
Abstract
Rosai–Dorfman disease is a rare non-Langerhans cell histiocytosis disorder, also known as sinus histiocytosis, with massive lymphadenopathy. Rosai–Dorfman disease is classified into nodal and extranodal diseases. Ocular involvement is one of the common extranodal manifestations; however, uveitis manifestation is infrequent. We reported an interesting Rosai–Dorfman disease patient who presented with chronic bilateral granulomatous anterior uveitis with disc hyperemia and cystoid macular edema. She was a 60-year-old Thai female who had abnormal skin nodules on her back after multiple recurrent chronic anterior uveitis. The diagnosis has been made based on a constellation of the patient’s information, physical examination, and histopathological results. We successfully treated the patient with topical steroids, posterior subtenon triamcinolone 20-mg injection, and methotrexate.
Keywords
Introduction
Rosai–Dorfman disease (RDD) is a rare and benign disease characterized by abnormal proliferation and accumulation of non-Langerhans cell histiocytes in the body. The RDD was first described in 1969 by Rosai and Dorfman as a novel disease of painless cervical lymphadenopathy.1,2 It can be classified into two types: nodal and extranodal diseases, with different signs and symptoms varied by the specific involved body area. 3
Ophthalmic manifestation is one of the most common extranodal manifestations, accounting for 10.5% of cases, and the orbit is the most affected part.3–5 An orbital mass and epibulbar mass were commonly reported presentations.4–7 An intraocular involvement of RDD is exquisitely rare, but it tends to have more aggressive characters and multiple organ involvement. 4 Most reported cases presented with mass lesions, such as ciliary body mass and choroidal mass.6,8–10
To the best of our knowledge, it was unusual for RDD to be associated with uveitis.6,8,11,12 Our case is an extranodal RDD with cutaneous nodules and refractory bilateral chronic anterior uveitis complicated with cystoid macular edema (CME) and hyperemic disc, which was successfully treated with posterior subtenon (PST) triamcinolone injection and methotrexate (MTX).
Case presentation
A 60-year-old Thai female presented with a history of refractory chronic anterior uveitis in both eyes, which was intermittently treated elsewhere with topical steroids for years. She presented to us after having had a new onset of photophobia and blurred vision in both eyes for a couple of days. A review of the system was positive for well-controlled essential hypertension and type 2 diabetes mellitus (DM) with moderate nonproliferative diabetic retinopathy (NPDR). Numerous painless skin nodules were noticed on the back by herself for several weeks (Figure 1). Eye examination revealed visual acuity of 20/32 in the right eye (OD) and 20/40 in the left eye (OS), and intraocular pressure was 10 mmHg in both eyes. There were grade 2+ anterior chamber cells with diffuse stellate and mutton-fat keratic precipitates in both eyes, notably more in the right eye. A dilated fundus examination showed a bilateral hyperemic optic disc, slightly more pronounced in the left eye. There were scatter dot/blot hemorrhages with no exudation, vitritis, vasculitis, or retinitis (Figure 2). Interestingly, marked CME with prominence in the inner retinal layers was found in both eyes with a central foveal thickness of 295, 297 µm on optical coherence tomography (OCT) (Carl Zeiss Meditec, INC, Dublin, CA, USA) (Figure 3(a) and (b)). Fluorescein angiography (FA) (Kowa VX10i, Japan) revealed normal retinal and choroidal filling with optic disc hyperfluorescence and mild leakage. A foveal hyperfluorescent in petaloid leakage was also detected in both eyes. All detected microaneurysms on FA were present only in the extrafoveal area. The diagnosis of moderate diabetic retinopathy and bilateral chronic granulomatous anterior uveitis (CAU) with CME and disc hyperemia was made. Extensive investigations were initiated, and it was found to have nonreactive Venereal Disease Research Laboratory (VDRL) test, nonreactive Treponema pallidum Themagglutination assay (TPHA) test, nonreactive anti-HIV, an inconclusive test of Quantiferon gold for tuberculosis (Nil 0.02, TB1 Ag 0.02, TB2 Ag 0.02, Mitogen 0.02), and a normal chest X-ray. We made a dermatologic consultation, and a skin biopsy of the nodules at the back was performed. The pathological result showed abnormal granulomatous infiltration and emperipolesis (Figure 4(a)). The immunohistochemical study demonstrated the presence of CD68 positive, S100 positive, and CD1a negative (Figure 4(b)–(d)), which was consistent with the diagnosis of RDD. Further systemic investigations for RDD were performed, including computed tomography of the chest and abdomen and magnetic resonance imaging of the brain, which were all unremarkable.

Numerous skin nodules discrete at the back.

