
Abstract
Rosai-Dorfman disease (RDD) is a rare histiocytic condition of unknown etiology. Patients with RDD classically present with massive painless cervical lymphadenopathy. However, extra-nodal disease occurs in approximately 40% of cases, with the skin being among the most commonly involved sites. Patients with isolated extra-nodal involvement may present without adenopathy. Reports of RDD occurring in patients with Hodgkin’s lymphoma, and B-cell lymphoma have been published, but there has only been one previous report of RDD in a patient with a T-cell lymphoma. This case report documents a unique combination of RDD and mycosis fungoides (MF), a cutaneous T cell lymphoma. This report also highlights diagnostic challenges in RDD due to the rarity of the condition and its variable presentation.
Keywords
Introduction
Rosai-Dorfman disease (RDD), also called sinus histiocytosis with massive lymphadenopathy, is a nonmalignant histiocytic condition of unknown etiology that often resolves spontaneously without treatment.1–3 The classic presentation of this rare condition is massive painless cervical lymphadenopathy,1,3 however, extra-nodal disease occurs in approximately 40% of cases. 2 The most commonly involved sites in extra-nodal RDD include the skin and upper respiratory tract.1,2
Although the presentation of RDD may resemble lymphoma, the condition has characteristic histopathological features that clarify the diagnosis. In RDD, histiocytes show emperipolesis (i.e. intact erythrocytes and lymphocytes within the histiocyte cytoplasm due to non-destructive phagocytosis), which is characteristic of RDD and required for diagnosis.1,2 RDD histiocytes stain positively for CD68 and S100 and negatively for CD1a.1,3,4
There have been reports of RDD occurring in patients with Hodgkin’s lymphoma5,6 and B-cell lymphoma,2,7 but there has only been one report of RDD in a patient with a T-cell lymphoma. 8 This case documents a unique combination of RDD and mycosis fungoides (MF), a cutaneous T-cell lymphoma.
Case report
A 63-year-old male presented to the dermatology clinic for a routine full skin examination. He has been followed by dermatology for MF since his diagnosis in 1988. A timeline detailing the management of his MF is presented in Figure 1. He was diagnosed with 25 basal cell carcinomas and 2 squamous cell carcinomas within the past decade. His history is also significant for actinic keratoses, seborrheic keratoses, and porokeratoses. The patient is otherwise healthy and works as a personal trainer. He occasionally smokes cigars and marijuana. His family history is non-contributory.

Timeline of treatments for MF. The patient was diagnosed with MF in 1988 and RDD in 2017.
During the skin examination, 3 small, firm red nodules were noted on the patient’s back (Figure 2). The lesions were located on the left upper back, superiorly; left upper back, inferiorly; and the left mid back. Given the patient’s history, these lesions were suspected to be MF, however, shave biopsies were taken to rule out squamous cell carcinomas and large cell transformation.

RDD nodules.
Histopathology confirmed that the nodules were extra-nodal RDD and not MF lesions as initially suspected (Figure 3). All three biopsies showed characteristic features of RDD, including a dermal infiltrate of giant histiocytes exhibiting emperipolesis, and positive staining for CD68 and S100, with negative staining for CD1a. The specimens were reviewed at a dermatopathology consensus conference, and there was agreement between four pathologists on the diagnosis of extra-nodal RDD.

