
Abstract
We report a case of endovascular treatment of bone cement embolism after percutaneous vertebroplasty. The patient underwent percutaneous vertebroplasty for acute L1 compression fracture. Two weeks later, the patient developed symptoms of pulmonary embolism. Computed tomography pulmonary angiogram confirmed the presence of a bone cement foreign body in the pulmonary artery. Endovascular treatment was performed, and the cement embolism was caught, pulled to the level of the iliac vein, and fixed with stents. At the 1-year follow-up, the patient did not have any complaints, postoperative computed tomography pulmonary angiogram showed no obvious manifestations of pulmonary embolism, and angiography showed that the bone cement was fixed in place and that the iliac veins were normal.
Introduction
Bone cement leakage is a common complication after percutaneous vertebroplasty. Most occurrences are related to local vertebral leakage, and patients have no obvious symptoms. 1 However, if bone cement leaks from its injection site through the anterior vertebral veins and embolizes the heart and pulmonary arteries, it will become a serious and potentially life-threatening complication. 2 The incidence of bone cement pulmonary embolism was 0%–25%. 3
The treatment of bone cement embolism is still unclear. The currently reported treatment methods include surgical treatment and conservative treatment. However, there is still controversy over whether to use conservative or surgical treatment. Most literature supports conservative treatment for asymptomatic bone cement embolism.4,5 Some symptomatic bone cement embolisms were also reported to achieve good therapeutic effects through conservative treatment. 6 Symptomatic patients with intracardiac cement embolism and pulmonary cement embolism underwent open surgery for cement removal.7,8 Only a very small number of patients received endovascular therapy. 9
Case presentation
A 68-year-old woman with a history of hypertension, atrial fibrillation, and hypothyroidism underwent percutaneous vertebroplasty for acute L1 compression fracture at a local hospital. After the surgery, chest tightness, shortness of breath, and palpitations developed. Two weeks later, the patient fainted and was sent to our emergency department. The arterial blood gas analysis showed hypoxemia. The electrocardiogram showed a long R-R interval of atrial fibrillation. Computed tomography pulmonary angiogram (CTPA) showed a foreign body (Figure 1) in the right main pulmonary artery. The other physical examination was unremarkable.

CTPA showed bone cement in the right main pulmonary artery.
Due to the large trauma and severe postoperative complications of open surgery, we chose to undergo emergency endovascular treatment. The 10F FuStar steerable sheath, and 6F multipurpose (MPA) catheter and snare were introduced from the femoral vein approach, and the end of the bone cement was caught and gently removed (Figure 2). The bone cement was caught in the bifurcation of the common iliac vein and could not be pulled out from either side of the iliac vein. Finally, two SMART Control stents (14 × 80 mm; Cordis, Florida, United States) were placed on the iliac veins on both sides to fix the bone cement in place (Figure 3). Administer anticoagulant therapy (Levaroxaban 20 mg qd) to patients after surgery for 6 months.
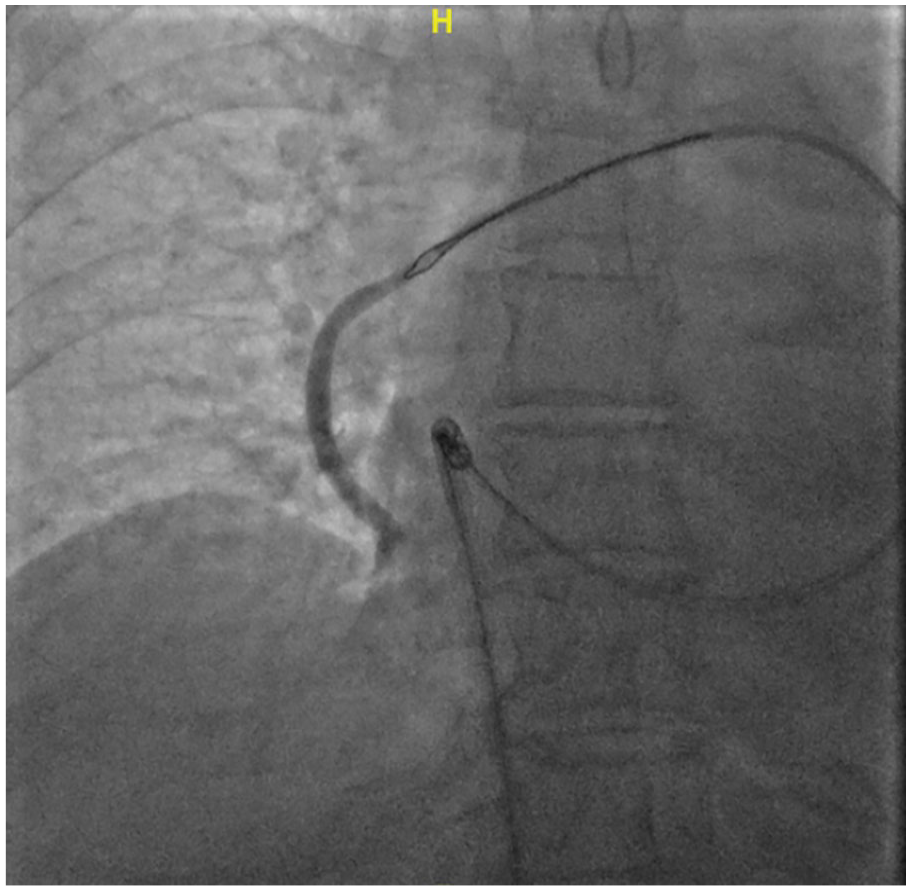
Introduced the 10F FuStar steerable sheath, 6F multipurpose (MPA) catheter and snare to catch the end of the bone cement and pull it out gently.
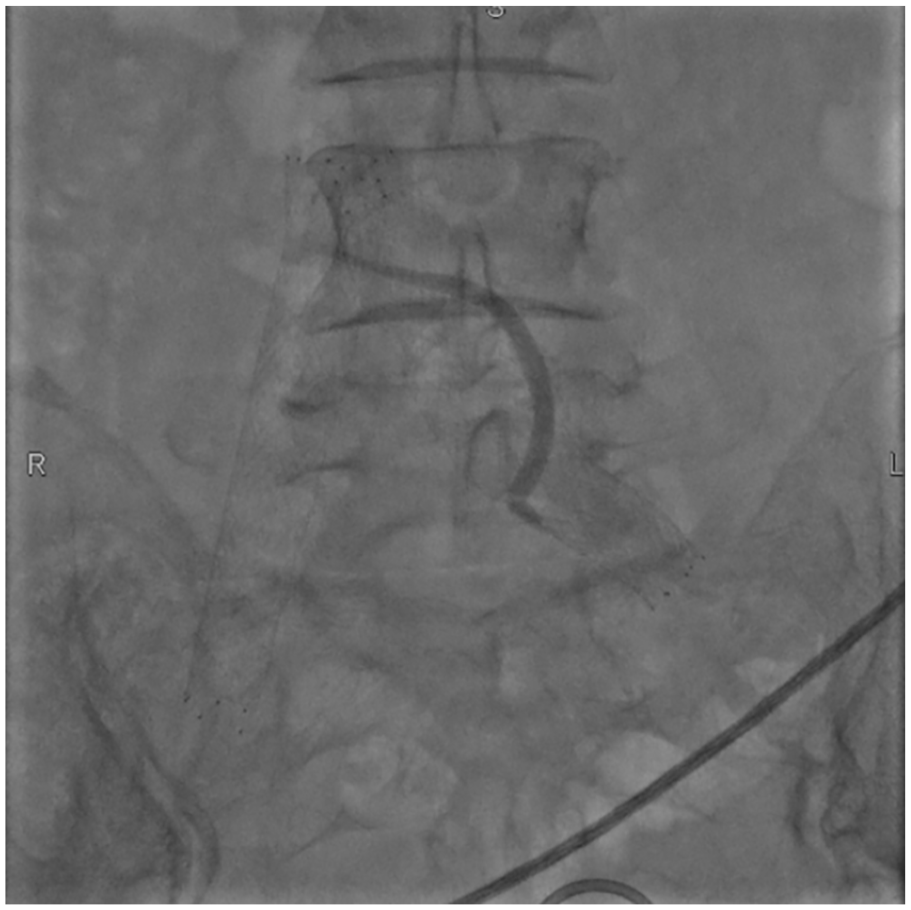
The bone cement was caught in the bifurcation of the common iliac vein and cannot be pulled out from either side of the iliac vein. Stents were placed on the iliac veins on both sides to fix the bone cement in place.
At the 1-year follow-up, the patient did not have any complaints, postoperative CTPA showed no obvious manifestations of pulmonary embolism (Figure 4), and angiography showed that the bone cement was fixed in place and that the iliac veins were normal (Figure 5).

