
Abstract
Introduction:
Over two-thirds of Canadians are deficient in vitamin D. Clinical overlap can compound diagnosis of depression in vitamin D deficient individuals. Citing high costs, the Ministry of Health has restricted routine vitamin D screening and hence is not feasible.
Objectives:
The current case series is an attempt to recognise the clinical overlap between depression and vitamin D deficiency in order to avoid unnecessary antidepressant prescriptions and to demonstrate the role of collaborative care in such patients.
Method:
After appropriate ethics approval 62 patients from an outpatient clinic were screened for the diagnosis of treatment resistant depression. Those who had predominant somatic complaints were further screened for organic factors and those with inadequate vitamin D levels were referred to family physicians for supplementation with vitamin D.
Results:
More than 50% were detected deficient in vitamin D after our evaluation. They showed subjective improvement with vitamin D supplements. No modification of antidepressants was needed.
Conclusion:
Vitamin D deficiency should be suspected in depressed patients with prominent somatic symptoms and their treatment resistance should be reconsidered to avoid unnecessary exposure to mood stabilisers. Collaborating with primary care is advocated.
Limitation:
Co-prescription of an antidepressant is a confounder in our case series, and we propose more organised studies with objective rating scales.
Introduction
Over two-thirds of Canadians are deficient in vitamin D. 1 The implications of this in terms of bone health are increasingly understood, yet its impact on other health areas, particularly mental health, is unclear. Vitamin D deficiency has also been implicated in autism, schizophrenia, Alzheimer’s dementia, Parkinson’s disease and multiple sclerosis. 2 Hippocampus is one of the brain regions that is implicated in depression. It also has vitamin D receptors. This may explain the clinical overlap between depression and vitamin D deficiency (Figure 1). Role of vitamin D in treating depression is controversial. Robust evidence linking the two is absent. In the last 10 years, majority studies have failed to conclude an association between depression and low vitamin D levels. 3 A systematic review and meta-analysis of seven randomised controlled trials has noted the unequivocal effect of vitamin D supplementation as an antidepressant. 4 While the recent literature has explained the action of vitamin D in the brain, much is still unknown concerning how vitamin D relates to mood. 5 The few epidemiological studies of vitamin D and depression have produced inconsistent results and generally have had substantial methodological limitations. 6 In yet another systematic review and meta-analysis, 1 case–control study, 10 cross-sectional studies and 3 cohort studies were analysed. The findings were consistent with the hypothesis that low vitamin D concentration is associated with depression. However, it reiterated the need for robust randomised controlled trials to confirm the causal relation between deficiency of vitamin D and depression. 7 Our case series highlights the importance of suspecting low vitamin D levels in so-called treatment-resistant cases. Collaboration with primary care physicians is essential to provide holistic and continuing care. Citing high costs, the Ministry of Health 8 has restricted routine vitamin D screening. Therefore, a high index of clinical suspicion is advised. 9

Clinical overlap between vitamin D deficiency and depressive episode.
Case series
This case series was conducted in the outpatient setting of a University hospital. Approval was granted by Health Sciences Research Ethics Board, Queen’s University. The need for patient consent was waived as only patient documents were inspected. Clinic records of all adult psychiatry patients (18–65 years, n = 62) assessed by the primary author in 2012 were reviewed. When screened for a diagnosis of depressive episode as defined by Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM IV), 28 cases were identified (Figure 2). Among them, 11 patients were labelled by family physicians as ‘treatment resistant’ as they had failed to respond to at least three different antidepressants in therapeutic doses prescribed for optimal duration for their current episode. None of them had a previous history of mood disorder. The possibility of seasonal affective disorder was ruled out keeping in mind its association with vitamin D deficiency. However, none of the patients had been screened for any organic factors that could lead to a depressive picture, thereby challenging their treatment resistance. All patients were within the age range of 31–40 years. Five of them were male. The rest were female. The mean duration of the depressive episode was 7.7 months. Symptom exploration on clinical interview using the DSM IV criteria revealed predominance of somatic features such as fatigue, unrefreshing sleep and somatic pains as opposed to pervasively low mood. Their ‘treatment resistance’ was re-examined. Common possible contributory factors such as anaemia, thyroid dysfunction, sleep apnoea and vitamin B12 deficiency were ruled out. Bearing in mind the ministry recommendations, serum vitamin D levels were judiciously advised in these 11 patients. Six patients had insufficient levels of 25-OH vitamin D, the mean level being 31 nmol/L. The desirable physiologic range is 75–250 nmol/L (Table 1). 10 However, these ranges are not universally uniform. At our recommendation, family physicians supplemented ongoing antidepressants with vitamin D. One received intramuscular 5000 IU of vitamin D3 on a weekly basis. The rest were prescribed daily oral vitamin D3 supplements (Table 2). 11 Patients were followed up at 6- to 8-week intervals for at least 4 months. They reported subjective improvement in their fatigue when their ongoing antidepressants were supplemented with vitamin D. These were recorded by the two authors and reported to the family physician. Of those, one patient sustained the improvement for at least 2 months after discontinuing the antidepressant. Alteration of antidepressants was not warranted in any. Neither patient needed any additional antidepressant or mood stabiliser. The family physicians played an immense role in monitoring and treating vitamin D deficiency at our recommendation.

