
Abstract
Purtscher’s retinopathy is an occlusive micro-vasculopathy causing sudden onset visual loss in trauma. Similar retinal appearance is observed as a rare complication of acute pancreatitis which is identified as Purtscher-like retinopathy (PulR). We report the case of a 15-year-old girl diagnosed to have acute on chronic pancreatitis who noticed a sudden onset loss of vision in the left eye and was found to have significantly diminished visual acuity. A dilated fundoscopic examination demonstrated pathognomonic Purtscher flecken, multiple retinal haemorrhages, cotton wool spots and macular oedema. A clinical diagnosis of PulR was made in the setting of acute on chronic pancreatitis. Optical coherence tomography was used to support the diagnosis and to monitor response to therapy. Given the variable prognosis with no evidence-based therapies available, she had a subjective improvement in visual acuity with administration of intravitreal steroids and observation with management of the acute episode of pancreatitis. Knowledge and awareness of this rare condition will enable its early detection and the search for newer therapies.
Introduction
Purtscher-like retinopathy (PulR) is a rare complication of acute pancreatitis. Literature regarding management of acute or acute on chronic pancreatitis hardly recognize this complication.1,2 Purtscher’s retinopathy (PuR) is an occlusive micro-vasculopathy that causes sudden onset vision loss of varying severity. It was first described by Otmar Purtscher in 1910 in a patient with head trauma. Subsequently, it was found to be associated with indirect non-ocular traumatic conditions and various non-traumatic systemic conditions.3,4 When associated with non-traumatic clinical entities, such as acute pancreatitis, pancreatic adenocarcinoma, fat embolism syndrome, chronic kidney disease and autoimmune conditions, it is termed as PulR.5,6
The clinical presentation includes painless, unilateral, or bilateral, and subacute loss of vision with a causal link to a traumatic or a non-traumatic event. Fundus will show cotton wool spots, retinal haemorrhages and pathognomonic Purtscher flecken typically confined to the peripapillary and macular region sparing the retinal periphery (Figure 1). 3 We describe a case of PulR, a rarely diagnosed complication of idiopathic acute on chronic pancreatitis.
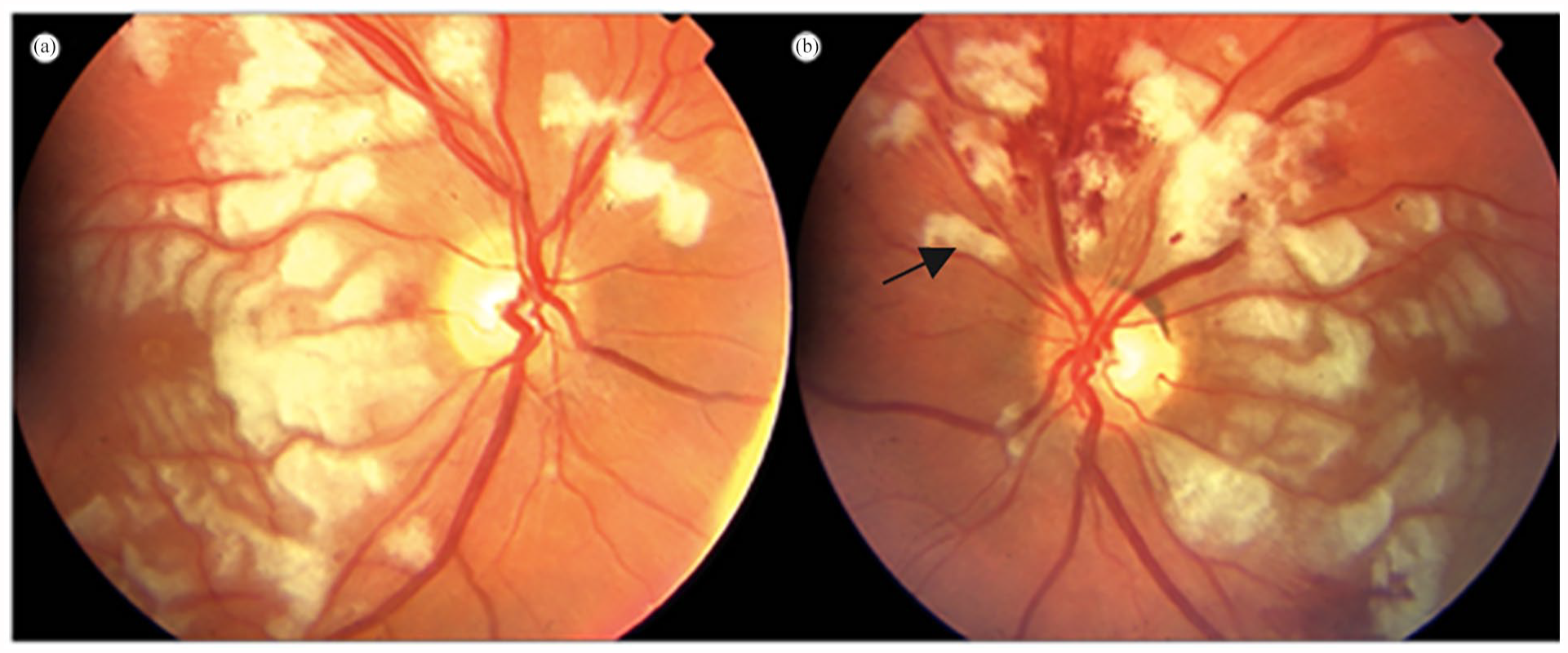
Typical fundoscopic appearance of Purtscher’s retinopathy showing pathognomonic Purtscher flecken, cotton wool spots and retinal haemorrhages. The black arrow denotes Purtscher flecken found between retinal vessels and well demarcated than cotton wool spots.
Case presentation
A 15-year-old girl with history of chronic pancreatitis presented with an episode of acute exacerbation. During last 6-month period, she had multiple episodes of acute or chronic pancreatitis causing severe epigastric pain which required multiple hospital admissions.
During the index admission, she developed high spiking fever and was found to have an infected walled off pancreatic necrosis using contrast enhanced computer tomography (CECT) and endoscopic ultrasound. Her C-reactive protein level was 600 mg/l. She was started on broad spectrum intravenous antibiotics. After a prolonged course of antibiotics of 14 days, her fever settled and the inflammatory markers came down.
Three days after her fever was settled, she complained of loss of vision in her left eye. She denied any eye pain, floaters or flashes. The patient did not have a prior history of any visual pathology or a refractive error. Visual acuity of her left eye was 1/60 and the right eye had a normal visual acuity of 6/6. An urgent ophthalmology referral facilitated a fundoscopic examination with fundal photography, measurement of intra-ocular pressure and optical coherence tomography (OCT). The clinical and investigation findings were as shown in Table 1.
Clinical and investigation findings.

