
Abstract
The aim of this case study is to report how treatment and rehabilitation for meniscus tears can exacerbate the underlying condition or improve function. In addition, the objective of the study is to compare quadriceps physical therapy in a patient to gluteal muscle therapy. There are different types of meniscus tears, and each rehabilitation plan depends on the location and type of meniscus injury. Treatment options include conservative, nonsurgical therapy and surgical repair or replacement therapy. Typically, strengthening the quad muscles is the focus of physiotherapy. Few studies have assessed the role of the gluteal muscles, rather than the quad muscles, in improving the patient’s situation. The patient, a 32-year-old female, reported experiencing sharp pain in her right knee, a swollen knee, and joint line tenderness, following an incident involving carrying an unbalanced load. Magnetic resonance imaging confirmed the presence of a meniscal tear in the right knee. The patient received quadriceps physical therapy, which resulted in worsening of the knee joint and loss of mobility. Subsequently, she received (gluteal muscle) therapy, which resulted in restoration of mobility, improved range of motion, and recovery from joint line tenderness. The patient was able to walk again without pain. Gluteal muscles play a key role in stabilizing the pelvis and maintaining proper alignment of the hips and knees. They help with movements such as walking, running, and jumping, and strong gluteal muscles reduce the risk of injuries, like knee valgus.
Introduction
The medial meniscus is “C shaped” and primarily attached to the tibia and femur. The meniscus acts as a shock absorber for the knee. 1 Meniscal tears represent one of the most common injuries in sports. 1 Among knee joint injuries in athletes, 24% are medial meniscus tears, 8% are lateral meniscus tears, and 20%–30% of ligament injuries are associated with meniscal tears. 1 The mean incidence of meniscal injuries is as high as 60–70/100,000 knee injuries. 2 There are different types of meniscal tears: longitudinal tears, bucket-handle lesions, flap tears, radial tears, and ramp lesions, as well as more complex lesions involving several mechanisms. Horizontal tears are a type of longitudinal tear that occurs alongside the upper part of the tibia and affects one of the surfaces or edges of the joint. 1
There are several surgical and rehabilitation treatments depending on the type and severity of the meniscal tear. 1 Meniscal tears can be treated conservatively with ice, application of heating pads, compression, bandages, and anti-inflammatory drugs, or can be treated surgically with repair or replacement, with removal considered a suboptimal option. 1 Physical therapy is a typical component of either conservative or post-surgical treatment. It plays a vital role in pain management, restoring function, and improving overall quality of life.
Previously, meniscectomy or partial meniscectomy was one of the most common surgeries. However, research shows that the meniscus has a crucial role in knee joint stability, and removal increases the risk of early osteoarthritis. Therefore, preserving the meniscus or repairing meniscal tears should always be prioritized. 2
According to Chirichella et al., the rehabilitation program should focus on managing swelling, controlling range of motion, and strengthening the quadriceps and hamstring muscles. 2 However, randomized controlled trials comparing physical therapy to rest and time for nonsurgical treatment of meniscus tears are lacking. Siemieniuk et al. recommended therapy aimed at strengthening gluteal muscles (GMs) for patients at risk of osteoarthritis who had grade 1 or lower meniscal tears or had tears caused by degeneration. 3
Examples of non-weight bearing exercises to increase the strength of the GMs, including but not limited to clamshells, single leg bridge, side leg raise in hip extension, bilateral glute bridge, side plank with abduction, and bird dog exercise. 4 Here, we present a case study that supports therapy to strengthen GMs.
Case
A 32-year-old female presented to the emergency room for severe pain in the right knee with medial tenderness. The patient reported that the injury was obtained from a sharp twist while carrying an unbalanced load. She did not have any history of knee injury or other joint issues. The patient was unable to move the right knee or bear weight on it. Movements involving the knee (walking, squatting, kneeling, and stair ambulation) were painful. The flexion McMurray test was positive. 5 Magnetic resonance imaging was done; long repetition time—axial, sagittal, and coronal—images of the right knee were obtained. The results reflected a horizontal tear (grade 1) within the posterior horn of the medial meniscus without meniscal extrusion or perimeniscal cyst (Figures 1(a) and 1(b) and 2(a) and 2(b)). The fluid reflected no joint effusion; however, a small Baker’s cyst without signs of rupture was visible. Lateral deviation of the patella on full knee extension, along with a mildly increased tibial tuberosity to trochlear groove distance compared to the contralateral side, raised the possibility of patellar instability.

Horizontal tear within the posterior horn of the medial meniscus: (a) and (b). The red arrows indicate a horizontal tear (Grade 1) within the posterior horn of the medial meniscus.
