
Abstract
This case study evaluated the effectiveness of using a combination of faradic and neuromuscular electrical stimulation to improve the sensory and motor function of the bladder/bowel in pediatric patients diagnosed with spina bifida with myelomeningocele. All five patients were pediatric cases aged 4–15 years (mean age 8.4 ± 4.3 years) with complete incontinence in both bladder and bowel functions and self-referred to the Leyaqa Physical Therapy Center in Qatif, Saudi Arabia. All patients had diminished sensation from the hips down and underwent 24 electrical stimulation sessions. Bladder and bowel control were improved by 40% and 20%, respectively. All participants had improved bladder sensation, and 80% had improved bowel sensation. All participants reported improvement in constipation. Feeling the urge or sensation of emptying the bladder or bowel was dramatically improved in all participants. This combination of stimulation electrotherapy can be offered with benefits according to the series of cases studied.
Keywords
Introduction
Spina bifida (SB) has two types: Closed SB, also called SB occulta (which means hidden), is the mildest form of SB. In this form, there is no opening or sac on the infant’s back; thus, the nerves are usually intact.1,2 The second type is open SB, also called SB aperta. 2 This type is more serious than closed SB and refers to an opening between the vertebrae through which a sac of fluids extrudes. 2 There are two types of SB aperta. The first is meningocele, in which the sac of fluid emerges through an opening in the back but without exposure to any nerves. 1 This type of SB is rare but can cause minor disabilities.1,3 The second type is myelomeningocele, the most severe form of SB, characterized as failure of the spine and spinal canal to close before birth. 1 The spinal canal remains open along several vertebrae, allowing the membranes and spinal nerves to push through this opening to form a sac of fluids that exposes tissues and nerves, eventually causing life-threatening infections for the infant.1,3
SB has no definite cure, and management of the condition differs from one person to another, depending on the severity of the complications. 3 SB occulta usually does not require treatment, as the person may live with it without ever being diagnosed. 2 By contrast, SB aperta causes neurological damage that is often irreversible. 1 Therefore, children born with SB aperta are more likely to require multidisciplinary interventions, starting with surgical intervention to position the sac back in place and close the opening in the vertebrae. 1 This must be done within 24–48 h after birth to minimize the risk of infection associated with nerve exposure. 1 Another possible surgical intervention is shunt insertion into the infant’s brain to control hydrocephalus (fluid accumulation in the brain) 1 Children with SB aperta require regular medications throughout their lives to manage and prevent life-threatening complications, 1 which can include total or partial paralysis; orthopedic complications, such as foot deformities and asymmetric hips; scoliosis; hydrocephalus; urinary tract infections; bowel and bladder incontinence; meningitis; dairy allergy; learning difficulties; and depression. 1 Children with SB may also require assistive equipment and rehabilitative therapy, including physiotherapy, occupational therapy, and speech therapy, to improve their quality of life. 1
The following case series study assesses a treatment that supports a combination of faradic electrical stimulation (FES) and neuromuscular electrical stimulation (NMES) as a therapy to improve bowel and bladder control in children with SB with myelomeningocele. Most children diagnosed with myelomeningocele have bladder and bowel incontinence, which leads to various health risks, such as infection of the urinary tract and skin rashes.4,5 The condition can also create psychosocial challenges for both patients and parents. According to the series of cases studied, Faradic nerve stimulation can be offered to improve sensory and motor function of the bowel and bladder for children diagnosed with myelomeningocele, while NMES is also helpful in these children, as it is an approved tool for recruitment of new muscle fibers and strengthening of the muscles. 6
Methodology
Study design and population
This is a case series of five children diagnosed with myelomeningocele undergoing physiotherapy sessions three times a week for a total of 24 sessions. The patients were selected based on their diagnosis and their willingness to participate in the study. The study took place between March and April 2022 at the Leyaqa Physical Therapy Center, Qatif, Saudi Arabia. This study was reviewed and approved by the Research Ethics Committee at Security Forces Hospital Program-Makkah. The approval number is ECM#0534-127882. The approval number is 0534-127882. This study was conducted according to the Declaration of Helsinki. Written informed consent was obtained from a legally authorized representative(s) for anonymized patients’ information to be published in this article.
