
Abstract
Traditionally reflecting critical stenosis of the proximal left anterior descending (LAD) artery, Wellens’ syndrome (WS) is an electrocardiogram (ECG) pattern of biphasic or deeply inverted T waves in leads V2 and V3. This critical stenosis can progress to an extensive anterior myocardial infarction (MI) if early and appropriate management is not received promptly. The diagnosis of severe stenosis of the LAD coronary artery can be made by using electrocardiographic changes in Wellens’ syndrome. Due to the significant area that the LAD vascularizes, patients who exhibit symptoms and test results suggestive of this syndrome should be referred right away for an angiographic exploration in order to confirm the diagnosis and guide treatment. We report a case of a 71-year-old male admitted to our department for acute chest pain. His ECG showed Wellens’ syndrome type 2 during both chest pain and pain free with slightly elevated troponin. His TIMI score was 3 and the GRACE score was 136. Critical stenosis of the LAD coronary artery was found in the coronary angiography, which required a drug-eluting stent. The patient was discharged asymptomatic from medical therapy. The diagnosis was established on the basis of the patient’s interview, ECG analysis, and coronary angiography.
Introduction
Forty-two years ago, Wellens and his colleagues documented an ECG pattern that was observed in patients admitted for unstable angina. This pattern included T-wave changes in the precordial leads, which were highly associated with severe stenosis of the proximal left anterior descending (LAD) artery. This condition was called Wellens’ syndrome (WS). 1 Clinical and electrocardiographic criteria for WS are symmetric and deeply inverted T waves, in leads V2 and V3, occasionally in leads V1, V4, V5 and V6; or biphasic T wave inleads V2 and V3; plus isoelectric or minimally elevated (<1 mm) ST segment, no precordial Q waves; a history of angina; a pattern is that often present in pain-free state, normal or slightly elevated cardiac serum markers.2,3 Non-ST-segment elevation myocardial infarction (NSTEMI) is rising among Wellens’ syndrome patients, while the incidence of unstable angina is decreasing. 4 Early detection and treatment are of the utmost importance since these patterns frequently indicate a preinfarction state that can result in a large anterior wall myocardial infarction. Patients frequently present pain-free with only T-wave abnormalities and a normal or modest increase in cardiac biomarkers, a combination that can be misleadingly reassuring, so it is easy to overlook this diagnosis. 5 In this article, we report a case of acute chest pain in a 71-year-old patient with age and male sex as cardiovascular risk factors admitted to our department for WS. Upon admission to the catheterization room, coronary angiography revealed a very tight lesion of the proximal LAD with a heavy burden of thrombus managed by a successful direct stenting. This case emphasizes the value of early revascularization when WS is identified and the role of the ECG in the diagnostic orientation. Our article was written according to the CAse REports (CARE) guidelines. 6
Case presentation
A 71-year-old male with age and sex as cardiovascular risk factors and no previously known diseases complained of episodes of oppressive chest pain with irradiation to his back, which appeared initially during effort but progressed to resting pain with increasing frequency and intensity. The patient did not complain of palpitation or episodes of syncope. On presentation to our department, the patient was hemodynamically stable but still in pain, with a blood pressure of 130/80 mm Hg, a heart rate of 88 beats/min, and an oxygen saturation of 98%. Cardiac troponin was at 54 pg/ml (normal value <17 pg/ml); the metabolic panel and complete blood count were unremarkable. ECG on admission during chest pain showed negative T waves in V1–V4 suggestive of type 2 Wellens’ syndrome (Figure 1). ECG repeated during chest pain-free period showed the same findings. His TIMI (Thrombolysis in Myocardial Infarction) score 7 was 3 and the GRACE (Global Registry of Acute Coronary Events) score 8 was 136. Transthoracic echocardiography revealed no abnormalities with a preserved ejection fraction (EF: 70%). Therefore, it was decided to refer the patient to coronary angiography, which revealed a critical lesion in the proximal portion of the LAD with distal TIMI 3 flow that required the placement of one drug-eluting stent (Figure 2). The patient was discharged stable with optimal medical treatment. He was seen by his physician after 6 weeks and reported no particular symptoms.