OCT, optical coherence tomography.
Fundal images showed blurred disc margins and macular oedema with exudates. Multiple haemorrhages were seen in the retinal nerve fibre layer dispersed with cotton wool spots in between, predominantly over the peripapillary and macular regions. Pathognomonic Purtscher flecken, which are well-demarcated areas of retinal whitening between the retinal vessels were also seen. Macular thickness as measured with OCT was more than 700 µm which confirmed the presence of macular oedema.
An urgent vitreoretinal opinion was obtained and diagnosis of PulR was confirmed. She was treated with urgent intravitreal Triamcinolone 1 mg and with intravitreal Bevacizumab 0.05 mg (anti-Vascular Endothelial Growth Factor) to the left eye as separate intravitreal injections given under topical anaesthesia approximately 48 h following noticing the loss of vision.
One week post-injection her left eye visual acuity had worsened to hand movements even though the fundal appearance and the OCT showed a slight improvement. Figure 2 shows the fundal photo after 1 week showing retinal haemorrhages and cotton wool spots. Purtscher flecken seen at the diagnosis were not seen. In post 1 week OCT (Figure 3), there was improvement in macular oedema with disrupted inner segment/outer segment (IS/OS) junction.

Fundal photo after 1 week showing disappearance of Purstscher flecken. Retinal haemorrhages and cotton wool spots are still seen.

OCT after 1 week showing improved macular oedema and disrupted IS/OS junction.
However, by 3 weeks post-injection her left eye visual acuity improved slightly up to 2/60 with a clinically improved fundal appearance (Figure 4) showing improvement in retinal haemorrhages and cotton wool spots and with the OCT (Figure 5) showing settled macular oedema with poor prognostic features such as disrupted IS/OS junction and macular atrophy. Her right eye remained unaffected.

Fundal photo after 3 weeks showing improvement in retinal haemorrhages and cotton wool spots.

