
Abstract
Hydrocalyx is a dilated renal calyx due to obstruction of the infundibulum and a rare complication after percutaneous nephrolithotomy. We present a 22-year-old girl with hydrocalyx who had following percutaneous nephrolithotomy and its management. A 22-year-old female with recurrent right flank pain underwent percutaneous nephrolithotomy for a kidney stone. Despite interventions such as endoscopic infundibulotomy and double J stenting, the patient experienced persistent symptoms. Laparoscopy ultimately led to improvement. Hydrocalyx is a rare but significant complication post-percutaneous nephrolithotomy. Minimally invasive procedures and endoscopic interventions are the primary treatment options. Laparoscopy may be considered if initial interventions fail. Formation of hydrocalyx after percutaneous nephrolithotomy is a rare yet considerable complication and there are only a few articles in this field available to our knowledge.
Introduction
Hydrocalyx is a dilated renal calyx due to obstruction of the infundibulum. Formation reasons of hydrocalices are included of congenital, post infectious, post traumatic, or iatrogenic injuries.1,2 Since urine production continues in hydrocalyx, hematuria, infection, and pain are the possible symptoms. 3
Decompressing of the calyx, alleviating the obstruction, and treatment of coexisting nephrolithiasis are the components of hydrocalyx treatment. 4
Percutaneous nephrolithotomy (PCNL) is a minimally invasive surgical method, complications rate is up to 83% of cases, they may happen during or after the procedure, even several years after it.5,6 Most of the complications are minor, including bleeding or fever which need no intervention to eliminate. 5 Renal collecting system obstruction is a rare post-PCNL complication, but ureteral stricture or avulsion, blood clot, infundibular stenosis, or transient mucosal edema can cause the obstruction.7,8
Importantly, the literature on hydrocalyx post-PCNL is limited. This dearth of documented cases underscores the novelty of our report, offering valuable insights into the complexities of hydrocalyx formation after PCNL and contributing to the limited existing data in this field. 7
Case presentation
A 22-year-old woman presented with recurrent right flank pain that had been occurring for the past 3 years, typically alleviated after passing kidney stones. She had a history of kidney stones without signs of infection or hematuria. Additionally, she underwent tonsillectomy at age 3, appendectomy at 4, rectal prolapse surgery at 11, and umbilical hernia repair surgery at 20.
In another clinical center in January 19, 2021 she referred because of severe pain of right flank for the first time. The abdominal computed tomography (CT) showed a 9 mm stone in right kidney (Figure 1(a)). In February 18, 2021 Extracorporeal Shockwave Therapy (ESWL) was performed on the patient. Since it was not efficient, in March 9, 2021, PCNL was executed and the stone was extracted. But in April 20, 2021 flank pain and nausea and vomiting dragged her back to the hospital and a DJ was applied, which in May 21, 2021 it was removed. Flank pain and nausea/vomiting continued since then. In July 1, 2021, abdominopelvic sonography showed mild to moderate hydronephrosis at right kidney.