Flow chart for case series.
Laboratory correlates of vitamin D (LifeLabs). 10
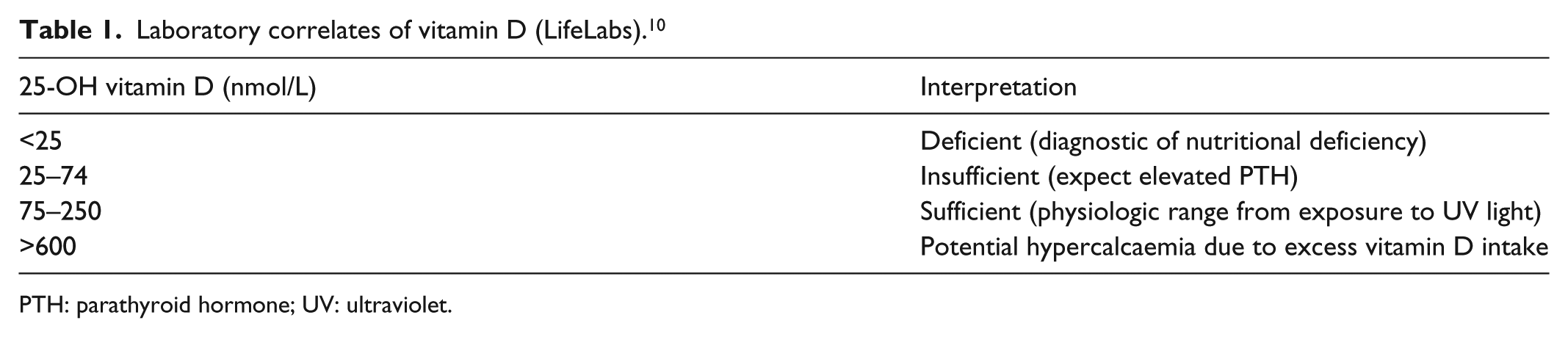
PTH: parathyroid hormone; UV: ultraviolet.
Vitamin D: serum levels and doses administered (Ped. Child Health). 11

IM: intramuscular; PO: per os.
Mean serum vitamin D level = 31 nmol/L; standard deviation (SD) = 8.25.
Discussion
More than 50% patients with suspected diagnosis of treatment-resistant depression had inadequate vitamin D levels. It is worthwhile noting that all of them had described fatigue and somatic pains more frequently than pervasive low mood. Once vitamin D was prescribed, they reported subjective improvement in their clinical features especially fatigue in nearly 6 weeks. None of them needed any alternative antidepressants or mood stabilisers. Owing to regulations by Ministry of health, serum vitamin D levels could not be repeated post-supplemenation. 8 Hence the possibility of a placebo-effect cannot be denied. The relationship between vitamin D and depression is intriguing in terms of cause and effect. 6 Vitamin D deficiency may lead to a depressive picture. On the other hand, a depressed individual may be housebound due to low motivation. This in turn will affect the synthesis of vitamin D due to lack of exposure to the sun. Poor diet due to lack of appetite can also contribute to the deficiency. 12 A small sample and the retrospective study design limit the generalisability of our observations. We also did not study the role of ethnicity which can influence serum vitamin D levels as demonstrated by a recent study of traumatic cord injury patients. Despite the same degree of immobilisation and sun exposure, lower vitamin D levels were observed in African Americans relative to the Whites. 13 However, yet another study has revealed an association between low vitamin D levels and depression, largely independent of several lifestyle and health factors. 14 Owing to ethical reasons, the prescribed antidepressant was continued when vitamin D was supplemented. Objective rating scales could not be used as this was a retrospective observational study in a clinical setting. Prospective studies with use of such rating scales can help counter this confounder to some extent.
Conclusion
Our case series suggests that low vitamin D levels should be suspected in ‘depressed’ patients with predominant somatic symptoms before labelling them as treatment resistant. Collaborative care involving family physicians avoids undue prescription of mood stabilisers. More randomised controlled trials are recommended to conclusively prove the causative role of vitamin D deficiency in depression. 4 Studying the prophylactic role of vitamin D in preventing depression may eliminate the confounding effect of the antidepressant observed in our series. The purpose of this case series is not to recommend vitamin D as the therapy for treatment-resistant depression, but to question the treatment resistance, reconsider the aetiological role of organic factors and treat accordingly.
Limitations
Objectivity to the case series may be limited by the absence of structured interview questionnaires and lack of repeat serum vitamin D levels post-supplementation.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.