All included children were clinically stable, and they continued their physiotherapy as planned by their healthcare provider with no additional interventions in their daily living routines.
Data collection
The children’s parents or guardians were asked to complete a questionnaire to evaluate the children’s basic bowel and bladder function before starting the electrical therapy and the 24th session of electrical therapy. In addition, 3 months of post-therapy evaluation was reported. The physiotherapy program consisted of lower extremities strengthening and stretching, weight bearing, and upper extremity strengthening exercises. Electrical stimulation applied in prone for FES using four electrodes, two on the sacrum and two on the abdomen, as shown in Figure 2. FES was applied for 30 min in each session. The participants were positioned in supine lying position with two electrodes in the groin areas for NMES, as shown in Figure 3. NMES was applied for 30 min in each session.
Data analysis
The means of pre- and post-assessments were calculated for comparisons. The means before and after assessment were assigned numerical values according to specific response categories (Never = 1, Most of the time = 4). The mean for each question was calculated and then compared using a two-sample t-test assuming equal variances.
Results
Five patients (mean age 8.4 ± 4.3 years) were recruited. The majority were male patients (n = 3). All patients had complete motor dysfunction with loss of sensation/on diaper. Of the five included children, three had a ventriculoperitoneal (VIP) shunt (Table 1).
Summary of all children included in this case series.

VIP: Ventriculoperitoneal.
All parents and guardians completed pre- and post-treatment questionnaires. The pre-treatment questionnaire responses confirmed that all children had never had control over emptying their bladders or bowels, nor were they able to completely empty their bladders or bowels at once. Four children never felt the urge to empty their bladders or bowels, and four children reported constipation at most times (Table 2).
Summary of pre-treatment questionnaire responses.

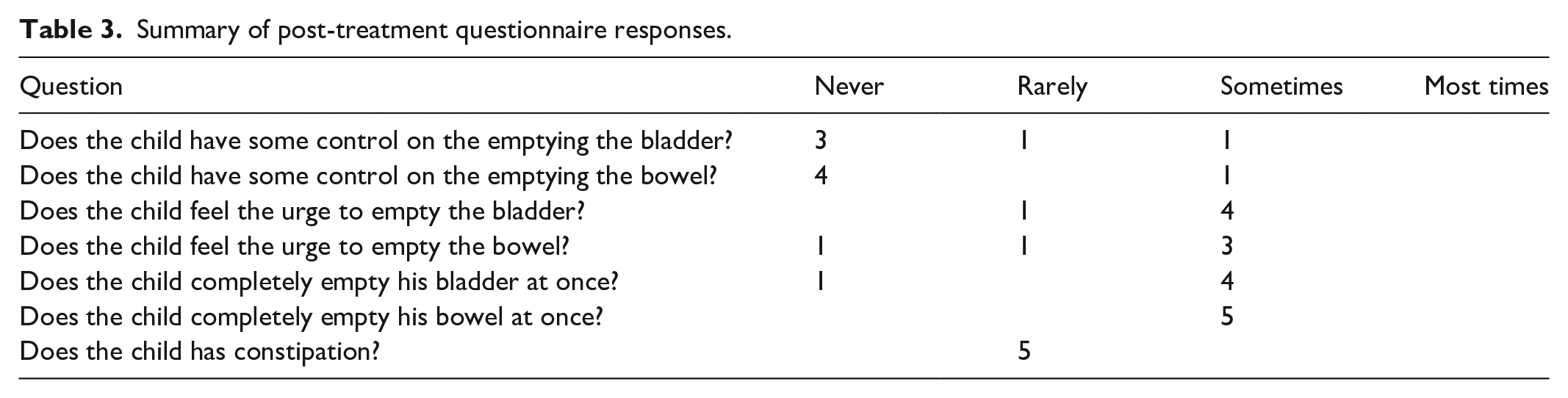
In the post-treatment questionnaire, parents of two children reported some improvement in their children’s control of emptying their bladders, one child had improvement in emptying their bowel, four children reported improvement in feeling the urge to empty their bladder, three children reported improvement in feeling the urge to empty their bowel, four children were able to empty their bladders all at once, and all five children were able to completely empty their bowels all at once. Finally, all five children rarely had constipation after the treatment (Table 3) (Figure 1).
