and residual lung capacities in obese patients. 9
The patient was suffering from pulmonary oedema. Therefore, GA is dangerous due to its negative effects on lung function. It causes weaker pharyngeal muscles, less effective airway reflexes, coughing and colonization with Gram-negative bacteria. 10
Besides that, she was suffering from ischaemic heart disease and heart failure. Anaesthetic agents in elderly individuals can depress myocardial and vascular smooth muscle contraction, leading to unpredictable responses and decreased adaptability in surgical procedures. 8
She also had a chronic kidney disease, and as her Glomerular filtration Rate (GFR) declines, she is more vulnerable to electrolyte abnormalities, acid-base derangements and impaired reactivity to renin, angiotensin, aldosterone and vasopressin. 11 So to reduce these risks, we used CSEA.
Here, TCSEA has been used for both exploratory laparoscopy and laparotomy (sigmoidectomy, colostomy) for compromised ASA5 patients, making it special as GA is traditionally used during laparoscopic abdominal surgery rather than RA because of the respiratory changes. 12 In comparison with other cases in the literature review, TCSEA was used in laparoscopic cholecystectomy in healthy patients with a combination of GA. 3 Additionally, studies have been done on the effectiveness of spinal anaesthesia used alone or in combination with epidural anaesthesia for the lumbar spine but not for the thoracic spine. 13
Conclusion
Elderly patients with comorbidities have a higher incidence of morbidity and mortality when undergoing any operative procedure, which presents a challenge to anesthesiologists. This case report has demonstrated that ASA5 patients can benefit from TCSEA with significant postoperative benefits when administered properly. Even so, this technique requires anesthesiologists with deep experience in thoracic RA.
Footnotes
Acknowledgements
None.
Author contributions
M.R.M. contributed to writing and editing; S.A.M. contributed to data collection and writing; A.J. contributed to data collection and writing; K.T. contributed to editing and supervising; F.I. contributed to editing and supervising.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.