Photofundus of the right and left eye.

Optical coherence tomography (OCT). (a) Initial presentation of OCT demonstrated cystoid macular edema of the right eye. (b) Initial presentation of OCT demonstrated cystoid macular edema of the left eye. (c) After treatment, OCT demonstrated resolution of cystoid macular edema of the right eye. (d) After treatment, OCT demonstrated resolution of cystoid macular edema of the left eye.
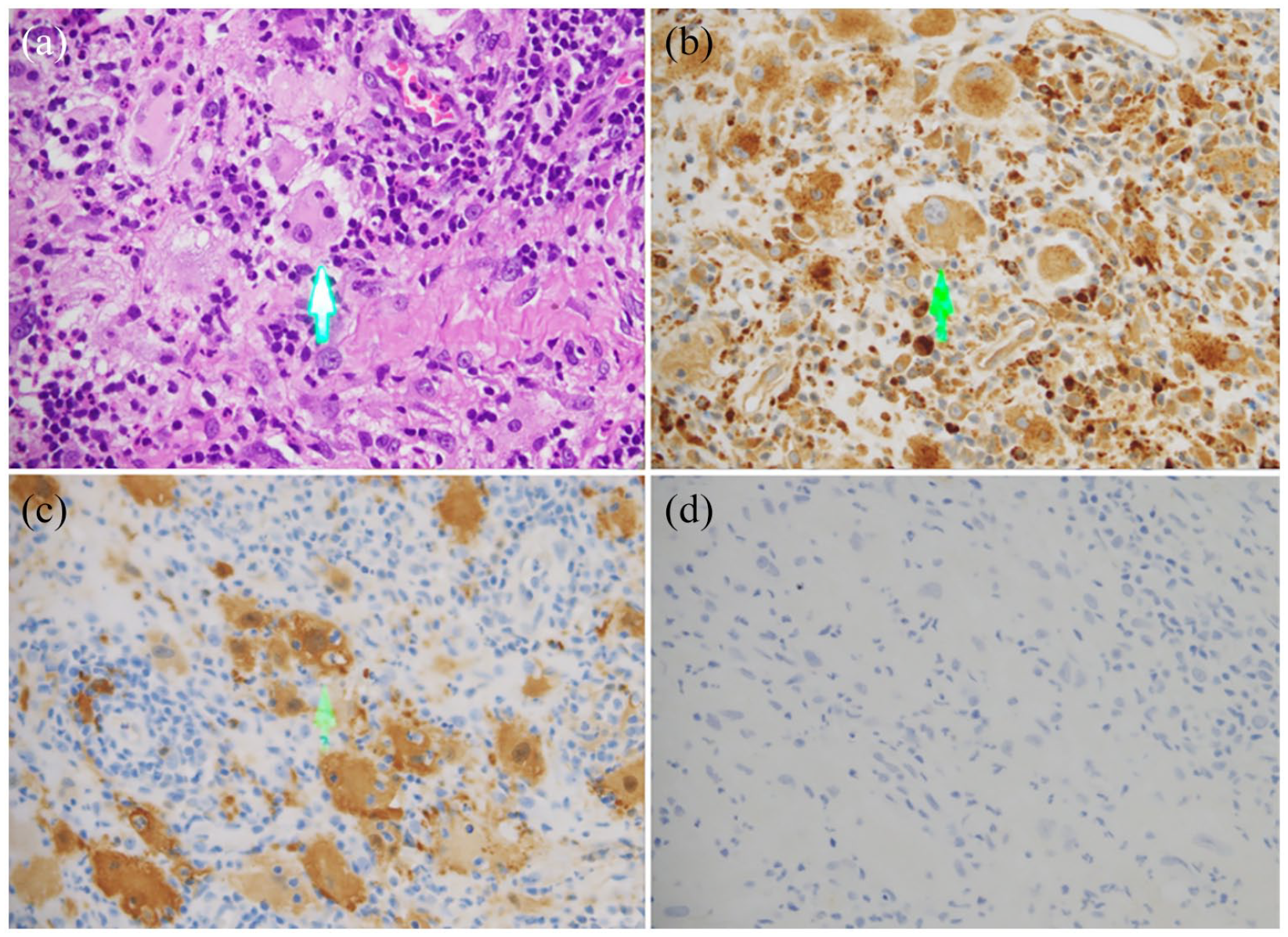
Histopathological findings. (a) Prominent histiocytic infiltration with emperipolesis (arrow). (b) Positive staining for CD68 histiocytic infiltrate showed emperipolesis (arrow). (c) Positive staining for S100 histiocytic infiltration showed emperipolesis (arrow). (d) Negative staining for CD1a.
