
Abstract
Tuberculosis is a multi-system disease, but paranasal sinuses involvement is uncommon, and most cases occur secondary to pulmonary tuberculosis. Tuberculous granuloma of the paranasal sinuses is rare and only a few cases are reported. Due to non-specific ways of clinical presentations, diagnosis of paranasal tuberculosis can be missed, delayed or confused with other entities like malignancy. We present an uncommon case of tuberculous granuloma of the left maxillary antrum and ethmoid sinus in a 56-year-old man which mimicked trigeminal neuralgia and malignancy. Medial maxillectomy and anterior ethmoidectomy with clearance of the lesion followed by antituberculous treatment prevented permanent loss of his vision. Depending on the chief complaints, patients may present to various specialties. Early cross-referral is important for early diagnosis, appropriate management and prevention of complications.
Introduction
Tuberculosis, a multi-system disease, is still a major health problem in most parts of the developing world. Pulmonary tuberculosis is the most common form of primary tuberculosis, although primary tuberculosis can occur at any other sites. Involvement of the paranasal sinuses is rare 1 due to the protective functions of the sinonasal mucosa. 2 Most of the cases of paranasal sinus tuberculosis occur secondary to pulmonary tuberculosis.2,3 Tuberculous granuloma of paranasal sinuses is uncommon and only a few cases are reported. Paranasal tuberculosis remains asymptomatic until well-advanced 3 and presents with non-specific symptoms and signs mimicking other clinical conditions. Patients may present with various symptoms like nasal obstruction, nasal discharge,1,4 epistaxis,1,3 facial swelling,1,2 postnasal drip, hyposmia, headache, 4 ulceration at the nasal vestibule, 5 drooping of eyelid, facial numbness, 6 eye discharge, 7 proptosis,7,8 reduced vision 9 or loosening of teeth. 10 Due to its non-specific clinical presentations, there is diagnostic dilemma and therapeutic delay. 2 Maxillary sinus tuberculosis resembles other granulomatous or neoplastic diseases 1 and remains an under-diagnosed entity.1,2 We are reporting an unusual case of tuberculous granuloma of maxillary antrum and ethmoid sinus presenting with clinical pictures suggestive of malignancy.
Case report
A 56-year-old man who was previously healthy presented with a history of episodic pain and numbness over the left cheek for a month followed by inability to open mouth fully for a week. He also complained of left eye swelling with drooping of eyelid and reduced vision for 1 week. He initially visited a general practitioner for his pain and later consulted a neurosurgeon as his symptoms got worsened. He was treated for left trigeminal neuralgia by the neurosurgeon and then referred to us to evaluate further for his cheek pain and numbness. He did not have nasal blockage, rhinorrhoea, epistaxis, anosmia or constitutional symptoms like fever, loss of appetite and loss of weight. He did not have a previous infection with tuberculosis and could not recall any contact history. There was no history of nasal or sinus surgery. On examination, he had severe trismus with just a finger breadth of mouth opening. Perception to light touch was impaired on his left cheek at V2 (maxillary division) region. There was mild proptosis and ptosis of his left eye; however, eye movements were normal and full range. Other cranial nerve examinations were normal. There was no obvious swelling on his left cheek or facial asymmetry except for the mild proptosis and ptosis. Neck examination revealed no palpable lymph nodes. Anterior and posterior rhinoscopic examinations did not reveal any sinus pathology and other physical examinations were normal.
Blood investigation showed white blood cell (WBC) 10.9 × 103/dL, and differential counts were normal. Erythrocyte sedimentation rate (ESR) was 9 mm in the first hour. Blood for anti-HIV was non-reactive. Sputum for AFB × 3 was negative. Chest X-ray did not reveal any lung pathology. CT (computed tomography) scan of the paranasal sinuses showed soft tissue lesion in the left anterior ethmoid sinus and maxillary antrum (Figure 1) with erosions of the medial and lateral walls of the maxillary sinus.

Soft tissue lesion in the left maxillary antrum (black arrow).
The lesion was extending into the inferomedial aspect of the left orbit displacing the orbit anteriorly (Figure 2). Malignancy in the maxillary antrum involving the anterior ethmoid and orbit was our initial impression.

Soft tissue lesion extending into the inferomedial aspect of the left orbit displacing the globe anteriorly (white arrow).
Endoscopic left medial maxillectomy and anterior ethmoidectomy was performed which revealed soft fluffy and necrotic mass at the left maxillary antrum and ethmoidal cells with a bit of pus. The mass was cleared off and sent for histopathological examination and acid-fast bacilli. Histopathological examination was reported as necrotic tissue composed of reactive multinucleated giant cells, many of Langhan’s type and aggregates of epithelioid histiocytes admixed with a predominantly chronic inflammatory infiltrate forming coalescent granuloma compatible with tuberculous granuloma (Figure 3(a)–(c)).
