
Abstract
A 63-year-old patient with skin neurofibromas since birth was brought to emergency in a critical state due to massive bleeding per rectum. After stabilization and massive transfusion, the patient underwent Gastro-Intestinal (GI) endoscopy and abdominal computed tomography. A mass was identified in the jejunum. On laparotomy, multiple neurofibromas were seen in the jejunum. The segment with bleeding tumour was resected. Histopathology revealed benign spindle cell neoplasm, a gastrointestinal stromal tumour. The patient recovered and was discharged on day 15.
Keywords
Introduction
As early as 1882, Von Recklinghausen described neurofibromatosis as a neuro-dermatological disease. In 1983, I Vujic, RD Sbrocchi, et al. demonstrated angiographically that there can be neurofibromas in the gastro-intestinal tract from the jejunum to the distal ileum. 1 Though clinical characteristics were described long back in the form of skin neurofibromas, café au lait spots, leish nodules and axillary freckles, called ‘probands’ were defined later. Genetic studies were also done much later, and today neurofibromatosis 1 is diagnosed by the presence of 1 proband and a heterozygous NF1 pathogenic variant. 2 These patients may have localized lesions, but suffer from similar complications as NF1 patients. 3 I Pinsk, O Dukhno et al. estimated that about 11%–25% of NF1 patients have gastrointestinal involvement mostly in the form of stromal tumours. 4 Nada Garrouche, Amel Ben Abdallah et al. described a spectrum of gastrointestinal lesions in NF1 ranging from microscopic proliferative lesions to large neurofibromas, neuroendocrine and gastrointestinal stromal tumours (GIST). 5
Case report
A 63-year-old man was admitted to the Department of Emergency medicine with complaints of massive per rectal bleed for 2 days.
On presentation, he was pale, exsanguinated.
Pulse rate 112 beats per minute, blood pressure: systolic 80 and diastolic 50 mmhg.
Examination revealed multiple neurofibromas over the abdominal wall and trunk (Figure 1). The abdomen was soft and tender, and per rectal examination revealed large amounts of altered blood. He was shifted to the intensive care unit.

Neurofibromatosis lesions are seen.
Laboratory investigations: Haemoglobin (5.10 mg/dl), TLC 4700 platelets (83,000/cumm). Urea 98 mg/dl creatinine 1.23 mg/dl Liver Function Tests (LFT) normal, serum albumin 1.3 gm/dl. The abdominal ultrasound was normal.
Upper GI endoscopy was normal. A colonoscopy revealed blood coming from ileum and above. In the colon, there was one large haemorrhoid at an 11 o’clock position and two small haemorrhoids at a 5 o’clock position, but these were not bleeding.
Contrast-enhanced computed tomography (CECT) scan of the abdomen showed an iso-dense ill-defined lesion of size measuring 22 × 20 mm showing post-contrast enhancement in the proximal jejunum (Figure 2).

CECT scan of abdomen over abdomen showing ill-defined lesion in proximal jejunum.
As there was ongoing bleeding, the decision was taken for surgical intervention. Before the procedure, the patient was given massive blood transfusions of four points of packed cells, four random donor platelets and four fresh frozen plasmas. Exploratory laparotomy revealed multiple neurofibromas throughout the small intestine of varying size with the largest one in the proximal jejunum (Figure 3(a) and (b)). The segment of the jejunum containing the large neurofibroma was resected, and jejuno-jejunal anastomosis was done. Day 2 of postoperative period, the patient developed breathlessness. X-ray findings were suggestive of Tranfusion related acute lung injury (TRALI). The patient was treated with oxygen and other supportive measures. He improved and was discharged on day 15 of the hospital stay.
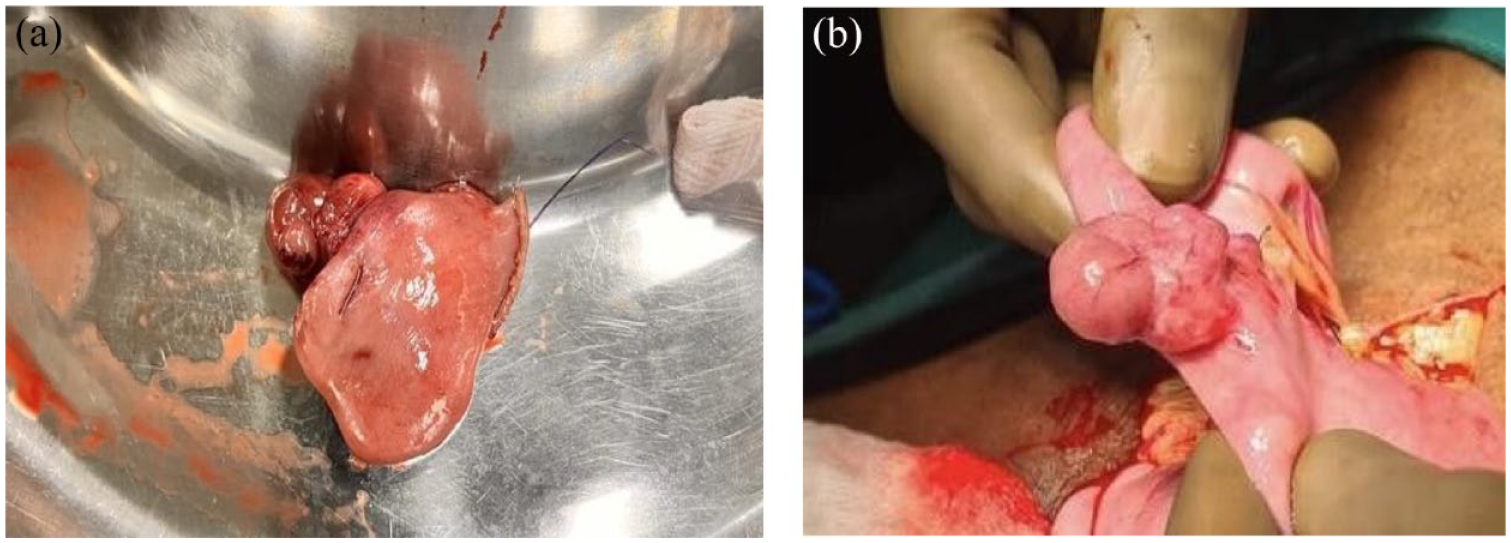
(a) shows resected specimen & Figure (b) shows specimen of large neurofibroma which was present in proximal jejunum and taken out during exploratory laparotomy.
The resected nodule was sent for histopathology analysis, and the report was suggestive of benign spindle cell neoplasm (Figure 4(a)), possibly GIST.