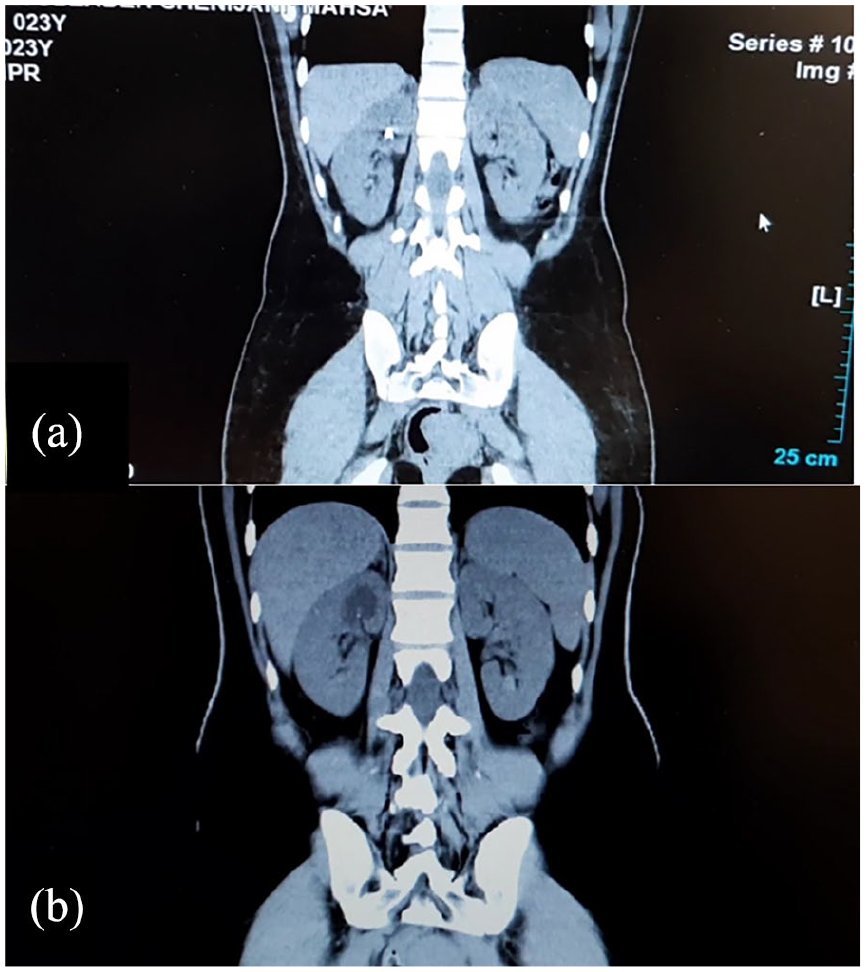
(a) First computed tomography (CT) scan shows the stone (b) First CT scan in our center shows the hydrocalyx several months after undergoing percutaneous nephrolithotomy in patient with recurred pain.
In August 18, 2021, she referred to Labbafinejad hospital and at first an abdominopelvic CT scan without contrast was performed, in which the hydrocalyx was obvious and no stone was visible (Figure 1(b)). Also, her labs were totally normal and there was no infection or hematuria in her labs as they are mentioned in Table 1. In September 14, 2021, Intravenous Pyelogram (IVP) was performed in which the absence of right upper calyx was obvious (Figure 2(a)), and in October 13, 2021, percutaneous nephrostomy tube insertion in right upper calyx and percutaneous nephrocystography was performed and the isolated right upper calyx was observable (Figure 2(b)).
Lab data.
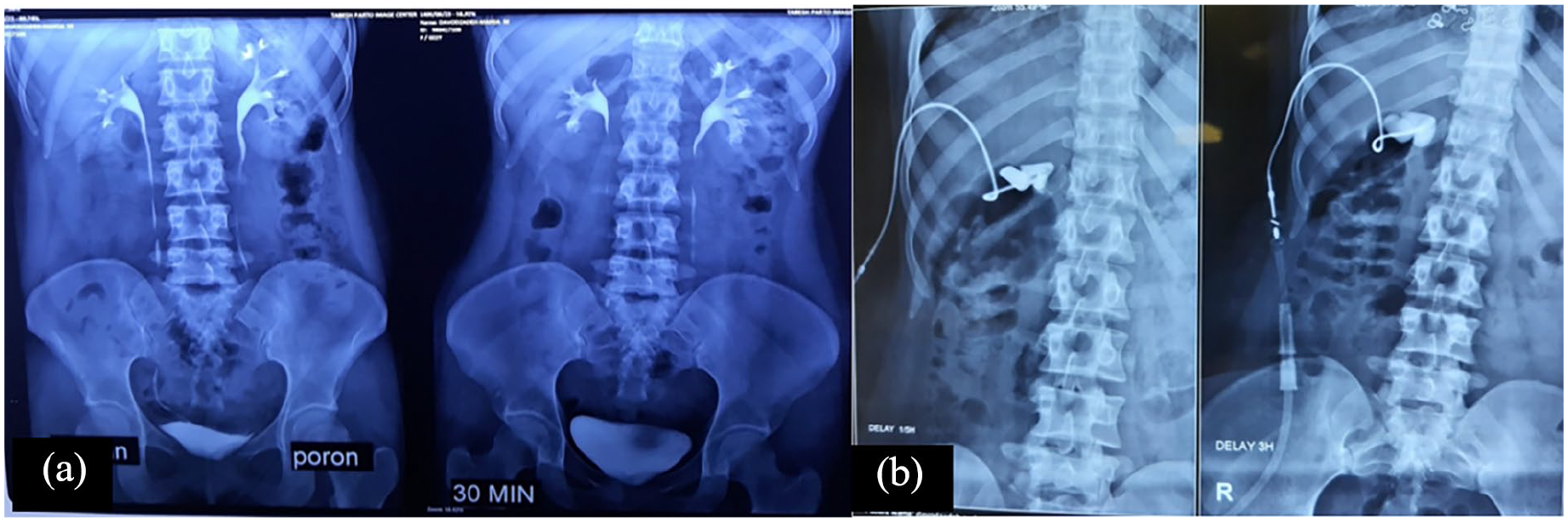
(a) IVP and the absence of right upper calyx (b) Percutaneous nephrocytography shows the isolated calyx.