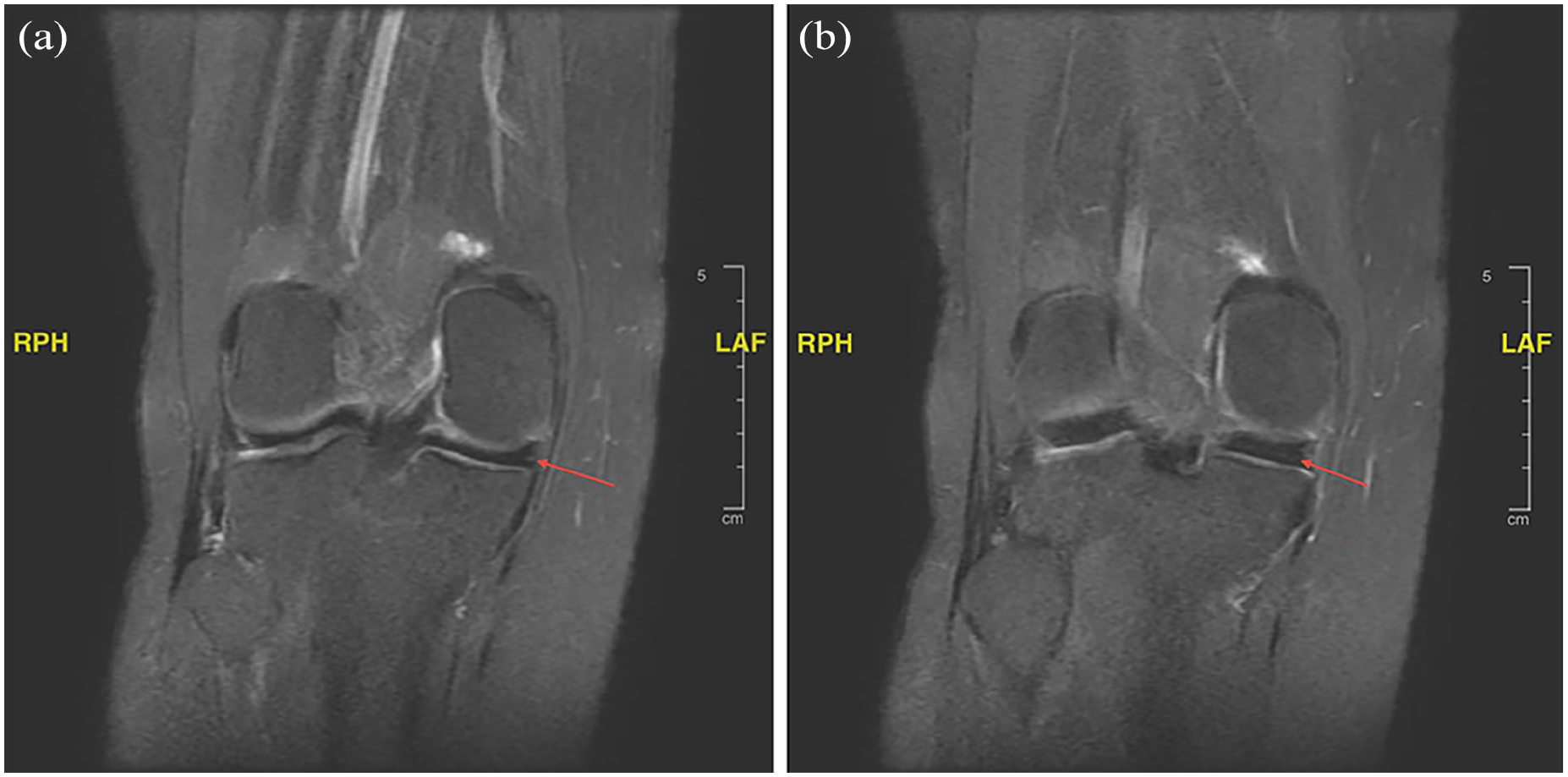
Coronal images of horizontal tear: (a) and (b). The red arrows indicate a Grade 1 horizontal tear within the posterior horn of the medial meniscus.
The recommended treatment plan was physiotherapy to decrease pain, swelling, and tenderness, and to increase range of motion and the strength of the vastus medialis oblique muscles. Also, the patient was advised to follow the Rest, Ice, Compression, Elevation protocol and to avoid prolonged walking or standing. Because her work in an administrative office required extended periods (10 h/day) of sitting with bent knees, she was recommended to be on light duty for 2 months.