OCT after 3 weeks showing settled macular oedema. But poor prognostic features like disrupted IS/OS junction and macular atrophy are evident.
Visual-evoked potentials (VEPs) of the left eye showed severe axonal loss.
Discussion
Although first description of PuR is in 1910 by Otmar Purtscher, its association with acute pancreatitis was not recognized until 1975.2,4 Complement activation leading to embolization of clumped granulocytes occluding the precapillary arterioles in the retina is proposed as the main pathophysiological mechanism causing this condition. In acute pancreatitis, elevations of serum lipase leading to fat embolization and subsequent complement activation in the retinal precapillary arterioles causing leucocyte aggregation is an additional pathway. Ischaemia of the microvascular bed is the final outcome which gives rise to the characteristic retinal appearance.5,7
The only reported incidence of PuR or PulR in literature is 0.24 cases per million population per year. The mean age of the cases considered was 42 years. In addition to being rare, being asymptomatic, being undiagnosed and underreported contributes to its reported low incidence.4,8
Diagnosis of PulR is clinical with the history of visual loss in the presence of a systemic illness like acute pancreatitis and the characteristic fundoscopic changes. It can be either unilateral or bilateral. Retinal haemorrhages, cotton wool spots, macular oedema and pathognomonic Purtscher flecken confirmed the diagnosis with the help of fundal photography and OCT. 8 Central retinal artery occlusion (CRAO) and central retinal vein occlusion (CRVO) can be considered in the differential diagnosis of PulR. CRAO is usually due to an embolus obstructing the narrow segment of the retinal artery causing a diffuse area of retinal whitening with no retinal haemorrhages in contrast to patches of retinal whitening and haemorrhages seen in PuR. In CRVO, there is thrombosis or inflammation of the central retinal vein. The fundoscopic appearance of PuR is easily distinguishable from both CRAO and CRVO. 3
Intravitreal steroids are used in the treatment of PuR though current evidence does not show significant difference in the improvement of visual acuity when compared with observation. Ability of corticosteroids to stabilize the damaged neuronal membrane and microvasculature and inhibit complement activation leading to leucocyte aggregation can be attributed to the improvement in visual acuity noted in some case reports.7,8 Systemic therapy with corticosteroids particularly high-dose intravenous methylprednisolone, intravitreal bevacizumab and hyperbaric oxygen therapy has been used in isolated case reports with varying success. However, none of the therapies have sufficient evidence to be recommended in the treatment.4,9 Thus, observation and management of the underlying condition with a trial of intravitreal corticosteroids is acceptable in the current context.
Although the retinal haemorrhages, cotton wool spots and macular oedema improved 3 weeks following the treatment, there were poor prognostic features in the OCT like macular atrophy and disrupted IS/OS junction. The initial ischaemic insult must have been unsalvageable despite the improvement in morphology with treatment. This was confirmed by VEPs which showed severe axonal loss.
The aetiology for our patient’s chronic pancreatitis was investigated with imaging and metabolic screening. Magnetic resonance cholangiopancreatography and CECT did not detect any gall stones or ductal abnormalities. Calcium levels, lipid profile, IgG4 levels and anti-nuclear antigen levels were done, and it excluded metabolic and autoimmune causes. She did not have a drug history that might have precipitated nor a family history of pancreatitis. Genetic studies were not performed due to economic constraints. To date the patient remains free of further episodes of acute pancreatitis. If she develops another episode, she will be at an increased risk of losing the right eye. Though the literature does not report recurrence of PuR with repeated systemic insults, the pathophysiological mechanism has the capability to affect the other eye. Thus, in the subsequent management, the patient’s right eye should be monitored closely, preferably with fundoscopy.
With or without treatment, the final outcomes of PuR can vary from complete resolution to permanent loss of vision.4,8 Early recognition and prompt diagnosis have a role in ensuring a better prognosis. Routine visual assessment including a fundoscopic examination in patients with acute pancreatitis will facilitate detection of this rare condition early as the cause of the disease. In addition, novel therapeutic options need to be investigated to improve rates of visual recovery.
Conclusion
PulR is a rare complication of acute pancreatitis which can result in permanent loss of vision. Awareness of this complication will ensure its early detection and the search for newer therapies.
Footnotes
Acknowledgements
Authors wish to acknowledge all the ward staff who took care of this patient.
Author contributions
G.B.K.D.B. and C.G. wrote the original draft which was reviewed and edited by D.S., and N.F. P.S. provided resources for the formulation of the case report and along with N.F. was involved in the formal analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from a legally authorized representative for anonymized patient information to be published in this article.