
Abstract
Primary hyperparathyroidism (PHPT), an endocrine disorder most commonly caused by parathyroid adenoma (PTA), manifests with a diverse array of symptoms, reflecting the multisystem impact of parathyroid hormone: nephrolithiasis, peptic ulcer disease, psychiatric disorders, muscle weakness, constipation, polyuria, pancreatitis, myalgia, and arthralgia. Rarely do these PTA attain a significant size. PHPT is usually diagnosed through biochemical tests, and radiological imaging characterizes the adenoma. Serum 25-hydroxyvitamin D levels are useful in explaining the large adenoma size. Here, we report a rare case of a 60-year-old female from Morocco who presented with marked dyspnea due to a giant PTA.
Introduction
Primary hyperparathyroidism (PHPT) is a common endocrine disorder caused by a parathyroid adenoma (PTA) in 80%–85% of cases. 1 Most of these adenomas are small, weighing around 70 mg to 1 g, except for some rare cases of giant PTA (GPTA), which are defined as weighing over 3.5 g. Clinical symptoms, such as renal colic, peptic ulcer disease, psychiatric disorders, muscle weakness, constipation, polyuria, pancreatitis, myalgia, and arthralgia with bone diseases, often prompt physicians to perform calcium and parathyroid hormone (PTH) measurements, which typically indicate hyperparathyroidism. A 25-hydroxyvitamin D (25-OHD) level should also be checked for vitamin D deficiency, which, in the rare cases of giant adenomas, may explain the large size of the adenoma and unusual respiratory symptoms. Imaging techniques, such as ultrasound and scintigraphy coupled with computed tomography (CT), are used to locate the adenoma, assess its size, and determine its relationship with surrounding tissue.
We report the Moroccan experience with a case of a GPTA presenting with dyspnea.
Case report
