
Abstract
A 54-year-old African-American male presented to the colorectal surgery clinic with the chief complaint of a painful anal swelling that had been ongoing for several weeks. An adequate rectal examination was not possible due to severe pain. Therefore, he was taken to the operating room for an exam under anesthesia where a presacral mass was identified. A transgluteal core needle biopsy was performed which was consistent with gastrointestinal stromal tumor. Computed tomography imaging identified a 16 cm ×10 cm ×9 cmrectal gastrointestinal stromal tumor. Given the size and location, the patient began treatment with neoadjuvant Imatinib. His progress was followed with serial computed tomography scans and clinic visits. A 3D model was created the tumor and surrounding structures to aide in pre- and intraoperative planning. The model was utilized during patient education and found to valuable in describing the potential for levator invasion and framing potential post-operative outcomes. The patient was able to undergo rectal preservation via a robotic low anterior resection with a transanal total mesorectal excision, coloanal anastomosis, and diverting ileostomy.
Keywords
Introduction
Three-dimensional (3D) printing is a manufacturing process initially undertaken in the aeronautic and automotive engineering industries.1,2 Advances in 3D printing technology have permeated the medical field and have led to 3D printing patient-specific anatomic models. 3 It has been used in a wide array of specialties, from orthopedics, physical medicine and rehabilitation (PM&R), surgical oncology, urology, neurosurgery, and cardiac surgery, to name a few.4,5 Another interesting application is surgical models for trainee education.6,7
There have been many different applications of 3D models. Orthopedic surgery has created preoperative models to aid in sizing joint replacements. 8 Various solid organ tumors have been printed to plan the best approach to resection to minimize blood loss or injuring abutting structures.9–11 PM&R has printed various devices for patients to improve the accessibility of patients and their environment, such as joint prosthetics. 5 During the pandemic, the Richmond VA Medical Center used 3D printing to print COVID nasal swabs to help overcome supply chain disruptions.
In this case report, we describe our experience implementing 3D printing technology in planning and informed consent with a patient with a very low rectal tumor. We hypothesized that having a 3D model of the tumor and the surrounding structures would help anticipate potential issues in the operating room and the extent of the operation and improve the patient’s understanding of his disease process, all of which have been documented in the literature. The Institutional Review Board at our facility deemed it unnecessary to get informed consent to publish this case report. However, the informed consent process at the VA includes using deidentified information for publication, in which the patient signed and agreed.
Case
A 54-year-old male presented to the colorectal surgery clinic with the chief complaint of a painful anal swelling that had been ongoing for several weeks. He denied any obvious drainage but would occasionally notice some moisture. He had had regular bowel movements with occasional pain but no blood. His vitals in the clinic were a heart rate of 106 beats per minute, blood pressure of 145/87, respiratory rate of 18 breaths per minute, and a temperature of 98.2°F. On the physical exam, a large, firm, tender posterior anal mass was noted; on a digital exam, a small amount of what was thought to be pus was noted on the examiner’s finger. A complete blood count from approximately 6 weeks earlier was significant for 11.4 × 103 white blood cells. Differential diagnoses at the time were perirectal abscess, presacral mass, malignant neoplasm of the rectum, or pelvic abscess.
Upon arrival to the operating room, the patient was placed under general anesthesia and in a prone jackknife position. The operative surgeon conducted a digital rectal exam; he could not feel a superior margin to the posterior perirectal mass. A rigid proctoscope was then inserted, and a posterior mass indenting the posterior rectal wall was noted and extended superiorly 11 cm from the anal verge. Once past the mass, the rest of the rectum and sigmoid appeared normal. Proctoscopy revealed no mucosal irregularities, and no pus was noted. Next, a fine needle aspiration using an 18-gauge needle with a syringe was inserted via the posterior midline perianal skin located one-inch posterior to the anal verge and directed superiorly into the retrorectal mass. Aspiration produced a red, gelatinous material. The aspirate was sent for cytology, biopsy, and culture, and the procedure was terminated.
The pathology results were significant for strong diffuse expression of vimentin, CD68, and CD34 and weak patchy CD10. There was a strong CD117 and DOG1 expression concerning gastrointestinal stromal tumor (GIST). A c-kit exon 11 mutation was noted with a p.K550-K558 deletion. The Ki67 exceeded 10%. At the time of diagnosis, the tumor was classified as T4N0M0, equating to stage IIIB.
While waiting for the pathology results, the patient was sent for a CT scan of his abdomen and pelvis. The mass was measured as 10 cm × 9 cm × 16 cm, located between the rectum and the sacrum (Figure 1). He also underwent a CT scan of his chest which did not demonstrate metastatic spread. Preoperative positron emission tomography-computed tomography (PETCT) scan was considered, however, given the patient’s severe symptoms. Imatinib was started urgently before a baseline PETCT could be scheduled. The utility of PETCT surveillance in the absence of pretreatment imaging was deemed limited. 12

Initial sagittal and coronal computed tomography imaging of gastrointestinal stromal tumor.
