
Abstract
A 28-year-old male hospitalized with a diagnosis of acute pancreatitis presented with sudden onset of blurred vision in both eyes after 48 h of admission. Visual acuity was counting fingers in both eyes. Fundus examination revealed multiple cotton wool spots and intraretinal hemorrhages typical of Purtscher’s retinopathy. Optical coherence tomography macula showed serous macular detachment. In 8 weeks follow-up, visual acuity improved to 6/18 oculus dexter (OD) and 6/60 oculus sinister (OS) with resolution of fundus lesions and resorbed subretinal fluid. Purtscher-like retinopathy, though rare should be considered as a differential in all cases with vision loss in acute pancreatitis. This particular case highlights the significance of a thorough examination of the fundus by an ophthalmologist in identifying this infrequent condition that is often overlooked.
Introduction
The first case of Purtscher’s retinopathy was described in 1910 by Otmar Purtscher in a patient who suffered severe head trauma. Though classical Purtscher’s retinopathy is thought to occur after trauma to the head, neck, or thorax, crush injuries, long bone fractures, and barotrauma, a similar clinical picture can also be seen in a multitude of nontraumatic conditions, in which case the term “Purtscher’s-like retinopathy” is used. 1
Some common systemic conditions that can lead to Purtscher-like retinopathy are acute pancreatitis, fat embolism, amniotic fluid emboli, pancreatic adenocarcinoma, autoimmune disease, renal failure, and other rare causes are thrombotic thrombocytopenic purpura, hemolytic uremic syndrome, and cryoglobulinemia. 1
Pathogenesis involves embolic occlusion of the precapillary arterioles. Potential emboli include air, fat, platelets, fibrin, leukocyte aggregates as well as exogenous particle. 2 In patients with acute pancreatitis, complement activation may induce the formation of these leukocyte aggregates. 1
Clinical presentation is variable, with some patients presenting with profound vision loss and others with minimal changes. Loss of acuity may be accompanied by field loss in the form of central, paracentral, or arcuate scotoma. A relative afferent pupillary defect may or may not be present. Fundus findings are cotton wool spots, retinal hemorrhages, and Purtscher’s flecken (multiple, discrete areas of whitening in the inner retina between the retinal arterioles and venules), usually confined to the posterior pole. A pseudo-cherry red spot may be seen when the confluent retinal whitening surrounds the posterior pole. The acute retinal changes may not be apparent until 24–48 h of systemic illness. Prognosis is variable and largely depends on the extent of retinal involvement. The pathological changes usually resolve spontaneously without treatment within 1–3 months. Poor prognostic factors include optic disc swelling, pseudo-cherry red spot, macular edema, involvement of outer retina, choroidal hypoperfusion, and retinal capillary non-perfusion in fluorescein angiography.1,3
Till date, there is no consensus on the treatment of Purtscher-like retinopathy. Many treatment options, like high-dose steroids, and hyperbaric oxygen therapy, low molecular weight heparin (LMWH), have been suggested but with variable outcomes.
Case report
A 28-year-old male presented with sudden onset of blurred vision in both eyes. The patient had been hospitalized for 48 h for severe epigastric pain and vomiting. He had a history of alcohol intake for 5 years and have had a binge of alcohol intake (one liter 40% alcohol by volume) 3 days back. He had no previous history of binge drinking and had no significant medical and surgical history.
On examination, best corrected visual acuity was counting fingers in both eyes. Anterior segment findings were within normal limits. Fundus examination revealed bilateral peripapillary cotton wool spots and a few flame-shaped intraretinal hemorrhages consistent with Purtscher’s retinopathy (Figure 1). Optical coherence tomography (OCT) of the macula showed a serous macular detachment in both eyes (Figure 2).

Multiple peripapillary and posterior pole cotton wool spots (blue arrow), few peripapillary flame-shaped hemorrhages (green arrow) at presentation.