A 60-year-old Moroccan female without significant medical or surgical history presented with a marked dyspnea and a left lower neck swelling moving on swallowing, gradually increasing in volume over the past 3 years. Given these clinical signs, an ultrasound of her neck (Figure 1) was first requested. It revealed a retro thyroid tissue formation posterior to the left thyroid lobe, oblong with a fusiform proximal tip, relatively hypoechoic and vascularized in US DOPPLER. The patient underwent a cervical CT scan (Figure 2) for a better characterization of the tumor, which showed a tissular mass posterior to the left thyroid lobe, extending from the vertebral body C6 to D3, oblong, well limited, with regular contours, hypodense homogeneously enhanced after injection of contrast agent, measuring 14 × 11 × 46 mm.
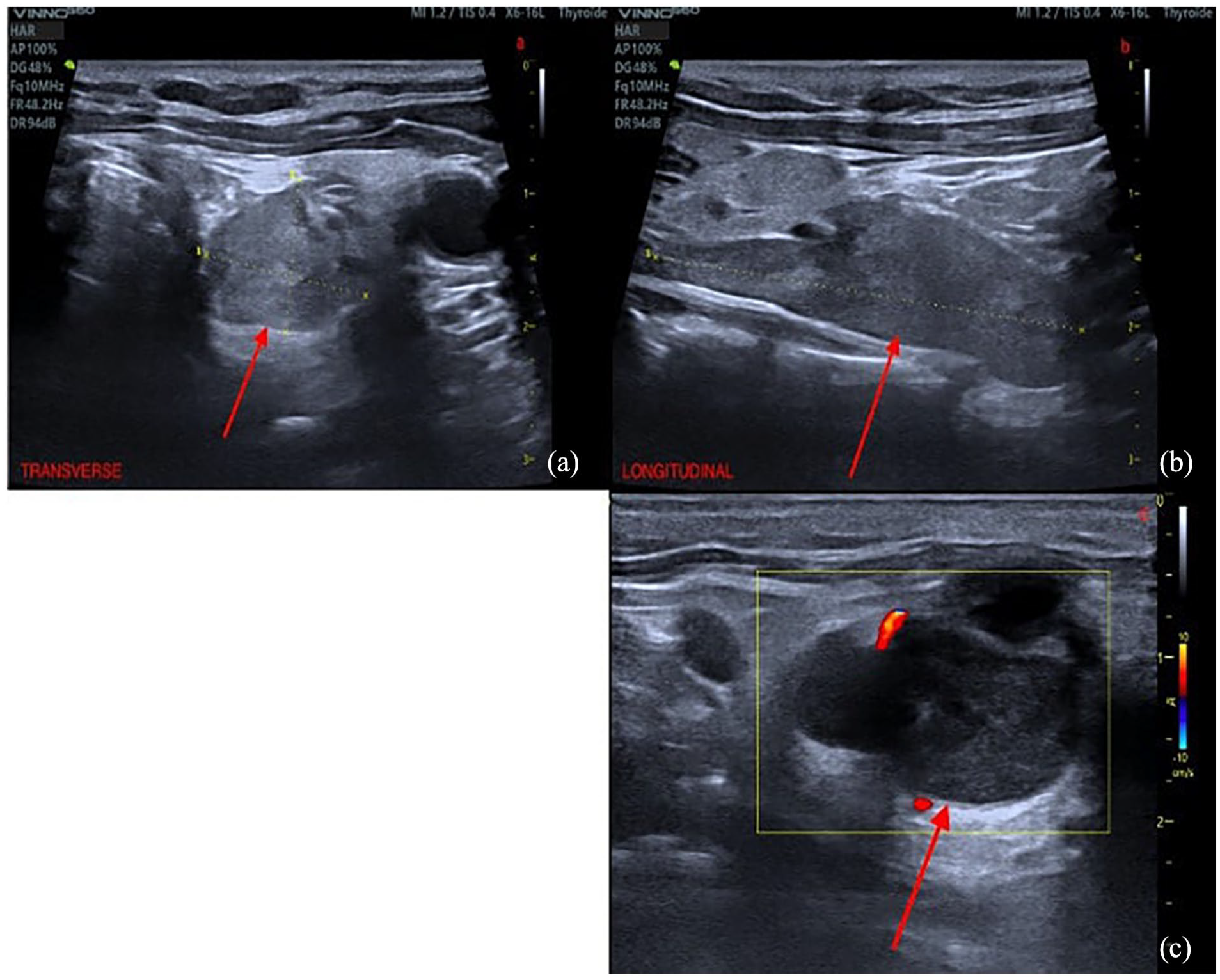
Ultrasound of giant parathyroid adenoma. Transverse view (a), longitudinal view (b), transverse view with Doppler (c), showing a retro thyroid formation (red arrow), oblong, relatively hypoechoic and vascularized (c).

Cervical CT scan without (a) and with contrast medium ((b) axial, (c) sagittal, (d) coronal) showing an homogeneous soft tissue process at the left tracheoesophageal groove, posterior to the left thyroid lobe, measuring : 14 × 11 × 46 mm.
Biochemical data indicated PHPT, with elevated serum PTH (144 pg/ml) and calcium (12 mg/dl) levels. A vitamin D deficiency was identified with a low level of 25-OHD (19.4 pg/ml). The assessment of hypercalcemia’s impact revealed no abnormalities in cardiac, renal (serum creatinine level: 0.7 mg/dl), or digestive systems.
The parathyroid sestamibi scintigraphy (Figure 3) reported a large focus of 99mTc-sestamibi scintigraphy (MIBI) intense uptake on earlier and delayed images, extending from the middle and lower 2/3 of the left thyroid gland to the low cervical level, contrasting with a complete thyroid washout at the end of the examination.

Parathyroid sestamibi scintigraphy showing a large focus of MIBI-Tc 99m intense uptake on earlier (a) and delayed images (b), extending from the middle and lower 2/3 of the left thyroid gland to the low cervical level, contrasting with a complete thyroid washout at the end of the examination.