Within 1 month of treatment the patient’s symptoms of rectal pain had resolved, and he had no treatment-related side effects. He was able to discontinue his narcotic pain medications due to the resolution of the pain associated with the tumor. Interval CT scans demonstrated regression of the tumor, reaching a nadir of 8.5 cm × 4.2 cm × 3.5 cm at 11 months of Imatinib. However, at the 14-month interval imaging, the tumor was noted to have grown to 10.0 cm × 6.3 cm × 4.2 cm on the final preoperative MRI. At which point, maximum treatment response had been achieved.
Surgical intervention was needed as the tumor showed signs of evading medical treatment. Despite imaging showing a tumor volume reduction by approximately 81.6%, the tumor was abutting the sphincter complex and indistinguishable from the left levator ani muscle. Risks and benefits of abdominoperineal resection versus rectal preservation were presented to the patient. Rectal preservation is associated with increased chance of incontinence and higher likelihood of a positive surgical margin given involvement of the sphincter complex. Abdominoperineal resection is associated with a higher wound complication rate. Given the patient’s excellent neoadjuvant response rectal preservation was perceived to be medically appropriate, with abdominoperineal resection being reserved as a salvage approach if necessary.
The Central Virginia VA Health System recently started developing 3D-printed medical models. The surgical team requested a model to appreciate the three-dimensional relationships and anatomical structures involved for preoperative planning and patient education. The operating surgeon requested that the model contain the tumor, anal sphincters, and levator ani. Two separate models were created. The CT scans were segmented using Materialize (Belgium) medical segmentation software. First, a colorful resin model printed on a Dynamism xRize 3D printer (Denver, USA) that cost less than $30 was printed, which took approximately 8 h to print (Figure 2). A second model was printed with a translucent and flexible material on a Stratasys J750 Digital Anatomy Printer (Minnesota, USA), which cost approximately $300 and took 6 h to print (Figure 3).
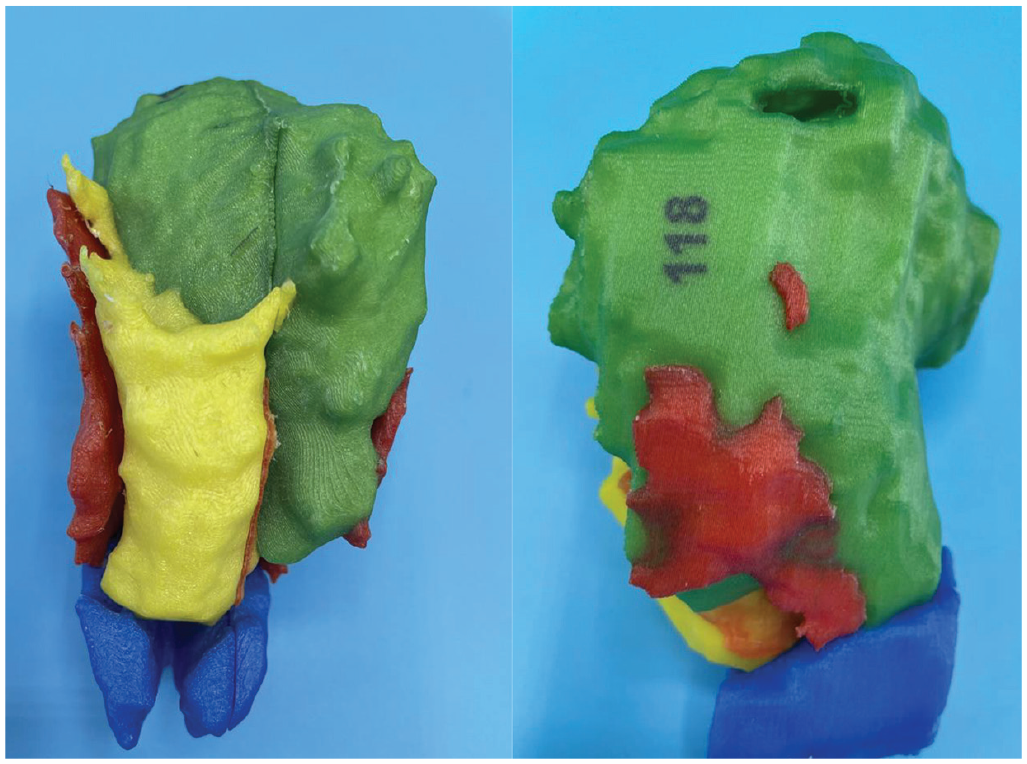
3D printed model of gastrointestinal stromal tumor (green), rectum (yellow), levator ani muscles (red), and sphincter complex (blue). Model was able to be split down the long axis of the gastrointestinal stromal tumor at the request of the surgeon.