We initially started the treatment with topical 1% prednisolone acetate four to six times daily for both eyes. Additional PST triamcinolone was given at a dosage of 20 mg. in each eye. Her condition started to improve after 2 weeks of medication initiation. Disc hyperemia and CME were reduced (Figure 3(c) and (d)). MTX had been given after receiving the skin biopsy pathological result. After 3 months of treatment, her condition had significantly improved, all skin lesions had disappeared, and no intraocular inflammation was detected in both eyes (no anterior chamber cell, normal contour fovea, and normal disc). MTX was discontinued after 4 months of treatment, and there was no uveitis recurrence after 6 months of follow-up.
Discussion
We reported a rare presentation of RDD with bilateral CAU with disc hyperemia and CME. The associated uveitis in the setting of RDD was reported previously in only eight cases during the past 10 years (Table 1). The most common presentation in those reported uveitis cases was bilateral anterior uveitis. They can be accompanied by other ocular presentations such as scleritis, intraocular nodules, and systemic involvement. Our case had a presentation of bilateral anterior uveitis with cutaneous involvement, with no other ocular manifestations, but complicated with CME and disc hyperemia.
Summary of 10-year reported cases of Rosai–Dorfman disease associated with uveitis.

AU: anterior uveitis; CME: cystoid macular edema; ED: eye drop; F: female; IMT: immunosuppressive therapy; LN(+): with lymphadenopathy; M: male; MTX: methotrexate; OS: left eye; OU: both eyes; PO: per oral.
Ocular involvement was reported to be associated with more aggressive behavior and an increased risk of systemic involvement. 4 However, a combination of isolated intraocular involvement without any ocular mass lesions and with cutaneous lesions was reported to have a benign character with no associated systemic lymphadenopathy. 12 While uveitis without a cutaneous lesion may be characterized differently by being associated with systemic lymphadenopathy.12,14,17
In comparison to a previous report from Japan, the RDD with uveitis and cutaneous lesions was reported to occur in young adulthood individuals (mean aged 38.5 years), and the most common form was bilateral granulomatous anterior uveitis, but patients aged less than 20 years may have unilateral diseases. 17 The cutaneous lesions can develop simultaneously or several months after the onset of uveitis.12,17 Our patient was older than previously reported; she is a middle-aged Asian female with bilateral granulomatous anterior uveitis. Interestingly, her cutaneous lesions developed during the late course of RDD without systemic lymphadenopathy after long-standing chronic anterior uveitis.
In the setting of CAU, careful systemic examination and dilated fundus evaluation are vital. The benefits of a patient’s historical review, extensive systemic examination, and complete eye examination have been shown in our case. The definitive diagnosis was confirmed by a skin biopsy, which altered the pattern of uveitis care in this case. Any abnormal skin lesions or ophthalmological mass lesions may help diagnose this disease. Further systemic investigations, such as imaging, are required to complete the systemic evaluation.
Currently, there is no definite treatment recommendation in the setting of RDD with uveitis. There were variously reported tailored approaches, including observation in asymptomatic cases or management with the different routes of corticosteroids (topical, intravitreal, and systemic administration), surgery, radiation, and chemotherapy in mass lesions or systemic involvement.4,6–8,12–15,17–21 RDD associated with uveitis tends to be completely cured after treatment (Table 1). Even though, in our case, the patient had moderate NPDR and CME might be a consequence of this disease, we believed this CME was uveitic macular edema rather than diabetic macular edema. 22 Because of the characteristic hyperemic optic disc fluorescein leakage, all microaneurysms on FA were found on the extrafoveal area, and OCT revealed a pronounced CME in the inner retinal layers, unlike more prominent in the outer retinal layers in diabetic macular edema. 22 In addition, a good response after anti-inflammatory treatment confirmed our diagnosis. To the best of our knowledge, this is the first report using a combination of topical steroids, a single dose of PST triamcinolone, and MTX to treat a patient with RDD and CAU complicated with CME and hyperemic disc.
Conclusion
Uveitis in the setting of RDD is rare. The combination of RDD with uveitis and cutaneous lesions is more benign and usually not associated with systemic abnormalities or lymphadenopathy. Regional treatment, together with a short course of MTX, can successfully treat a patient with RDD and uveitis with CME and disc hyperemia.
In this particular case, it is recommended that an ophthalmologist take seriously into consideration the essentials of history-taking and physical examination. Multidisciplinary collaboration is highly recommended.
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
This work involving human data was in accordance with the ethical standards of the institutional and national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. It was approved by the Institutional Review Board, Royal Thai Army Medical Department (No. IRBRTA S087h/64). For data availability, please contact the author for data requests.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.