Summary of post-treatment questionnaire responses.

Improvement reported by parents of children with spina bifida aperta with myelomeningocele after combined faradic electrical stimulation and neuromuscular electrical stimulation treatments.
Case presentations
Case #1
A 4-year-old male patient presented with complete motor and sensory dysfunction of both bladder and bowel; therefore, he was diaper dependent and had occasional constipation. He was a buttock scooter with independent floor mobility and wore static ankle foot orthoses (AFOs) during the day only. For outdoor mobility, the mother used a pushchair. He underwent physical therapy three times a week, with no schooling activities. After the intervention, he told his mother that he was emptying his bladder in the diaper sometimes, but not his bowel. He expressed a feeling of the urge to empty the bladder on rare occasions but not the bowel. As further improvement, he sometimes completely emptied his bladder and bowel at once and rarely had constipation.
Case #2
A 6-year-old male presented with complete motor and sensory dysfunction of both the bladder and bowel. He had also undergone a VIP shunt in the first month after birth, secondary to congenital hydrocephalus. He was a primary school student, diaper dependent, and used a walker for mobility at home and school, together with static AFOs. He also had regular physical therapy visits three times a week. Before the intervention, he never had control of emptying his bladder or bowel, but he felt the urge to empty his bladder and bowel on rare occasions. He also had constipation most of the time. After the intervention, he sometimes felt the urge to empty his bladder and bowel. As further improvement, he sometimes completely emptied his bladder and bowel at once and rarely had constipation.
Case #3
A 7-year-old male presented with complete motor and sensory dysfunction of both the bladder and bowel; therefore, he was diaper dependent at all times. He also had constipation most of the time. At birth, he was diagnosed with hydrocephalus; therefore, he underwent a VIP shunt in the first month after birth, and it was revised at the age of 3 years due to shunt malfunction. He was exercised ambulant with a postural walker and AFOs during physical therapy visits three times a week. At home, he moved around by rolling over on the floor. He had constipation most of the time. After the intervention, he showed improvement in the feeling of the urge to empty his bladder sometimes, but rarely the bowel. He was able to empty both his bladder and bowel at once, sometimes. His mother stated that he rarely had constipation after the intervention.
Case #4
A 10-year-old female patient presented with complete motor and sensory dysfunction of both bladder and bowel; therefore, she was also diaper dependent at all times and had constipation most times. In addition, she suffered from hydrocephalus and underwent a VIP shunt within 1 month after birth. She was a primary school student, wheelchair dependent, and attended physical therapy three times a week. After the intervention, she showed improvement in the feeling of the urge to empty her bladder and bowel sometimes. She was able to empty both her bladder and bowel at once sometimes and rarely had constipation.
Case #5
A 15-year-old female patient presented with complete motor and sensory dysfunction of both her bladder and bowel; therefore, she was diaper dependent at all times. She also had hydrocephalus; therefore, she underwent a VIP shunt in the first month of her life. She was in intermediate regular school, wheelchair dependent, and overweight. She was exercise-ambulant using an elbow support walker, and unlike the other cases, she wore a ground-reaction ankle foot orthosis. After the intervention, she was able to control the emptying of her bladder for a short period on rare occasions and was able to control her bowel at school sometimes. She also showed improvement in the feeling of the urge to empty her bladder and bowel sometimes. She was able to empty her bowel at once sometimes, but never her bladder. She stated that she rarely had constipation after the intervention.
All the participants remained diaper dependent even after the intervention.