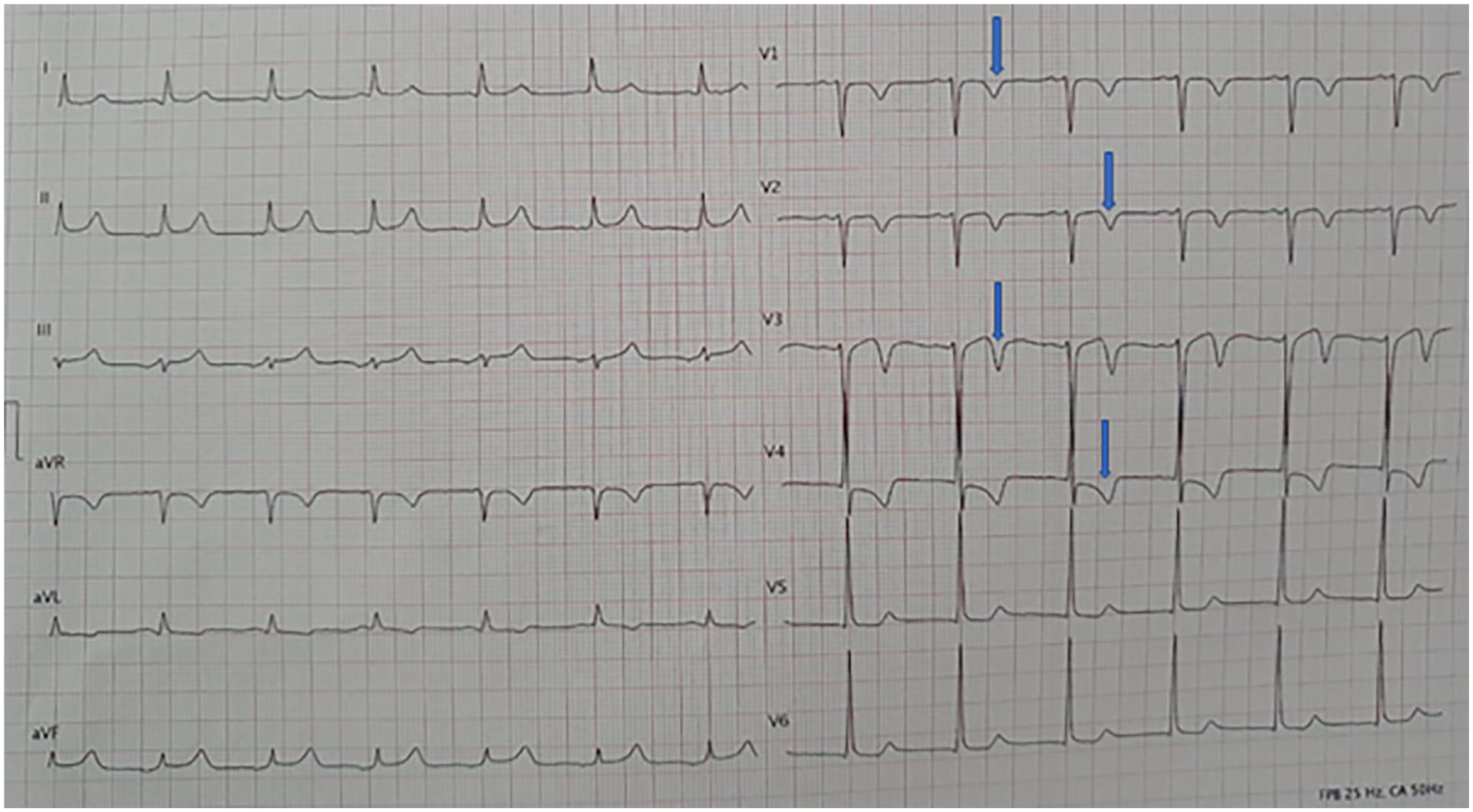
ECG on admission showing deeply inverted T-waves in V1–V4 suggestive of type 2 Wellens’ syndrome (blue arrows).

(a, b) Coronary angiography showing critical stenosis of the proximal LAD artery (blue arrows). (c) Poststent angiography with restoration of good flow in the LAD.
Discussion
With the precise aetiology being coronary artery disorders such as atherosclerotic plaque, coronary artery vasospasm, hypoxia, and increased cardiac demand, the incidence of WS ranges from 10% to 15% of all cases of acute coronary syndrome (ACS). Types A and B are described (1 and 2, respectively). Type 1 is characterised by biphasic T waves that are seen in V2 and V3. It represents 24% of all situations; it is less prevalent, more specific, and less recognized. In 76% of cases, Type 2 is the most prevalent and least specific. It is identified by symmetrical, deeply inverted T waves in V2 and V4. 9 Nevertheless, recent studies have reported a lower prevalence of WS in patients admitted for ACS.10,11 In a recent cross‑sectional study, 12 unlike previous studies, the type 1 was more frequent (55.6%). But despite being highly selective, this study was conducted in a single cardiac centre thereby limiting the number of patients who can be enrolled. The development of a type 1 ECG pattern is suggestive of a critical stenosis of the proximal LAD, whereas type 2 seems to be more associated with a lesion of the mid-LAD. 13 Our patient had type 2, but with severe stenosis of the proximal LAD and a heavy burden of thrombosis. There are three sections to the LAD. The first perforating septal branch marks the distal end of the proximal segment, which starts at the LAD’s origin. From the proximal segment’s end to the second diagonal branch lies the middle segment. Following the middle section, the distal portion comes to an end following the cardiac apex. 14 Proximal blockage of the LAD can jeopardize a significant portion of the myocardium due to the vast surface area of tissue it supplies, as is the case in patients with Wellens’ syndrome. 14 Critical blockage of the proximal LAD is the hallmark of Wellens’ syndrome, while the cause of the lesion may also affect the medial section of the LAD. 15 Furthermore, there is a high specificity for the presence of LAD obstruction in the Wellens ECG patterns. The presence of either ECG pattern in leads V2 and V3 has a 96% specificity for a LAD lesion, whereas the type 1 and type 2 patterns have specificities of 99% and 97%, respectively. 10 Specificity increases in the type 2 pattern in a correlation to the T-wave inversion’s depth. Similarly, each pattern’s positive and negative predictive values for LAD occlusion are very low; thus, when assessing patients, physicians should use their best sense. 10 Premature coronary heart disease in the family, type II diabetes mellitus, metabolic syndrome, hypertension, smoking, hyperlipidaemia, work stress, advanced age (55 ± 9 years), HIV-related cases, and early coronary disease history are the risk factors for WS. 16 Our patient had none of these except advanced age; this shows the place of the ECG in diagnostic orientation. Although clinical signs and ECG criteria of WS are in most cases related to an occlusion of the LAD, certain conditions such as digitalis use, bundle branch blocks, Takotsubo syndrome, left ventricular hypertrophy, cocaine-induced vasospasm, aortic dissection pulmonary embolism, pneumothorax, cerebral haemorrhage, myocardial bridging can also mimic WS.17,18 These conditions, called pseudo-Wellens syndrome, are rare entities characterized by the presence of ECG changes of WS, but without the stenosis of the LAD. 18 Similarly, cardiac memory phenomenon is also one of the causes of deep inverted T waves, which can be confused with WS and ACS. These deep inverted T waves usually occur after prolonged pacing, ventricular pre-excitation, intermittent left bundle branch block, wide QRS rhythms and ventricular tachycardia. The abnormal ventricular activation pattern leads to electrical remodelling of the myocardial cells, which manifest as changes in the T wave vector and polarity during conversion to the native rhythm; thus, remembering the direction of the QRS complex. 