This report tracks the patient’s progress over a 12-month period, from the time of injury to the restoration of movement.
Discussion
The patient received supervised rehabilitation treatment in a center in Riyadh, Saudi Arabia. The exercises focused on (i) intensive muscle strengthening, particularly of the quadriceps femoris muscles, (ii) balancing exercises, and (iii) increasing the range of motion. She also received heat and cold therapy, along with continuous ultrasound to increase the blood supply in the healing tissue.
During the first week, the patient received therapy 3 days/week, and she was requested to perform the same exercises at home. The physical therapist used cold and hot therapy, 30 repetitions of stretches, a transcutaneous electrical nerve stimulation machine, ultrasound, and strapping with kinesiology tape.
During the second week, the patient received therapy three times. More complex muscle strengthening exercises were undertaken, such as a pillow squeeze, seated leg extension, heel slide, straight leg raises (all sides), quad activation, toe raises, wall sits, and hamstring curls. Amino neuro frequency discs were also applied.
During the third week, the patient’s medical condition worsened, prompting the introduction of anti-inflammatory medications to manage the pain. In addition, 14 days of rest were scheduled with no supervised therapy or at-home exercises.
For the fourth week, hydrotherapy exercises were introduced to reduce inflammation. The exercises focused on the quadriceps femoris (quad muscles) and included pool leg raises, aquatic bicycle, single leg balance, squats, pool walking, and straight leg raises with the use of elastic resistance bands in the pool.
Whenever medium-to-advanced exercises were introduced, the patient would regress, experiencing pain and inflammation in the knee. This regression occurred after receiving therapy at three centers. Each center focused on strengthening the quad muscles.
The patient received surgical consultation from seven doctors. Surgery was not recommended. All advised her to continue with intensive physical therapy. Upon continued physical therapy, the patient experienced severe pain whenever she attempted to walk. Ultimately, her condition worsened, and she required a wheelchair or crutches to alleviate the pain of walking.
The patient visited a physical therapist in the United States and was diagnosed with probable nerve irritation (ICD 10: M79.2 unspecified neuralgia and neuritis). Physical therapy targeting the other issues in her leg, a meniscus tear, hip discomfort, sciatica, patellar misalignment, and knee cartilage inflammation, failed to resolve the nerve irritation.
Lumbar extension rotation syndrome and hip anterior glide medial rotation syndrome are two muscle imbalances that can cause hip discomfort, sciatica, patellar misalignment, and knee cartilage inflammation. 6 Although the patient made progress in her multiple attempts to address these two muscle imbalances, the unresolved nerve irritation hampered progress. To effectively treat the nerve irritation, the amount of treatment aimed at correcting the muscle imbalances had to be reduced.
The new physical therapy plan was tailored to emphasize the GMs, incorporating exercises such as standing glute squeezes, standing glute burners, standing baby-squat holds, and mini-bridges over a 6-month period. The objective of the new 6-month plan was to strengthen the GMs, thereby balancing the strength between the GM and quad muscle. Month 1 focused on glute squeezes, tailgate swings, and standing abdominal curls. Month 2 continued with the same exercises started in month 1, with increasing repetitions and introduced mini-bridges. Months 3 and 4 again increased repetitions of the existing exercises and added the following new exercises: toe curls, arch raises, intermediate-level mini-bridges, and standing baby-squat holds. Months 5 and 6 maintained the previous exercises and introduced clam exercises and standing glute burners to target the same muscle groups.
By the end of the 6-month exercise regimen, range of motion improved greatly, and joint line tenderness was negative. The patient was able to walk without pain.
GMs play an essential role in maintaining a correct knee position and preventing knee valgus during movements such as walking, running, jumping, and landing. 7 The gluteus medius and maximus, in particular, are crucial for stabilizing the hip and keeping the femur aligned during these movements, thereby maintaining the knee’s position in the coronal plane, preventing inward collapse (valgus) and reducing the risk of injury.
Conclusion
This case study shows that the wrong physiotherapy plan, focusing on intensive physical therapy and quad muscle strengthening, failed to resolve a knee joint issue related to a meniscal tear. Consequently, the nerves remained in a state of irritation even with normal activities such as walking and sitting in typical positions. In this case, the patient required a conservative and rehabilitation approach focused on GM strengthening.
Footnotes
Ethical considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent to participate
The author certifies that she has obtained all appropriate patient consent forms. The patient understands that his/her names and initials will not be published and due efforts will be made to conceal their identity.
Consent for publication
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Author contributions
AA wrote the abstract, introduction, case, management and outcome, and conclusion.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.