Discussion
During faradic stimulation, we placed four electrodes on the pelvic area and at the bottom of the abdomen to stimulate the sacral nerve, which supplies both the bowel and bladder, as shown in Figure 2. The electrical stimulation lasted for 20 min at low intensity for all children. Faradic stimulation was also conducted over the level of S2–S4 to stimulate the pelvic nerve, which is responsible for the contraction of the detrusor muscle to stimulate active micturition. It also stimulates the external sphincter of the ureter to provide voluntary control over micturition. 7
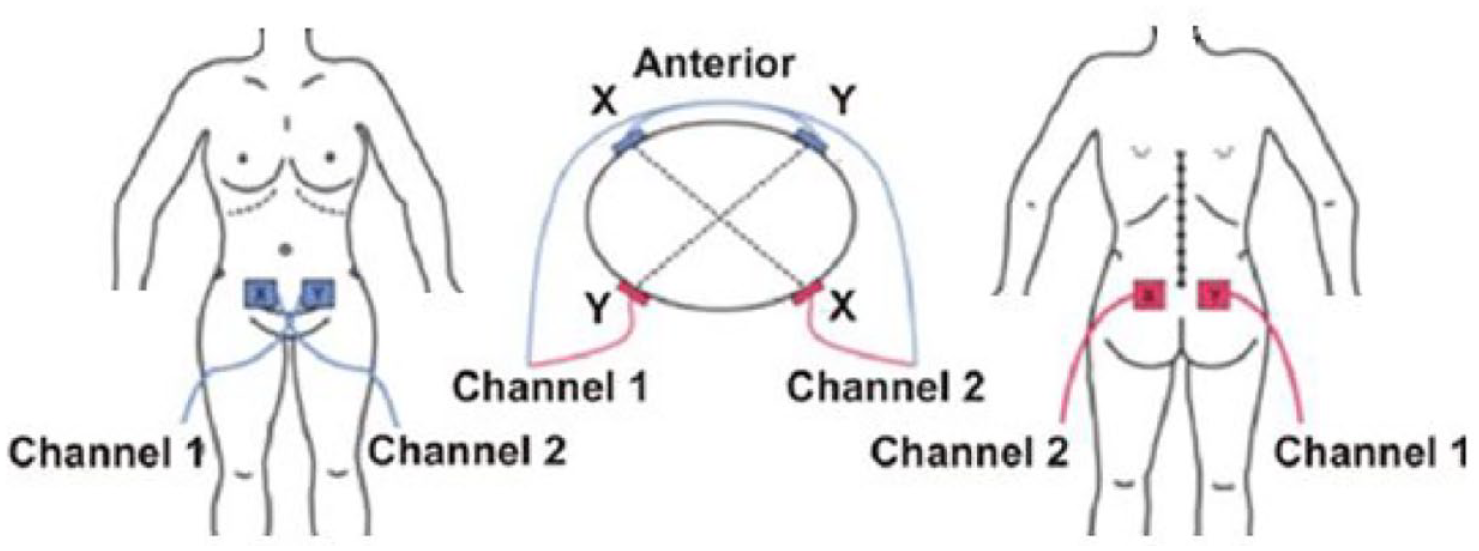
Electrode placement during faradic stimulation.
Faradic current stimulated the nerves, which in turn led the inverted muscle to contract. The procedure is fairly safe and does not cause irritation when used with caution and avoiding high intensity. In faradic current, high chemical formation should not be performed to avoid the serious danger of burns because of the short duration of the impulses and the biphasic administration. Faradic current is a short-duration interrupted direct current with a pulse duration ranging from 0.1 to 1 millisecond (MS) at a frequency of 50–100 Hertz (Hz). Faradic current is surged to produce tetanic contraction and relaxation of the muscle. The parameters of faradic stimulation are biphasic, asymmetrical, unbalanced, and spiked. The technique of application was to stimulate a group of muscles by stationary stimulation in which the active electrode and passive electrode were kept stationary.