19 The distinctive characteristic of WS is that the ECG abnormalities frequently manifest during the pain-free phase, which usually lasts for less than 15–20 min following the angina episode; consequently, WS is associated with a slight or non-existent release of troponin.3,13 These characteristics make patients with WS difficult to identify, leading to errors in diagnosis and inadequate risk stratification, so the ability to recognize these patterns is extremely important since ECG changes can sometimes be subtle. Like in our case, some authors have also reported the presence of electrical signs of WS during the pain phase. Park et al. 20 reported the case of a 45-year-old male patient admitted for acute chest pain with a type 1 Wellens’ syndrome, while the patient was still suffering, the evolution was marked by the occurrence of NSTEMI with a type 2 pattern 12 h later. Our patient had electrical signs during the painful period as well as in the pain-free phase but did not progress to a NSTEMI because he was taken directly to the catheterisation room where he received a drug-eluting stent. While the exact cause of the ECG abnormalities is unknown, it has been suggested that intermittent or unstable blood flow in the anterior descending coronary artery with critical blockage may cause local oedema or lightheadedness. 9 The presence of Wellens’ syndrome is not definitely associated with a poor prognosis in patients suffering from NSTE-ACS. Nevertheless, it has been pointed out that age ⩾65 years, diabetes, NSTEMI, eGFR <60 ml/min and left main disease are associated with poor outcomes like cardiac death. 11 As WS is the pre-infarct stage of ACS, diagnosing it early on may be lifesaving. T-wave alterations in WS are typically seen in patients who are asymptomatic. These patients may respond well to medical management initially, but with conservative therapy, they eventually have poor outcomes, such as left ventricular dysfunction, anterior myocardial infarction, or sudden cardiac death; hence, the importance of a revascularization strategy. Cardiac catheterization should be done in an emergency situation, and patients who are exhibiting symptoms should be closely monitored in the intensive care unit. For WS patients with severe LAD stenosis, a stress test is not recommended because it can cause an acute myocardial infarction and sudden death.9,16
Conclusions
WS is a pre-infarct condition with significant stenosis of the proximal LAD artery characterized by inverted or biphasic T waves in precordial leads. In this case, we have demonstrated the possibility of an atypical presentation even in elderly patients with no modifiable cardiovascular risk factors. A coronary evaluation is necessary for definitive management, even though medical management can be effective initially. Physicians who identify this ECG pattern should consider their patients at high risk and advocate for definitive therapy with coronary angiography and revascularization.
Footnotes
Acknowledgements
Non-applicable.
Author contributions
T.H. Diallo: study concept, data collection, data analysis, writing the paper; R. Djafarou Boubacar: data collection, data analysis, writing the paper; I.S. Azday: data collection, data analysis; R. Fellat: supervision and data validation; N. Fellat: supervision and data validation.
Availability of data and materials
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient for the anonymized publication of this case report
Research registration
Not applicable.
Provenance and peer review
Not commissioned, externally peer-reviewed.