(a) (×200, H&E) showing bland spindle cells with faintly eosinophilic cytoplasm in a syncytial pattern. (b) (×200) CD117 marker showing strong positivity. (c) (×200) S100 marker is negative.
CD117 and S100 markers were tested which turned out to be positive and negative, respectively (Figure 4(b) and (c)).
Follow up
Patient has been on regular follow-up for every month for 3 months now and has gained weight.
Discussion
Case reports have been published reporting a case of rectal cancer in NF1 patients, volvulus due to multiple mesenteric neurofibromas and isolated colonic neurofibroma.6–8
Ricci Kalayanamitra, Zainab Shahid et al., 9 report a young patient of NF1 who presented in a subacute manner with anaemia and intermittent malena due to a bleeding GIST.
Milos Stevic, Marina Vlajkovic et al. reported a case similar to ours with massive GI bleed. Magentic Resonance Imaging (MRI) showed a tumour in small pelvis, further delineated as GIST by GI bleeding scintigraphy with TchM99 in vivo labelled Red blood cell (RBC) scan. Of the multiple jejunal tumours, the bleeding one was resected and turned out to be a neurofibroma. 10 Amit Hudgi, Mohammad Azam et al. report a case of massive, life threatening GI bleed due to a GIST of terminal ileum diagnosed on video capsule endoscopy. 11 In 2022, Ashok Gunawardane, Jesse Fischer et al. report a case of a 54-year-old patient of NF1 who had undergone right adrenalectomy for pheochromocytoma and surgery for left optic glioma and now presented with massive GI bleed. CT enterography revealed hypervascular nodules and small bowel resection done. 12 In our patient, diagnosis was based on colonoscopy and abdominal CT. He received ‘massive transfusion’ 4 PCV, 4 RDP and 4 FFPs before surgery. He developed a delayed TRALI, transfusion associated lung injury, on post-op day 3, was treated with supportive therapy, recovered and discharged from hospital after 11 days. The patient has been advised to have regular follow-up and a yearly assessment for any recurrent GI bleed.
In case of localized and resectable GIST, surgical treatment is the mainstay, and laparoscopic surgery is a valid alternative. In fact, laparoscopid approach is safe and effective if the oncological radiality is respected. 13
Conclusion
Patients with neurofibromatosis 1 have various systemic presentations. Gastrointestinal bleeding due to neurofibromas can be life-threatening. Though difficult, a combination of colonoscopies, and imaging techniques can locate the bleeding tumour. Multi-disciplinary teamwork for stabilizing the patient and timely intervention with surgical resection can be life-saving.
Footnotes
Acknowledgements
The authors would like to acknowledge Dr Mahesh Thombre, Gastrosurgeon (HOD), Dr D Bannerji HOD Gastroenterology, Dr Komal D Sowaimul AP dept. of Pathology, Dr. D.Y. Patil Medical College and Hospital, Dr. D.Y. Patil Vidyapeeth, Pimpri Pune.
Author contributions
V.G. has made a substantial contribution to the concept and design of article and the interpretation of data for the article and revised it critically for important intellectual content. V.L. has made a substantial contribution to acquisition analysis and drafted the article. S.M., P.Y. and S.P. agreed to be accountable for all aspects of the work in ensuring that questions relate to the accuracy or integrity of the work and are appropriately investigated and resolved.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.