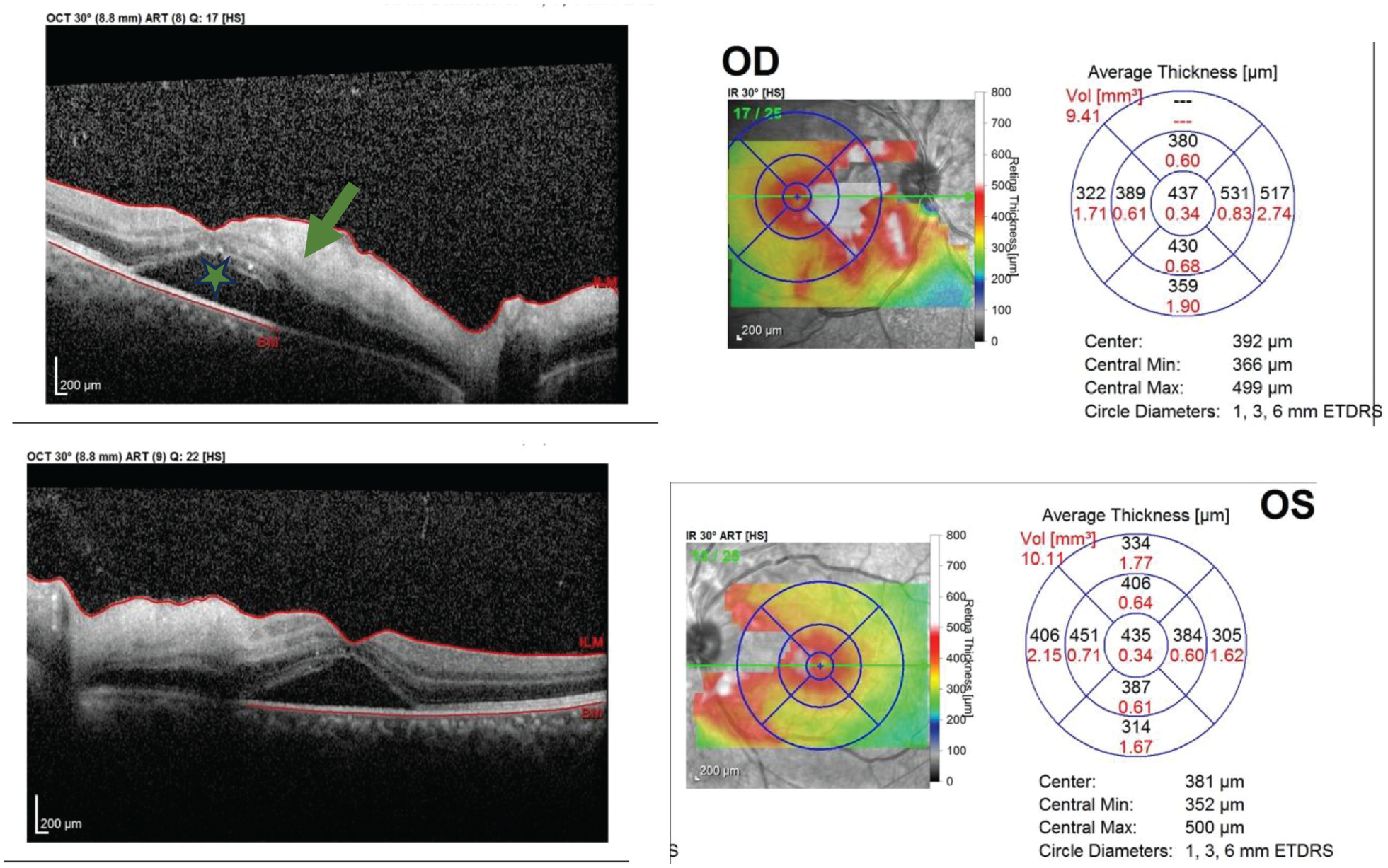
OCT macula and thickness map of both eyes showing inner retinal hyperreflectivity/thickening (green arrow) and serous macular detachment (asterisk).