3D printed model of gastrointestinal stromal tumor (solid pink), rectum (white), levator ani muscles (translucent red), and sphincter complex (clear). Model was able to be split down the long axis of the gastrointestinal stromal tumor at the request of the surgeon.
The patient underwent a robotic low anterior resection, transanal total mesorectal excision, and coloanal anastomosis with diverting ileostomy. The patient remained in the hospital for 1 week. Figure 4 shows the specimen after removal. Figure 5 shows a view of the pelvis during the operation.

Surgical specimen. The gastrointestinal stromal tumor measured approximately 8 cm.

Intraoperative photo left levator ani sacrificed to adequately resect the gastrointestinal stromal tumor (asterisks marks ischiorectal fossa).
Final pathology showed a GIST, spindle cell type, measuring 3.0 × 2.5 × 2.0 cm, high grade with mitotic rate >5 per high powered field, a Ki67 index of 30%, and 0/4 lymph nodes positive: final staging, pT2N0M0, staging IIIB. Margins were microscopically clear of disease indicating an R0 resection. The size discrepancy is directly related to the fact that the majority of the tumor was necrotic and liquefied as was reported on the preop MRI “Persistent heterogeneous signal of the tumor, with now more discrete fluid levels/hematocrit levels, likely reflecting necrosis and cystic degeneration.” Liquefied component of the tumor did not survive fixation and pathologic processing. Most recent follow-up visit and imaging were in January 2023 in which there was no evidence of disease.
The 3D model created by the GIST provided value to the patient’s care. The patient had a chance to hold and examine the model. He stated he felt more comfortable with the surgery and why the specific approach was selected, thus, aiding in informed consent. The residents involved in the surgery and perioperative care gained a better appreciation of what to expect and possible difficulties during the resection. Discussing the model with the attendings involved, while they were impressed with the technology and future applications, the model did not provide any new information or change the surgical approach. None of the people involved felt the more expensive model provided more or better information than the cheaper model.
Discussion
Spatial reasoning and surgery
A prerequisite to surgery is understanding a patient’s anatomy before an operation. 13 Traditionally, a surgeon would collate 2D radiographical images to anticipate the 3D environment he/she would be operating. 14 This process can be complicated for junior surgeons, especially when anatomy is complex, altered, or varied from standard arrangements.
Surgeons constantly use tactile feedback in the operating room to confirm anatomy and predict what structures can and cannot be removed or altered. Integrating visual and tactile feedback with working with 3D models helps to increase the accuracy of spatial relationships prior to the operating room.15,16 Multiple studies have demonstrated decreased operating room times, decreased anesthesia time, 17 reduced blood loss, increased surgeon confidence, and improved patient education and communication when 3D-printed models have been integrated into patient care.3,13
How has 3D printing been applied in surgery?
3D printing has been implemented in every step of surgery. The applications include anatomic models, surgical instruments, surgical marking guides, implants, and prostheses. 18 Many times, applications can fall into more than one group and be changed throughout an application—usually, preoperative applications of 3D printing center on planning an operative approach. A model can also be used in the informed consent process aiding in the patient’s understanding of an operation.
Intra-operatively, 3D-printed models are usually navigational. For example, marking guides provide physical guidance to the surgeon as the surgical incision is made or may serve as practice before an operative procedure. Additionally, models can be brought into the operating room and utilized for visual ques of landmarks during a case. Finally, the surgeon can use 3D models to educate trainees or patients prior to or following a procedure. This list is in no way exhaustive, and other applications are being developed, such as instrument creation, printed implants, assistive technologies, and bioprinting.
3D printing in the VA system
The Veterans Health Administration (VHA) is uniquely positioned to be a leader in medical 3D printing. In 2017, the VHA launched the VA 3D printing network by placing 3D printers in five hospitals. 19 Since that initiative, the program has grown from three hospitals to 75 sites with a central program office. 20 In 2020, three sites within the 3D printing network became FDA-registered advanced manufacturing “hubs” focusing on building and distributing patient-specific products for veterans. 20 The VHA 3D printing network is the largest in the country and has developed a unique infrastructure to provide 3D printing consultation services. 20 The VHA vision is for every Veterans Affairs Medical Center to have access to advanced manufacturing and provide eligible veterans with personalized care.
Conclusion
This case was a fantastic demonstration of how medicine, surgery, and technology continue to evolve. Between the remarkable advancement in targeted cancer therapy, improvements in medical imaging with translation to 3D modeling, and continued perfection of minimally invasive techniques, our patient had as good of an outcome as expected. It is too soon to claim victory over his GIST just yet, and we still have to see about reversing his ileostomy, but this case is encouraging of what lies ahead in medical advancements.
Footnotes
Author contribution
L.K.-B. contributed to manuscript draft and editing, concept, 3D segmentation; D.O. involved in manuscript draft; A.K., W.T., and L.F. are content experts who involved in manuscript editing; M.A. is concept and content expert who focused on manuscript editing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was funded by the Department of Veterans Affairs.