
Abstract
Bladder leiomyoma is a rare benign mesothelial tumor that is more commonly reported in women. Most patients present with frequent urination or obstructive urinary symptoms. Here, we portray a 50-year-old woman who presented to the clinic with abdominal pain and vaginal bleeding. Imaging showed a lobulated mass at the posterior aspect of the urinary bladder. The pathology of the surgery demonstrated a benign mesenchymal neoplasm composed of interlacing bundles of smooth muscle fibers with a whirling pattern, which eventually confirmed bladder leiomyoma. Although this tumor is benign, it can be misdiagnosed with other diseases such as a urothelial lesion or urothelial cell carcinoma of the bladder. Accordingly, it can inevitably affect patient management. Therefore, it must be diagnosed quickly and accurately and appropriate treatment should be applied.
Keywords
Introduction
Leiomyoma of the bladder could be an uncommon benign tumor that arises basically in middle-aged women. Even though no pathophysiological components have been portrayed to explain the development of this tumor, it may be related to an endocrine shift.1,2 Here, we report the case of a senior woman who primarily presented with abdominal pain and vaginal bleeding. She complained of frequent urination, pelvic pain, and a feeling of pelvic pressure. The mass detected within her bladder—by imaging techniques—was afterward histologically affirmed as leiomyoma.
Case report
A 50-year-old woman presented to the clinic with abdominal pain and vaginal bleeding. She had a history of diabetes and hyperthyroidism. In the drug history, she mentioned a history of taking insulin and levothyroxine (once a day). She had a history of refractory vaginal bleeding. On examination of the visual system, the conjunctiva was slightly pale. In the abdomen and pelvis, the area of the hypogastric region was tender and the large size of the uterus was palpable. The adnexa was free and the physical examination of the cervix and breast did not reveal any specific findings. Pap tests, blood and urine tests, and transvaginal ultrasounds were requested. Pap smear was normal and blood and urine tests revealed anemia and microscopic hematuria, respectively. On transvaginal ultrasound, the uterus was adenomyosis and contained multiple myomas. Transvaginal ultrasonography detected two masses, one measuring 20 mm × 30 mm posterior to the uterine fundus and the other measuring 57 mm × 73 mm anterior to the uterus. There was no space-occupying lesion in the endometrium and cervix and the size of the ovaries was normal. Magnetic resonance imaging (MRI) demonstrated a lobulated mass at the posterior aspect of the urinary bladder with 7.2 cm × 5.7 cm in diameter, which was presented as uterine leiomyoma (Figure 1). After contrast administration, there was an enhancement in the mass. An intramural and submucosal mass at the posterior portion of the body of the uterus with 3.1 cm × 2.8 cm in diameter was detected. Furthermore, a small intramural mass was indicated at the aspect of the uterus with measures approximately 1 cm × 1 cm in diameter (Figure 1). Both kidneys were normal in size and position. She was nominated for surgery due to refractory bleeding, pelvic pain and pressure, urinary symptoms, and desire for laparotomy. During the cystoscopy, the anterior mass of the uterine fundus was visible inside the bladder. Due to the size of the mass, transurethral resection for bladder tumor (TURBT) was not performed for the patient. She underwent a total abdominal hysterectomy (TAH), bilateral salpingo-oophorectomy (BSO), and partial cystectomy by laparotomy. Because the leiomyoma tissue had penetrated the bladder tissue, a partial cystectomy was performed. The reddish-white mass was noticed in the posterior aspect of the bladder wall thus partial cystectomy was performed (Figure 2). The pathology of bladder mass revealed a benign mesenchymal neoplasm composed of interlacing bundles of smooth muscle fibers with a whirling pattern (Figure 3) which the diagnosis of bladder leiomyoma was confirmed (Figure 4). The postoperative period was uneventful, and she was discharged after 3 days. During a 1-year follow-up period, the patient had no complaints of abdominal pain and vaginal bleeding, and bladder leiomyoma was not diagnosed by pelvic ultrasound and cystoscopic examination.

In the sagittal T2 view, low signal lobulated mass in superoposterior portion of bladder wall measuring 7.2 cm × 5.7 cm in diameter with significant enhancement in post contrast image shown by the red arrow.

Grossly, the mass is white-red in color.
