
Abstract
Most of the small-cell lung cancer patients are of the central type of lung cancer. Small-cell lung cancer often intrudes into the atmospheric tract and large blood vessels, thus causing severe tracheobronchial stenosis and superior vena cava syndrome. In addition, patients with malignant tumors, especially those with respiratory failure and severe hypoxia, can be complicated with thromboembolic diseases. We reported a 65-year-old woman with severe stenosis of the trachea, and right main bronchus complicated with acute respiratory failure was treated with bronchoscopy and stent implantation to improve the patient’s dyspnea, thus successfully receiving chemotherapy and timely treatment. After chemotherapy, the tumor shrank and the stenosis of the trachea and right main bronchus improved. We removed the right main bronchus stent and the tracheal stent successively to improve the quality of life of the patients. We managed both the cancer and exacerbation-related factors to improve the patient’s medical conditions so that the patient could receive timely and suitable treatment.
Keywords
Introduction
Small-cell lung cancer (SCLC) is a type of low-differentiated malignant epithelial tumor. Data from the International Association for the Study of Lung Cancer 1 show that the 2-year overall survival rate of the SCLC group of stages I, II, III, and IV is about 73%, 54%, 23%, and 8%, respectively. Data from Spain 2 indicate that 96.7% of SCLC patients could be present with metastases, with approximately 20% having brain metastases at the time of diagnosis. The overall survival was about 9.5 months, with the 1-year and 2-year survival rates being 38.9% and 14.8%, respectively. SCLC is highly malignant and invasive, prone to metastasis, and leading to a poor prognosis. SCLC is mostly a central type, and a few of the lesions can pressure the airway, resulting in severe tracheal stenosis and respiratory failure, the performance status score 3 can reach,4,5 thus affecting the treatment of tumors. Through endoscopic intervention and comprehensive management of critical conditions, patients with severe lung cancer can achieve reduced performance status scores and be effectively treated. We present herein the diagnosis and treatment of a severe SCLC patient with severe tracheal stenosis complicated with respiratory failure and myocardial infarction after tracheoscopic interventional therapy, and the patient was able to receive chemotherapy with improved myocardial blood supply.
Case report
A 65-year-old female patient was admitted to our department on April 3, 2022, due to hoarseness for over 1 month and aggravated dyspnea for 2 days. A chest computed tomography (CT) scan was performed in another hospital on March 30, 2022, showing a mass in the inferior lobe of the left lung, soft tissue mass in the mediastinum and right clavicular fossa, with unclear boundary with adjacent tissues, and there was the possibility of invasion to the lymph nodes and adjacent tissues and with pericardium and bilateral pleural effusion. MRI scan of the entire spine showed small patch-like abnormal signals at the rear of thoracic 7 vertebrae, excluding the possibility of metastatic tumor, abnormal signals at thoracic 11 and lumbar 2 vertebrae suggested benign lesions and angio-lipoma. Plain MRI with contrast showed abnormal enhancement in the left frontal area, indicating the possibility of meningioma. On April 1, 2022, a lymph node biopsy in the right supraclavicular area showed malignant tumor. The patient, who was transferred to our hospital due to worsened dyspnea on April 3, 2022, had a physical examination on admission. The respiratory rate increased to 30 breaths per minute and the patient was unable to lie supine; the blood gas values showed type I respiratory failure. A chest CT (Figure 1(a) and (b)) was done in the emergency room (ER) which revealed severe stenosis of the trachea and right main bronchus in an emergency, and bare metal stent implantation was performed under a rigid bronchoscope in an ER. The examination results showed tracheal stenosis and a rigid bronchoscope was inserted through the mouth after total intravenous anesthesia. The epiglottis was normal, and the endotracheal external pressure began to narrow at about 3 cm under the glottis in the upper tracheal segment, and the diameter of the lumen at the narrowest point was about 2–3 mm. After the rigid bronchoscope was passed, the carina widened, and the left and right main bronchial openings showed different degrees of stenosis, part of the left main bronchial mucosa was hypertrophic, and the left main bronchial artery was compound stenosis, guide wire was inserted, and the metallic stent was removed. A metal stent of 1.6 cm × 8 cm was placed in the trachea through the stent pusher, which was located on the carina, and the stent release was satisfactory. A metal stent of 1.4 cm × 3 cm was successfully placed in the right main bronchus, and the rigid bronchoscope was removed.