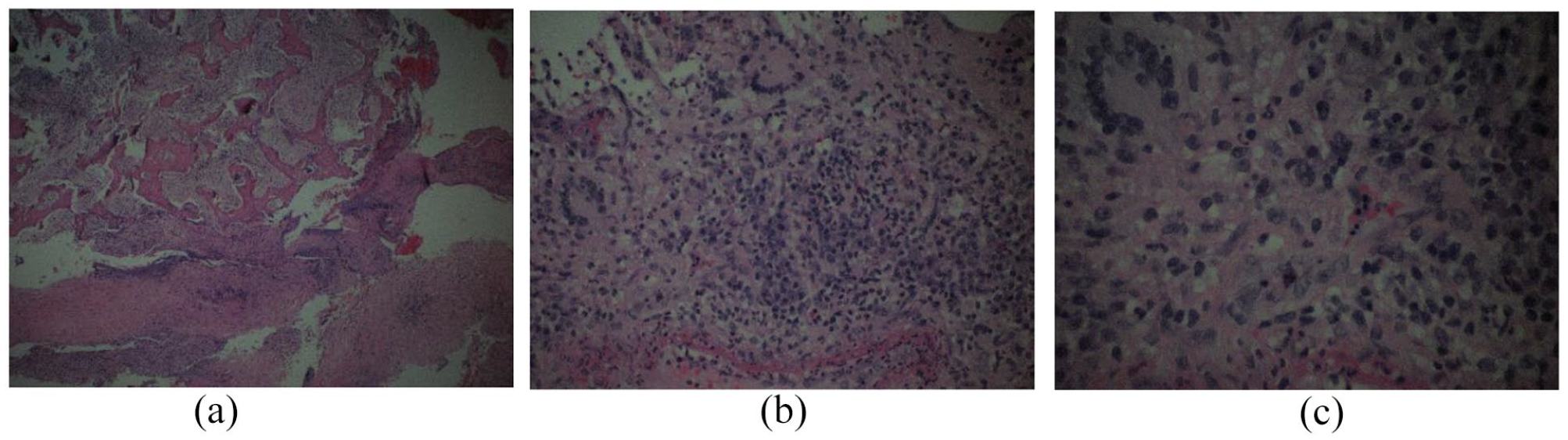
(a) HPE showing tuberculous granuloma (H&E stain ×10). (b) HPE showing multinucleated giant cells, many of Langhan’s type and aggregates of epithelioid histiocytes (H&E stain ×20). (c) HPE showing multinucleated giant cells, many of Langhan’s type and aggregates of epithelioid histiocytes (H&E stain ×40).
No AFB or fungi were detected on special stains and no malignant cells were seen. We diagnosed him as a case of tuberculous granuloma of left maxillary and ethmoid sinus involving the orbit. The patient was started on a 6-month course of standard antituberculous treatment (ATT), that is, isoniazid, rifampicin, pyrazinamide and ethambutol for 2 months in the intensive phase and isoniazid and rifampicin for 4 months in the continuation phase. His trismus improved to two fingers breath on post-operative day 3 and almost normal by 2 weeks. His left eye vision also improved from 6/30 preoperatively to 6/18 on post-operative day 7. He was doing well on follow-up at 6 months and nasal endoscopy was clear.
Discussion
Tuberculosis is an infectious disease caused by intracellular acid-fast bacillus demonstrated by Ziehl–Neelsen Stain. 11 It is a multi-systemic disease with varied clinical presentation and manifestation. It is still a major public health problem in most parts of the developing world and resurgence of tuberculosis due to the HIV epidemic world-wide and the increasing prevalence of multi-drug resistant tuberculosis is a challenge we are facing today. Tuberculosis of the paranasal sinuses and particularly tuberculous granuloma of sinuses is very rare. Out of paranasal sinuses, maxillary and ethmoid sinuses are most commonly affected by tuberculosis.6,9 Involvement of unusual sites leads to under-diagnosis of extra-pulmonary disease, although incidence of extra-pulmonary tuberculosis is on the rise in many regions of the world. 12
Most common presentations of the previous reported cases of the sinonasal tuberculosis are nasal obstruction, nasal discharge and epistaxis.1,3–5,8,11–20 However, our patient did not have these common presentations and has initially presented with pain and numbness over the left cheek for which he was treated for trigeminal neuralgia. Later, he developed trismus and proptosis and had reduced vision on the affected side. Only a few previously reported cases of tuberculosis involving the sinuses have presented with proptosis5,7,8 and none to our knowledge has presented with trismus. Initial inflammation in the sinus and the granuloma could have irritated the trigeminal nerve causing significant pain and numbness over the cheek, and also the trismus. Features on CT scan with the lesion spreading into the orbit and erosion of maxillary walls led us to think of malignancy as our most possible diagnosis. Tuberculous granuloma and other granulomatous conditions were the last thing on our mind at that time. It was only after the histopathological examination report of the lesion that the diagnosis of tuberculous granuloma was made. Surprisingly, ESR was only 9 mm in the first hour which is usually very high in tuberculosis. We noticed that most of the cases reported in our literature review have ESR less than 50 mm in the first hour.3,5,7–9,12,15,16,18–20 However, there are reported cases of tuberculous granuloma of the sinuses with ESR within the normal ranges.7,20 The chest X-ray of our case was clear and sputum for acid-fast bacilli was also negative which to certain extent can exclude primary infection in the lungs. However, we could not exclude pulmonary tuberculosis beyond doubt as we could not do other investigations like CBNAAT (cartridge-based nucleic acid amplification test)/GeneXpert, serological test for immunoglobulin M (IgM), TB culture and bronchoalveolar lavage. Fungal infection was unlikely as fungal elements on special stain were not detected in the specimen, although this cannot exclude other granulomatous conditions. In our case, AFB was not detected in the granuloma. Like in our case, many previously reported cases of the sinonasal tuberculosis have also not detected AFB in the specimen5,11–13,16,17 and have diagnosed as tuberculosis based on histopathological examination. We believe that AFB is not necessarily seen or detected in a tuberculous granuloma. Our case responded well to surgical debridement and anti-tubercular medication, with improvement of trismus and vision which supported our final diagnosis.
Conclusion
Tuberculous of the paranasal sinuses is uncommon, but it should be a differential diagnosis in cases not responding to conventional treatment. It may mimic malignancies of the sinuses and trigeminal neuralgia. Depending on the chief complaint, a patient may present to various specialties. Cross referral without delay is imperative for early diagnosis and treatment to prevent complications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for his anonymised information to be published in this article.