Ultimately in November 6, 2021, under fluoroscopic control, endoscopic infundibulotomy of right upper calyx was performed. At first in sterilized circumstances of operation room, right ureteroscopy was performed. Then we injected radiocontrast agent through the applied nephrostomy and the ureteroscope was aligned with upper calyx and by the guidance of fluoroscopy, manipulation, and rupturing of the block was done. We used semi-rigid uroscope of Wolf made in Germany. The tip of nephrostomy tube was emerged and by methylene blue injection into nephrostomy tube, the accuracy of the procedure was approved. A Double J was applied and a month later it was removed. After 6 months, in first follow-up, the patient reported that the right flank pain is back. Recurred stricture of infundibulum and hydrocalyx was obvious in IVP. She went through the second infundibulotomy, and a DJ was applied to be kept for 2 months. Finally, a partial nephrectomy of the right upper pole of the kidney was performed. However, following that, the patient condition did not show any improvement. In our case, as prior interventions yielded inadequate results, laparoscopy was done as the final and ultimately successful intervention. We conducted a laparoscopic endo-infundibulotomy to address the hydrocalyx. Following this procedure, the patient exhibited significant improvement, and a 6-month follow-up confirmed the absence of symptoms.
Discussion
As the endo-surgical methods are developed in managing the upper urinary tract diseases, they are becoming the golden choice to treat the infundibular strictures, caliceal diverticulum, ureteral strictures and ureteropelvic junction strictures.9,10 The treatment of mild and moderate cases include observation and endoscopic dilation but the severe cases can lead to renal impairment.
In our case, the initial pain experienced by our patient was likely attributable to obstruction caused by the kidney stone. However, following the PCNL, the development of a stricture in the calyx’s infundibulum and subsequent hydrocalyx formation have been identified as the underlying causes of the recurrent pain. Given that the hydrocalyx emerged in the patient’s CT scans post-PCNL, we deduce that it represents a surgical complication arising from the PCNL procedure. At the first infundibulotomy the DJ was removed after 1 month but at the second infudibulotomy the procedure has been done in two vertical directions and also the DJ was kept for 2 months. This case report holds significance as it sheds light on a rare complication post-PCNL, contributing valuable insights to the limited existing literature and guiding potential advancements in clinical management.
Conclusion
Our case report underscores the rarity and complexity of hydrocalyx formation after PCNL. Despite initial interventions, including endoscopic infundibulotomy and double J stenting, persistent symptoms necessitated laparoscopic intervention for resolution. The limited literature on this complication emphasizes the novelty and significance of our report, contributing valuable insights to guide future clinical approaches in managing hydrocalyx post-PCNL.
Footnotes
Acknowledgements
None.
Author contributions
A.B., B.N. contributed to Study concept and design; M.D., D.N., H.M. contributed to Data acquisition; S.J., N.R. contributed to Drafting of the manuscript; A.B., B.N. contributed to Critical revision of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.