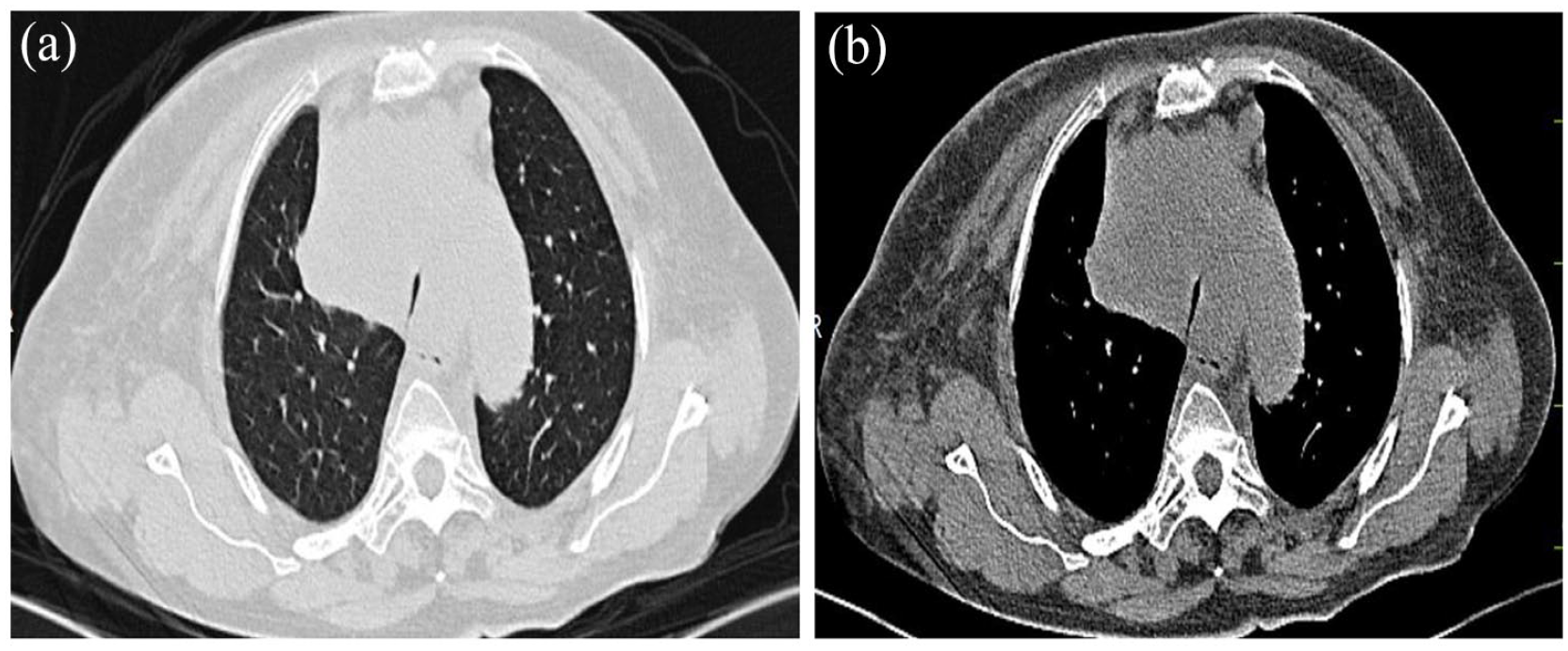
(a) Chest computed tomography (CT) on April 3, 2022 showed severe tracheal stenosis. (b) Severe stenosis of the right main bronchus on chest CT on April 3, 2022.