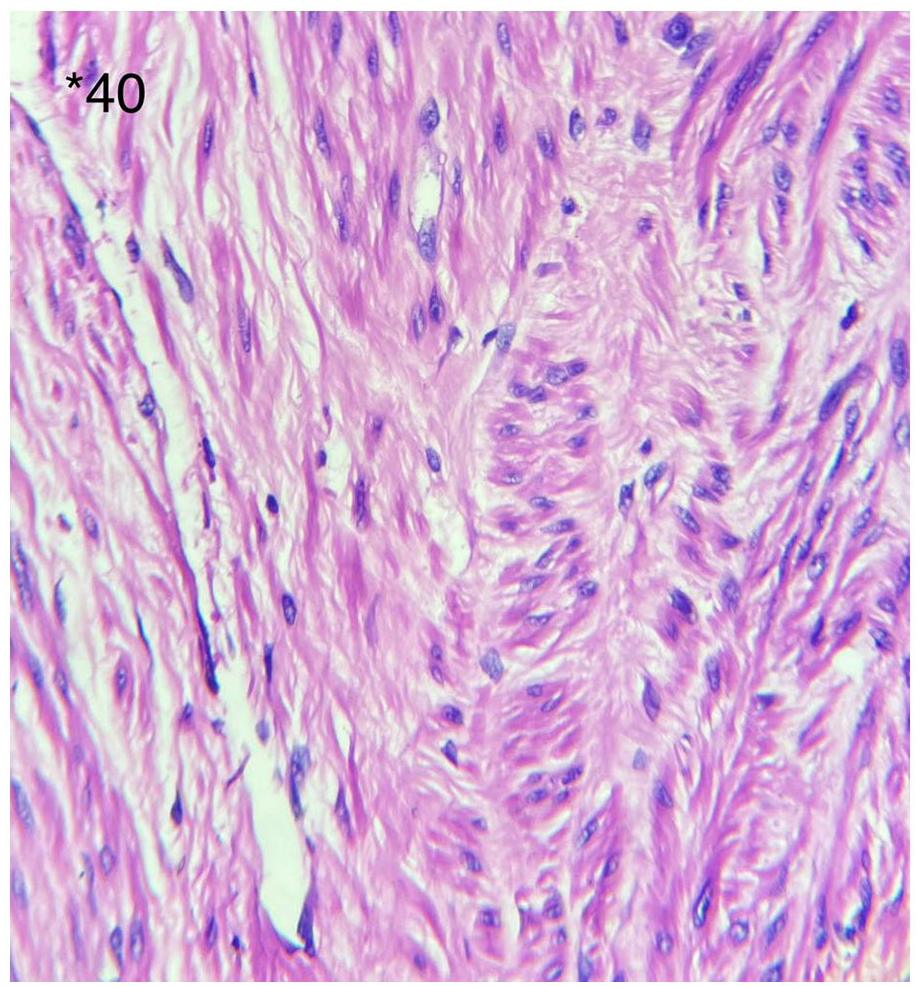
Bundles of elongate cells with eosinophilic cytoplasm and oval nuclei (H&E staining, ×40).

Immunostaining for smooth muscle actin shows diffuse and strong cytoplasmic positivity in smooth muscle cells.
Discussion
Bladder mesenchymal tumors, particularly leiomyomas, are moderately uncommon neoplasms emerging from the mesenchymal tissues ordinarily found within the bladder and compose 1% to 5% of all bladder neoplasms.2,3 In a separate study in 2013, an estimated 250 cases of bladder leiomyoma were reported from the past to 2013. 2 Reports indicate that this tumor is more common in women 40 to 60 years old with an average age of 44 years,2,4,5 demonstrating that sex discrepancy affects bladder leiomyoma occurrence. Due to the increasing incidence of bladder leiomyoma during pregnancy 6 and reports of cases of bladder leiomyoma with ovarian steroid receptors,6,7 it seems that bladder leiomyoma, like uterine leiomyoma, is associated with hormonal alternations. 8 The etiology of these benign tumors is not yet fully understood. Chromosomal changes, hormonal disorders, repeated bladder wall, and detrusor infection, perivascular inflammation, or dysontogenesis are assumed to be the etiology of bladder leiomyoma. 2
Bladder leiomyoma can be asymptomatic or, depending on the location of the tumor, can cause symptoms such as obstructive symptoms (49%), irritative symptoms (38%), hematuria (11%), and flank pain (13%). 9 Leiomyoma in the bladder neck may cause more severe symptoms than leiomyoma in the bladder wall. 10 Furthermore, bladder leiomyoma can cause certain symptoms, such as radiating pain in the left leg 11 or bacterial infection. 12 In our case, the patient presented with a complaint of abdominal pain and vaginal bleeding. Laparotomy was inevitable due to the invasion of the tumor into the urinary bladder as a presentation of uterine pedunculated leiomyoma. Our case and other studies have shown that although bladder leiomyoma is benign, it can cause various complications. So, it is critical to recognize the spectrum of symptoms. 12
Differential diagnosis of bladder leiomyoma with other maladies is particularly critical. Bladder leiomyoma may be confused with a urothelial lesion or urothelial cell carcinoma of the bladder, which should be careful in its differential diagnosis. 13 Traditional detection techniques of bladder leiomyoma contain ultrasound, computed tomography (CT), and MRI. 10 Homogeneous smooth lesions with peripheral hyperechogenicity are noticed on ultrasound. 14 Moreover, abdominal CT can detect the location of the leiomyoma and the difference between fluid-filled and a solid lesion. 2 However, MRI is preferable to CT to figure out the origin and recognize the boundary of the tumor. 10 Histopathologically, bladder leiomyoma is composed of bundles of smooth muscle fibers partitioned by connective tissue. 2 In our patient, a mass with a size of 57 mm × 73 mm in the posterior part of the urinary bladder was detected by transvaginal ultrasound and MRI. Moreover, transvaginal ultrasound of the uterus reported adenomyosis and myomatosis. After histopathological evaluation and observation of interlacing bundles of smooth muscle fibers with a whirling pattern, the diagnosis of bladder leiomyoma was confirmed. Reports confirm that the use of transvaginal ultrasound of the uterus along with MRI is an effective method to identify leiomyoma mass. 15
