
Abstract
The pathophysiology of the virus causing coronavirus disease 2019, the cytokine storm and severe vasculitis is well known. Diabetic patients and those with microcirculation issues are at risk of complications when diagnosed with coronavirus disease 2019. Calcium dobesilate has been used extensively for microangiopathy, diabetic retinopathy, chronic venous insufficiency, hemorrhoidal and post-thrombotic syndromes. We administered calcium dobesilate to several patients in our coronavirus disease hospital; documenting disease progression outcomes relating to cessation of disease worsening, reduction in glucocorticoid dose and oxygen. We present two case reports: patient 1 with acute and patient 2 with sub-acute coronavirus disease 2019; both patients received standard of care plus calcium dobesilate. Patient 1 achieved clinical, radiographic and laboratory improvements. Patient 2 derived calcium dobesilate benefits during the acute phase of coronavirus disease 2019 negating the need for supplemental oxygen and dose increases of dexamethasone. Further research is required to support the use of calcium dobesilate in coronavirus disease 2019 patients.
Introduction
Before the COVID-19 pandemic, the risk of developing complications following viral infection in patients with comorbidities associated with endothelial dysfunction was not well understood, and the onset of several non-pulmonary complications such as acute myocardial injury, renal failure or thromboembolic events was poorly described. The pandemic has highlighted the impact of COVID-19 on endothelial cells and the development of endotheliitis, thrombosis, and angiogenesis. Within the Mexican population there is a high prevalence of obesity, high blood pressure, insulin resistance and/or dyslipidaemia, predisposing individuals to contracting and developing progressive forms of COVID-19.
The treatment goal is to stabilize the endothelium thereby avoiding and/or decreasing any substrate that enhanced the virus’ progressive course (Figure 1),1–3 and includes weight control, nutrition, and physical exercise. For many patients this is insufficient and pharmacological treatment is required.
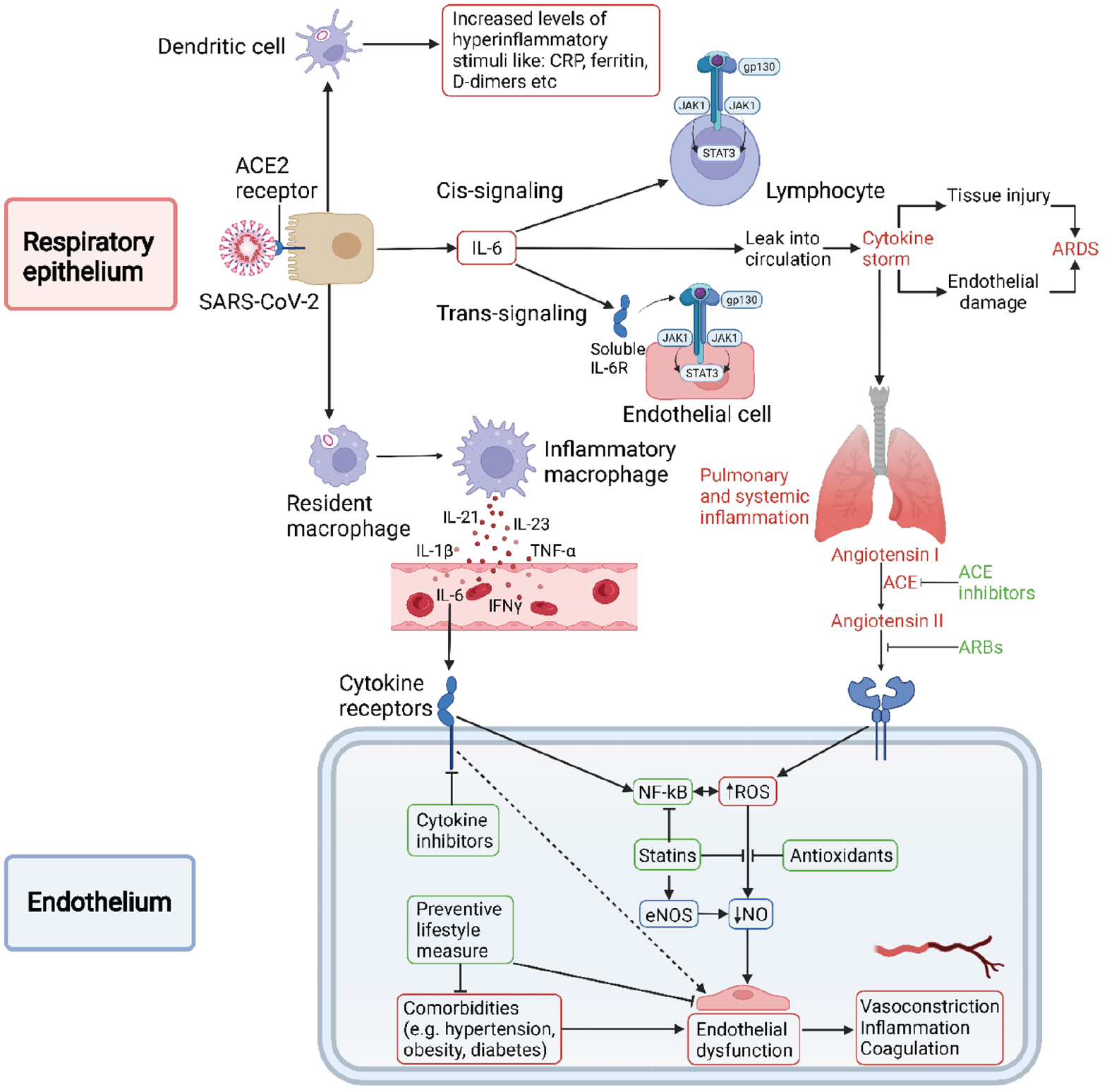