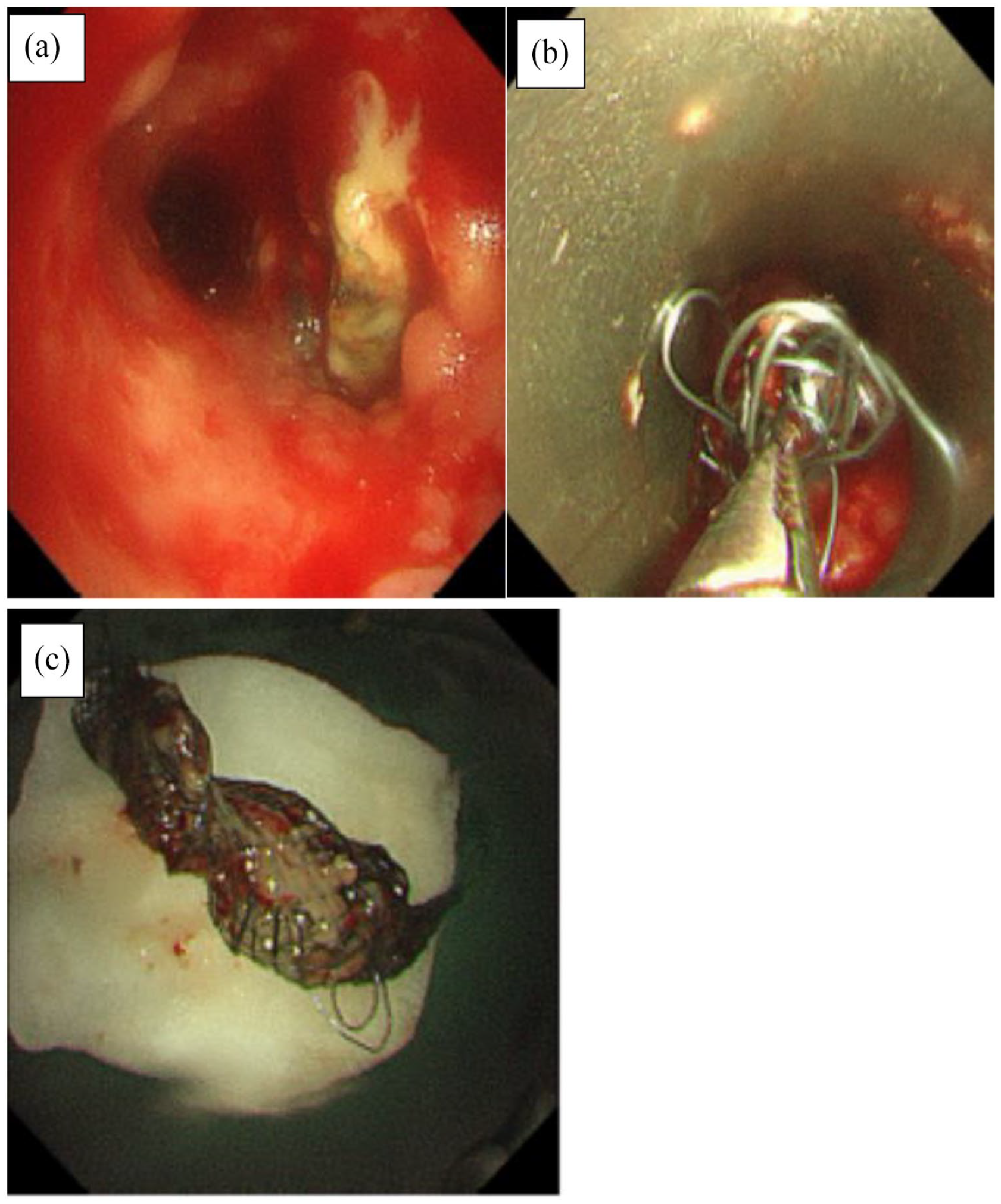
After the operation, the patient was transferred to the Respiratory Intensive Care Unit where she received comprehensive treatment involving tracheal intubation, mechanical ventilation, fluid rehydration, and maintenance of water, electrolyte, and acid–base balance. After April 4, 2022, the patient suffered an acute myocardial infarction and acute left heart failure, the symptoms were improved after anti-platelet aggregation, anticoagulation, lipid-regulating, heart strengthening, diuresis, crown expansion, tracheal catheter was pulled out, and non-invasive ventilator-assisted ventilation was given. All indexes, such as myocardial enzyme profile, heart failure index, and troponin, returned to the normal range and the performance status score dropped to 2 points, and the patient was given etoposide 100 mg D1-3 combined with carboplatin 350 mg D1 on April 15, 2022, and symptomatic supportive treatments such as antiemetic drugs, and drugs for stomach protection were also administered. The chest CT mass was significantly reduced in the review performed on April 29, 2022 (Figure 2). The patient was discharged after no complaints of discomfort, and chemotherapy with etoposide 100 mg D1–D4 combined with carboplatin 400 mg D1 on May 22, 2022, was administered. The patient’s performance status score was reduced to 1 point. The patient underwent bronchoscope metal stent removal of the right main bronchus and trachea on June 13, 2022 (Figure 3) and June 20, 2022, respectively (Figure 4). Later, etoposide 100 mg D1–D4 combined with carboplatin 400 mg D1 was used for chemotherapy on June 24, 2022, July 28, 2022, August 28, 2022, and September 26, 2022 and the condition was evaluated to be stable at present.