The cells stain positively for S100. Intact lymphocytes are visible within the cytoplasm of the giant cells (emperipolesis) at the center of the image.
RDD was not suspected in this case due to the patient’s atypical presentation and his history of MF. The patient did not exhibit massive cervical lymphadenopathy or any other systemic symptoms of RDD, such as fever. He was otherwise healthy, so a new disease process was not suspected, and the new lesions were assumed to be due to his ongoing MF.
The patient was seen approximately 3 weeks after the biopsies to discuss the results from pathology. He was examined, and two new red papules—similar to the lesions that showed RDD on biopsy—were noted on his abdomen. Cutaneous RDD follows a benign course, and it is common for lesions to spontaneously resolve. The lesions were small and not bothersome to the patient, so treatment was not initiated. He will continue to be followed by dermatology for his MF and RDD.
Discussion
This case serves to document a unique combination of RDD and MF, a cutaneous T-cell lymphoma. RDD has been associated with Hodgkin’s lymphoma5,6 and B-cell lymphoma,2,7 but this case is only the second report of RDD in a patient with a T-cell lymphoma. 8 A table summarizing key similarities and differences between this case and the previously reported one is provided in Table 1.
Summary of reported cases of RDD and T-cell lymphoma.
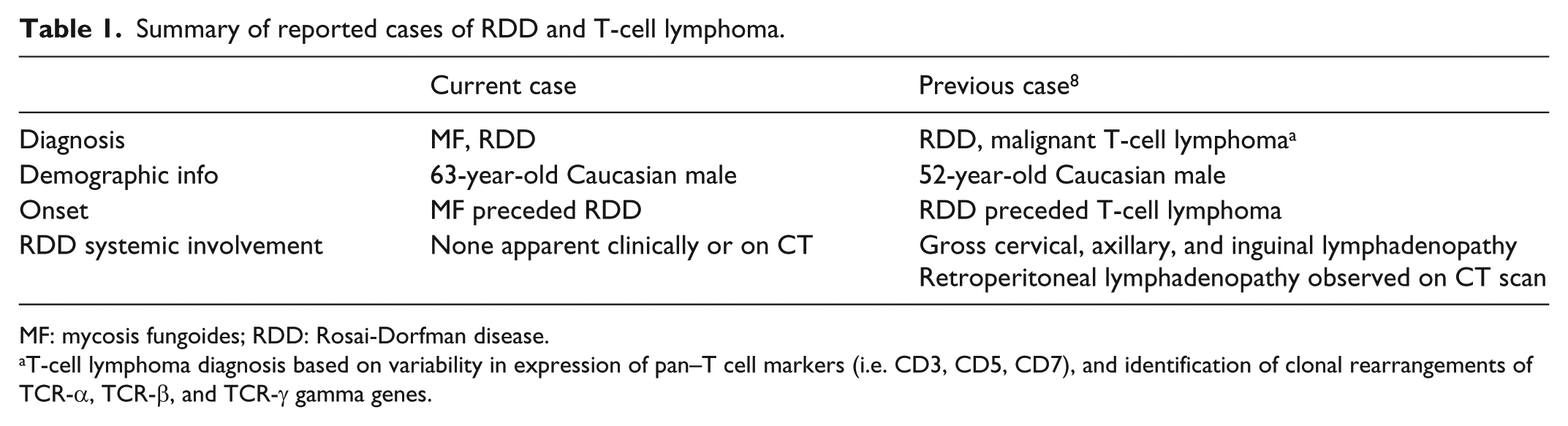
MF: mycosis fungoides; RDD: Rosai-Dorfman disease.
T-cell lymphoma diagnosis based on variability in expression of pan–T cell markers (i.e. CD3, CD5, CD7), and identification of clonal rearrangements of TCR-α, TCR-β, and TCR-γ gamma genes.
There are few cases of comorbid RDD and lymphomas reported in the literature, so it remains unclear if there is a true common pathogenesis between these conditions or if these reports represent chance associations. It is plausible that the abnormal immune response seen in both RDD and lymphomas provides a common pathogenesis for both conditions, and hypotheses in this regard have been proposed. For example, it has been suggested that elevated cytokine levels, including elevated tumor necrosis factor alpha, could be involved in a common pathogenesis between RDD and B-cell lymphomas.6,9
This case highlights diagnostic challenges in RDD, including the rarity of the condition and its variable presentation. Although the exact incidence and prevalence of RDD are unknown, only 423 cases were documented in an international registry between 1969—when the condition was formally recognized—and 1990. 2 Within the context of the extreme rarity of RDD, its variable presentation brings further challenges for diagnosis. For example, patients may present with the classic findings of RDD (i.e. massive cervical lymphadenopathy) or with isolated extra-nodal disease without lymphadenopathy. The patient reported in this case appears to have strictly cutaneous extra-nodal RDD, based on history and physical examination. CT scans of the patient’s neck, chest, abdomen, and pelvis were all negative for systemic involvement.
In conclusion, this report documents a unique case of comorbid RDD and MF. Previously, only one other co-occurrence between RDD and a T-cell lymphoma has been reported. This case also highlights diagnostic challenges in RDD brought about by the rarity of the condition and its variable presentation.
Footnotes
Acknowledgements
The authors would like to thank Dr Scott Bradshaw for providing pathology images and captions.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The patient verbally consented to the use of his clinical images for this report.