Endovesical masses have been for the most part differentiable (63%), conceivably because of its characteristic swelling into the bladder which actuated irritative complications and constrained the patient to attempt clinical treatment. The 2 different types of mass arise with a recurrence of 30% and 7% for extravesical and intramural, respectively. 16
Treatments can vary depending on the location and size of the tumor. Therapeutic options for bladder leiomyoma include TURBT, open surgery, and conservative. In addition, other less invasive surgeries that fall into the category of open surgery, such as laparoscopic cystotomy and robotic extramucosal excision, are appropriate for patients with bladder leiomyoma. 2 In this context, in one case of large urethral leiomyoma that had grown in the vesicouterine and vesicovaginal septum, the patient was well managed with laparoscopic surgery. Therefore, laparoscopic surgery can be proposed as a suitable and accurate procedure for the management of pelvic pathologies. 15 The use of open partial cystectomy for bladder leiomyoma, especially for large with extravesical growth masses or a tumor with a critical position and difficulty in distinction, can also be associated with an excellent prognosis. 17 However, in the current case, the patient refused to undergo laparoscopic surgery. Furthermore, it was not possible for the surgeon to perform this type of surgery due to the large size of the uterus, which contained multiple myomas, and the fact that laparoscopic surgery required special skills. 18 Apart from these issues, there were no facilities for laparoscopic surgery in our medical center. In patients with big endovesical tumors, extravascular growths, or intramural lesions, open resection is a decent choice and does not need a subsequent action. The patient is asymptomatic after surgical excision due to a low reoperation rate, nonappearance of relapse, and a great prognosis of leiomyoma.19,20 In this report, the patient’s vaginal bleeding was resistant to medications due to adenomyosis and multiple uterine myomas and she was a candidate for surgery due to age, refractory bleeding, anemia, abdominal pain, and pelvic pressure. In preoperative imaging, bladder leiomyoma was reported as uterine peduncle leiomyoma. As the leiomyoma tissue had involved the bladder tissue, a partial cystectomy was performed. In the future, the expansion of more accurate surgical techniques and diagnostic procedures may gradually become a major propensity in bladder leiomyoma management. Although bladder leiomyoma is a rare condition, we need to be watchful about this tumor’s potential complications as an important and treatable status in patients with critical conditions.
Conclusion
Leiomyoma of the bladder can cause abdominal pain and vaginal bleeding, which can be treated with different treatments depending on the location and size of the tumor. Leiomyoma bladder as a result of the uterine pedunculated leiomyoma should be watchfully considered. TAH and BSO can be effective in high-risk patients such as those with vaginal bleeding, relatively old age, and multiple uterine leiomyomas.
Footnotes
Acknowledgements
Special thanks to the Student Research Committee of Mazandaran University of Medical Sciences for supporting us in this project.
Author contributions
Z.N.: first operator in the case, planned and performed the procedure, and took decisions on hardware and technique used. Z.P.: assisted in procedure and drafted the manuscript. Z.T.: assisted in procedure. All authors read and approved the final version of the manuscript.
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article. A copy of the written consent is available for review by the editor-in-chief of this journal.