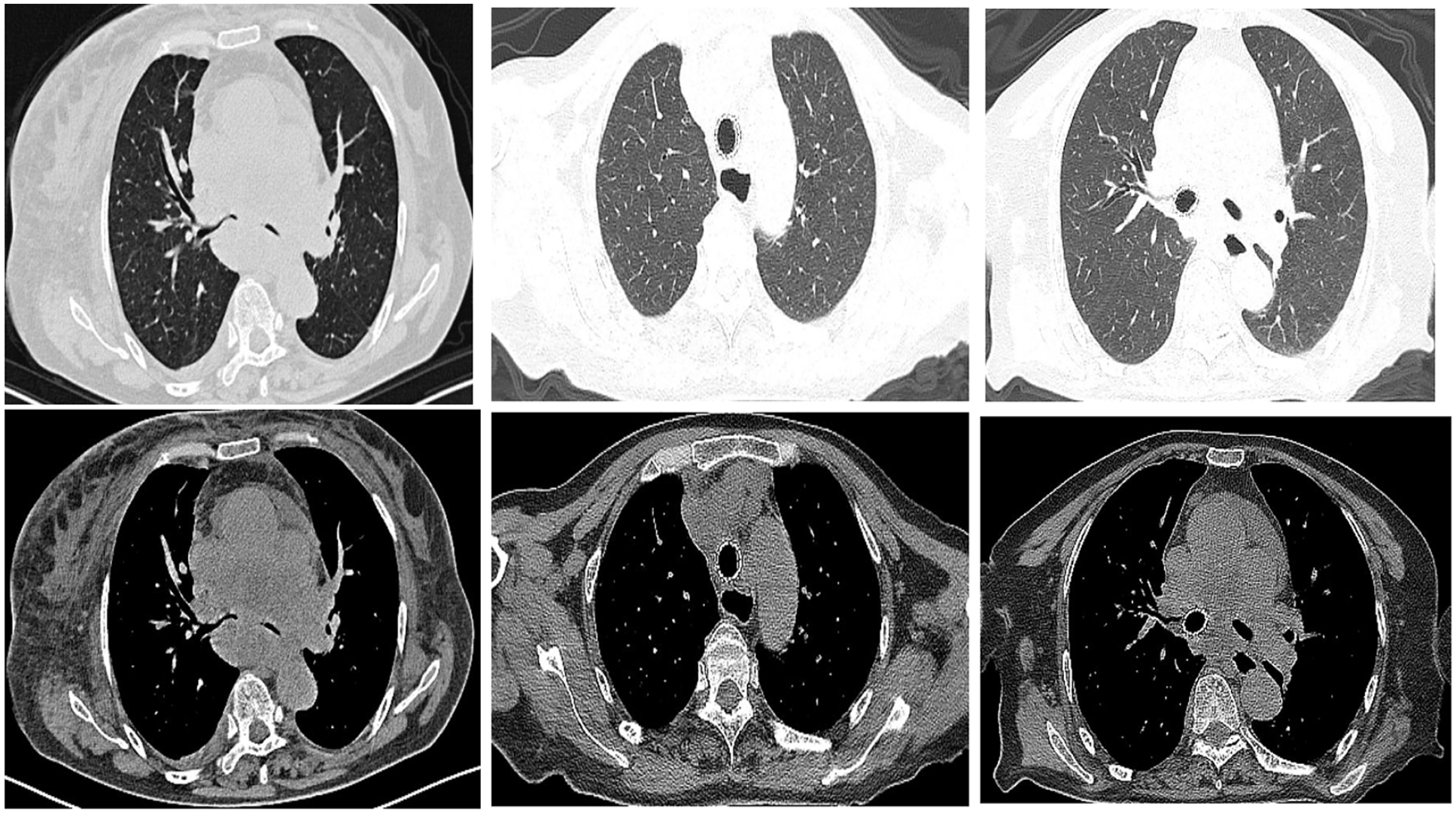
Chest CT after stent implantation and chemotherapy on April 29, 2022.