Calcium dobesilate (CaD), a well-established venoactive drug used in the treatment of several pathologies such as chronic venous insufficiency, hemorrhoidal diseases, and diabetic microangiopathies, has interesting properties in regard to COVID-19.4,5 Of particular interest are the anti-oxidative, anti-inflammatory and growth factor modulatory actions leading to an endothelium protective effect. Recently, CaD has been shown to reduce Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) entry into endothelial cells, possibly preventing further viral spreading into the microvasculature. 6
Preventive action
Entry of SARS-CoV-2 into the cell depends on three critical steps:
Its fixation to the cell surface via heparan sulfate.
Binding to the angiotensin converting enzyme 2 receptor through the S1 subunit and the spike protein binding domain.
Activation of the S2 subunit of the spike protein by the transmembrane serine 2 protease associated with the host cell surface.
That CaD potentially intervenes with these steps,5,7 and requires further evaluation.
Stabilizing action
While SARS-CoV-2 produces a state of intense inflammation, CaD acts in an antioxidant, anti-inflammatory, and antithrombotic way toward the endothelium,8–11 preventing sequelae. Oxidative stress and reactive oxygen species have been implicated in the pathophysiology of COVID-19. 12 Studies on human varicose vein cells have shown protective effects of CaD on oxidative stress by decreasing free radicals and strengthening the antioxidant system.10,13,14
CaD inhibits fibroblast and vascular endothelial growth factors15,16 favoring angiogenesis and the development of fibrosis, triggered by SARS-CoV-2.8,16,17
Post-COVID syndrome
Several publications have commented on the persistent symptoms of COVID-19.18,19 Greenhalgh et al. define post-acute COVID-19 as disease extending beyond 3 weeks from onset and provide guidance for disease management through monitoring and specialist rehabilitation. 20 Aguirre et al. consider the acute stage as being up to 4 weeks, 21 but only up to 3 weeks for mild and asymptomatic cases. 21 Three definitions of disease duration have been described (shown in Figure 2):
ACUTE COVID-19: Illness lasting up to 3 weeks from the date of onset of symptoms for the mild and asymptomatic, and up to 4 weeks for moderate, severe and critical cases.
COVID-19 POST-ACUTE OR SUB-ACUTE: Illness where symptoms persist beyond 3 weeks from the date of onset of symptoms in mild and asymptomatic, and more than 4 weeks for moderate, severe and critical cases.
CHRONIC COVID-19: Illness extends beyond 12 weeks from the date of onset of symptoms.