These findings were highly suggestive of a PTA, and the surgical team opted for an excision of the left lower retrothyroid mass, which measured approximately 5 cm in length and 32 g in weight. Vitamin D supplementation was started. Following surgery, serum calcium and PTH normalized, and the pathological examination of the specimen (Figure 4) was consistent with PTA.

Histopathological examination confirmed the final diagnosis of parathyroid adenoma.
Discussion
PHPT is classically defined by the excessive secretion of PTH, leading to an elevated serum calcium concentration. This is achieved by increased calcium absorption from the intestines and bones, coupled with decreased kidney clearance. 2 While PHPT can occur at any age, it is more prevalent in females during the fifth and sixth decades of life. 5
PTAs are the most common tumors associated with PHPT, typically weighing less than 1 g. In rare cases, when their weight exceeds 3.5 g, they are termed GPTAs. 4 The underlying reasons for this variation in size remain unclear, whether attributed to late disease detection, vitamin D deficiency, or the hyperproliferative nature of the adenoma cells.3,8,9
Patients diagnosed with PHPT often present with a range of non-specific symptoms, such as fatigue, irritability, and cognitive impairment. Additionally, the condition is commonly associated with manifestations of hypercalcemia, such as depression, bone pain, weakness, and renal colic (nephrolithiasis). Furthermore, dyspnea may develop unusually in patients with parathyroid disease due to direct pressure on relevant organs from a large adenoma and ectopic tissue.11,13 This dyspnea can be correlated with low levels of vitamin D, which is involved in several respiratory diseases, notably asthma, viral or tuberculosis respiratory infections, chronic obstructive pulmonary disease, chronic rhinitis, and the elastic disruption of the pulmonary artery wall, which becomes stiff.8,12
Regarding the physical examination, a significant portion of GPTAs exhibited both visible and palpable masses. The substantial size of these masses is a factor that might lead a clinician to consider thyroid disease even before reviewing laboratory results, given that palpable nodules are more frequently associated with the thyroid. 4
The diagnostic investigation of PHPT commences with assessing serum calcium and PTH levels. The hallmark features of PHPT include hypercalcemia and elevated PTH. 6 However, some studies proved that larger parathyroid adenomas are less efficient in secreting PTH compared with light adenomas. 9 Serum 25-OHD can be used to detect vitamin D deficiency, which stimulates parathyroid hyperplasia and explains some symptoms.6,9–13
Localization of the parathyroid adenoma is pivotal for guiding appropriate management. The primary imaging methods employed for this purpose are neck ultrasound and MIBI scan.
However, neck ultrasound has limitations, particularly in cases where the parathyroid adenoma is ectopic. In such instances, a neck ultrasound may not reveal any findings.
For neck GPTA, the most effective approach involves a combination of a MIBI scan and neck ultrasound. This combined method facilitates accurate localization, enabling guided neck exploration during subsequent interventions.
The predictive accuracy of ultrasound alone in determining GPTA location is approximately 79%. However, when ultrasound is combined with MIBI and CT, the overall localization accuracy increases to 82%. 7
In summary, a comprehensive diagnostic strategy for GPTA in PHPT involves serum calcium and PTH assessment, followed by a combination of imaging techniques, with a particular emphasis on the joint use of neck ultrasound and MIBI scan for optimal localization accuracy. 4
The conclusive diagnosis is achieved through surgical intervention, followed by histopathological evaluation. 11
Conclusion
Diagnosing parathyroid adenomas poses challenges, and among the diverse presentations, GPTAs represent a rare entity, which is not frequently revealed with respiratory symptoms such as dyspnea, and should be kept in mind during the diagnostic process.
Footnotes
Acknowledgements
I would like to express my gratitude to my professors and all the colleagues who participated in the completion of this work.
Author contributions
K.S.: conception of the work, design of the work, and acquisition of data. K.M. and C.F.: acquisition of data. F.C. and H.E.: contributed to acquisition, analysis, or interpretation. N.C., M.F., N.E.-C.E.K., M.J., and F.T.: revising the work critically for important intellectual content.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.