In the 1-year follow-up, CTPA showed no obvious manifestations of pulmonary embolism.

The 1-year follow-up, angiography showed that the bone cement was fixed in place and that the iliac veins were normal.
Discussion
Currently, there are no treatment guidelines for bone cement pulmonary embolism. The treatment of bone cement pulmonary embolism mainly depends on symptoms, the location and size of the embolus, and imaging features. 3 Some scholars suggest that open surgical removal may be the preferred treatment for symptomatic intracardiac cement embolism. 9 However, open surgery requires experienced surgeons to perform, and not all hospitals can complete it.
Endovascular treatment is a minimally invasive surgical method with a short recovery time. In recent years, with the further maturity of endovascular technology, some patients with bone cement embolization have received interventional treatment and achieved certain results. 10
If the patient’s bone cement does not cause vascular wall penetration, we can consider endovascular treatment. Soft and gentle operation is required during the surgery. Although the bone cement is relatively sharp, if the force of capture is too large, the bone cement may break, leading to increased difficulty and risk of surgery. For smaller emboli, we can directly remove them from the body through an endovascular procedure. But if the embolus is large, it cannot be removed. Some literature reports suggest that bone cement emboli can be pulled from the heart or pulmonary artery to the inferior vena cava or femoral vein through endovascular treatment, and then removed through open surgery to minimize the complications of open surgery to the greatest extent possible.11,12
The main purpose of endovascular treatment is to reduce the serious consequences caused by bone cement at the embolic site, and it is not necessary to remove bone cement from the body. Of course, it is best to be able to remove it. If the morphology and vascular conditions of the bone cement are poor, removal of the bone cement from the target organ and fixing it in a safe blood vessel can be considered, as in this case.
Conclusion
We report a case of endovascular treatment of a bone cement embolism after percutaneous vertebroplasty. Due to its large size and curvature, the bone cement could not be removed from the body, so stent grafts were used to fix the bone cement at the level of the iliac vein, which achieved good follow-up results.
Footnotes
Acknowledgements
None.
Author contributions
X.L., Y.S., W.J.Z., X.W. provided patient care, monitored the patient’s vital signs, provided treatment, and abstracted laboratory and clinical data; X.L. and X.W. performed a regular follow-up of the patient; X.L. and X.W. contributed to the writing of the manuscript; All authors reviewed and approved the final manuscript and issued final approval for the version to be submitted.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by the National Natural Science Foundation of China (No. 82300558).
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.