Metal stent removal of the right main bronchus under bronchoscope on June 13, 2022. (a) Tracheal stent. (b) Right main bronchial stent. (c) After the stent was removed from the right main bronchus. (d) The right main bronchial stent was removed.
Removal of metal tracheal stent under bronchoscope on June 20, 2022. (a) Endotracheal stent granulation. (b) Tracheal stent removal. (c) The removed tracheal stent.
Discussion
As SCLC is sensitive to chemotherapy, it is suggested in the guidelines that patients with a physical status score of 3 due to SCLC itself may be given salvage chemotherapy. The concept of severe lung cancer has been reported in the literature, 6 but not mentioned in the major lung cancer guidelines. Severe lung cancer refers to patients with lung cancer itself in a more advanced stage, or with a higher co-incidence of cardiovascular disease, chronic obstructive pulmonary disease, or respiratory infections. In the case of severe lung cancer, the lung cancer and the contributing factors should be treated together. Depending on the state of the patient, the performance status score may be reversible and fluctuate.
Surgical resection and reconstruction are the gold standard for the treatment of tracheal stenosis. However, for patients ineligible for surgery due to poor general condition, airway stenting is the option for treatment.7–11 In this case, the patient had obvious dyspnea due to severe tracheal stenosis, PS score 3–4, respiratory failure, indicating severe lung cancer, and the dyspnea was improved after endotracheal stent placement. Due to severe hypoxia, the patient developed cardiovascular disease like myocardial infarction after stent implantation. Currently available stents mainly include silicone stents and metal stents. Surgery remains associated with a high intraoperative mortality rate and postoperative complications, making it a less favorable option. Airway stenting can rapidly reconstruct the airway and alleviate symptoms such as respiratory distress,12,13 making it a potentially effective method. In our hospital, metal stents are easier to obtain than silicone stents, and silicone stents need to be customized, which delays time, and the patient’s condition was critical, and the stent needed to be placed immediately to correct respiratory failure, so metal stents were chosen. After treatment, the oxygenation index of the patient was improved, and the myocardial enzyme spectrum gradually returned to normal. After treatment with airway stenting, anticoagulation, anti-platelet aggregation, strong heart, and diuresis, the performance status score decreased, and EP (Etoposide combined with cisplatin) regimen chemotherapy was selected. Chest CT review after chemotherapy showed that the lesions were significantly reduced and the performance status score was reduced to 0–1 points with tracheal stenosis significantly improved. If a metal stent is placed for a long time, it is easy to cause displacement and fracture of the support. Moreover, the tumor shrank after the patient underwent chemotherapy, and the compression effect on the airway was relieved, so we chose to remove the stent as soon as possible. At last, the metallic stent was removed after several courses of chemotherapy.
Conclusion
Patients with primary airway obstruction who are sensitive to initial local therapy may have significantly lower performance status scores even after appropriate interventional therapy; this may suggest the need for further anticancer therapy. In the case of severe lung cancer, the lung cancer and the contributing factors should be treated simultaneously. The patient was evaluated to be stable at present. This case shows that the performance status score of patients may be reversible and fluctuate, so patients should be treated actively and timely.
Footnotes
Author contributions
H. L. contributed to conception and design; H.L. contributed to the provision of study materials or patients; H.L. contributed to the collection and assembly of data: J.Z. contributed to the data analysis and interpretation; All authors wrote the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Informed consent
Written informed consent for the publication of all clinical details and images was obtained from the patient.