In addition to conducting the faradic electrical nerve stimulation, we provided each parent with a portable NMES unit to be used once a day at home. The parents received sufficient training in how to apply NMES at home effectively and safely. NMES stimulates the pelvic floor muscles, which in these types of patients are atrophied because of disuse (Figure 3).
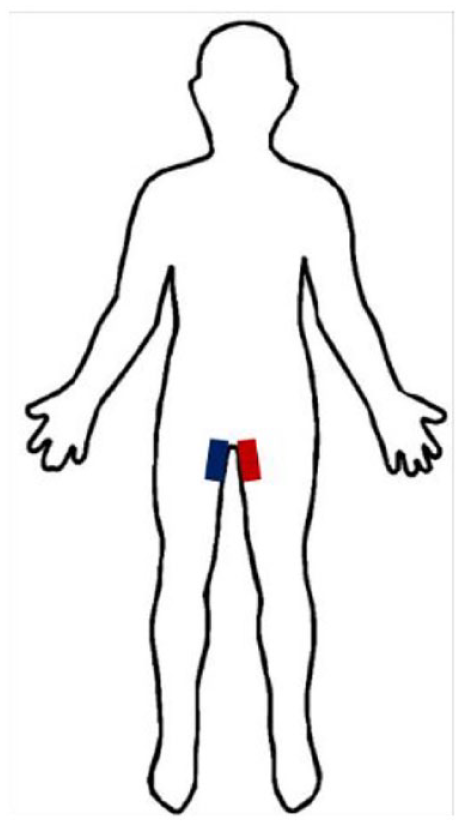
Placement of neuromuscular electrical stimulation to stimulate pelvic floor muscles at home.
All the children and parents were very compliant during the study. No complications or skin allergies were noticed. All children felt improved sensations from the first five sessions. The parents were very happy because their children started to feel the urge to empty both bladder and bowel most times. Case #5, who already had a weak feeling of the urge and had some feeling of emptying her bowel, could hold herself from emptying in the diaper during school most days, which reflected positively on her self-esteem. All children remained in diapers even after the improvement because their motor control was still the same. Case #1 reported that he felt the urge to urinate, and he could urinate completely and actively sometimes. After 3 months, we contacted the parents of all children and asked them to fill in the questionnaire again. The results were the same.
Conclusion
Although many studies in the literature have shown the positive impacts of using electrical simulation to improve bowel and bladder functions in patients with myelomeningocele, to our knowledge, this is the first case that combines both FES and NMES techniques and exhibits a significant impact.
In the present study, sacral nerve stimulation using faradic nerve stimulation in combination with NMES on pelvic floor muscles showed a positive result in terms of fecal and urine incontinence and it can be offered with benefits according to the series of cases studied. Extending this combination therapy to a minimum of 6 months should produce even better results. Unfortunately, none of the participants in the present study were willing to extend their therapy beyond 3 months. This study also highlights the necessity of using a high-technology intervention, such as implanting an electrode near each branch of the sacral nerve for more effective electrotherapy to improve bowel and bladder function in these children. A comprehensive nerve study for the bowel and bladder should be a routine checkup in the first year of their lives to establish a baseline matrix of the function and how early the intervention therapy should start in their lives to allow for greater neuroplasticity.
In conclusion, a combination of FES and NMES electrotherapy might be an effective way to improve the bladder and bowel functions of patients with myelomeningocele and might be offered as a treatment option to them.
Footnotes
Acknowledgements
The author extends her gratitude to Leyaqa Physical Therapy Center management and their supportive team. In addition, the author is very thankful to her colleagues for their adherence to the intervention and for collecting feedback from the patients’ parents. She is especially grateful to PT Abdulaziz Z. Alshahrani for his fruitful advice and consultation in preparing this manuscript.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was reviewed and approved by the Research Ethics Committee at Security Forces Hospital Program – Makkah. The approval number is ECM#0534-127882. This study was conducted according to the Declaration of Helsinki.
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patients’ information to be published in this article