Blood tests revealed a raised C-reactive protein (CRP) at 20 mg/L, a raised amylase (501 U/L), a raised lipase (1527 U/L), a decreased platelet count (71,000/cumm), and a raised Aspartate transaminase/Alanine transaminase (SGOT/SGPT 249/134). Prothrombin time (PT) activated partial thromboplastin time (aPTT), fibrinogen level, blood glucose, and electrolytes (Na, K, Ca, Mg) were within normal limits. Ultrasound of the abdomen showed a mildly enlarged pancreas, dilated pancreatic duct, and an ill-defined pancreatic head region suggestive of acute or chronic pancreatitis.
Computed tomography (CT) of the abdomen and pelvis showed features of acute severe necrotizing pancreatitis with peripancreatic collection, mild ascites, and mild bilateral pleural effusion (modified CT severity index = 10).
Patient was managed with intravenous fluids (Ringer’s lactate 3 mL/kg/h for 24 hfollowed by maintenance fluid), parenteral analgesics (tramadol 50 mg 8 h), and prophylactic antibiotic (meropenem 1 g 8 h) and was discharged after a week when clinical improvement was seen. No systemic steroids were administered, given the limited evidence of improved visual outcomes with steroid treatment. 4
At 2 weeks follow-up, the patient’s vision was 3/60 OU. The fundus examination showed relatively fewer cotton wool spots and few hemorrhages (Figure 3). An OCT scan of the macula revealed resolution of the serous macular detachment OD and improvement in the detachment OS (Figure 4).

Fundus findings at 2 weeks follow-up.

OCT macula and thickness maps of both eyes at the follow-up visit showing resolved serous fluid with diffuse macular thinning more profound nasally.
After 8 weeks, fundus lesions had completely disappeared (Figure 5) and best corrected visual acuity improved to 6/18 OD and 6/60 OS.

Resolved fundus lesions at 8 weeks follow-up.
Discussion
Purtscher’s retinopathy is an occlusive microvasculopathy associated with trauma and when the similar changes occur in nontraumatic conditions, it is labeled as Purtscher-like retinopathy. In acute pancreatitis, the pathophysiology is thought to be a result of release of proteolytic enzymes into the systemic circulation with subsequent activation of complement cascade and the formation of C5a-induced aggregates of leukocyte, platelets, and fibrin that cause retinal embolization and ischemia. 5
It usually occurs after the onset of acute pancreatitis. Howbeit, a report by Sanders et al. 6 described a patient with Purtscher-like retinopathy 2 weeks before the onset of acute pancreatitis and another report by Sharma et al.6,7 mentioned similar findings in a case of chronic pancreatitis who developed acute pancreatitis 6 months later.
Other causes of bilateral loss of vision in acute pancreatitis could be attributed to lateral geniculate body (LGB) pathology (hemorrhagic infarction and osmotic demyelination). 8
There have been numerous reports describing the association of acute pancreatitis with Purtscher-like retinopathy. However, none of these reports have mentioned the occurrence of serous macular detachment in conjunction with Purtscher-like retinopathy in cases of acute pancreatitis.
Two reports have specifically discussed the occurrence of serous macular detachment with Purtscher-like retinopathy. In a report by Tang Anthony et al. the occurrence of serous macular detachment has been discussed in acute onset Still’s disease. But, unlike our case, the macular detachment occurred secondary to exogenous steroid administration. 9
Another report by Ozdamar Erol et al. described the association of Purtscher-like retinopathy and serous macular detachment in a case of preeclampsia. 10
The visual outcomes may vary, though retinal lesions resolve completely over a period of time. Management should aim at the treatment of underlying systemic conditions. There are few reports mentioning the role of corticosteroids but with a varied outcome.
In our patient, spontaneous visual recovery occurred but was incomplete probably due to ischemic changes at macula.
Conclusion
Purtscher-like retinopathy is a rare complication of acute pancreatitis and presents as sudden loss of vision. Typical fundus findings can help in the diagnosis. Serous macular detachment may be an associated finding, in which instance OCT can be helpful in quantifying the macular edema and thus can help in monitoring the patient. Resolution of the lesions occur spontaneously with or without complete visual recovery.
Footnotes
Data availability
The authors confirm that data supporting the findings of this study are available within the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.