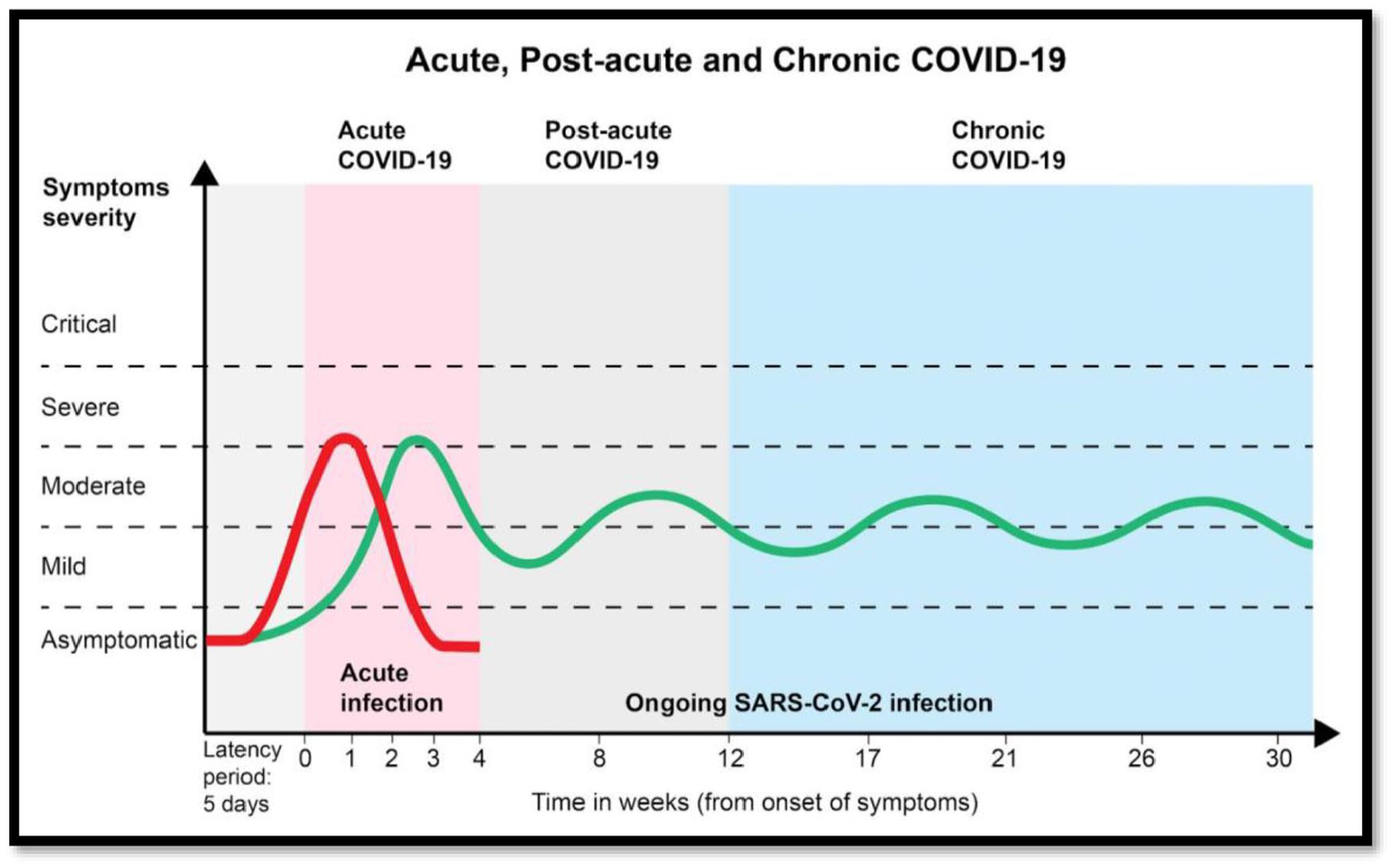
COVID-19 acute, post-acute and chronic disease duration.
Established facts
The pathophysiology of COVID-19 includes a cytokine storm accompanied by inflammation and intense vasculitis.
The goal of treatment is to stabilize the endothelium to avoid and/or decrease the progressive course of COVID-19.
Novel insights
The mechanisms of action of CaD can be beneficial during different stages of COVID-19.
Clinical, radiographic, and laboratory improvements were noted when CaD was added to COVID-19 treatment regimens.
Clinical experience and rationale for the use of calcium dobesilate to treat COVID-19 patients
We administered CaD to several patients at our hospital and documented disease progression outcomes relating to cessation of disease worsening, reduction in glucocorticoid dose and oxygen. Two case reports have been selected: patient 1 with acute and patient 2 with sub-acute COVID-19, both received 8 weeks of CaD treatment. Patients gave their written informed consent to publish their cases.
Case 1
A 72-year-old female (blood group O RH-) with dyslipidaemia (2 years), and uncontrolled osteoporosis was diagnosed with COVID-19 on December 31, 2020 through a positive polymerase chain reaction (PCR) test. 22 She presented for consultation on February 4, 2021, with a constant productive cough with nocturnal exacerbations and progressive asthenia. Laboratory test results revealed an increased erythrocyte sedimentation rate, C-reactive protein, ferritin, lactic dehydrogenase, low-density lipoprotein cholesterol and triglycerides at baseline. Posteroanterior and lateral chest X-rays showed bilateral faint alveolar opacities in the lower and middle lungs with increased bilateral density.
Treatment with CaD (500 mg every 8 h), colchicine (1 mg every 24 h) and an inhaled steroid with 160/4.5 mcg of budesonide/formoterol (every 8 h) was initiated. The patient was diagnosed with sub-acute post-COVID syndrome.
Biomarkers were repeated after 1 week showing normalization of the erythrocyte sedimentation rate, C-reactive protein, and lactic dehydrogenase, with a slight increase in ferritin. Chest X-rays showed clear clinical improvement of the interstitial-reticular pattern and bilateral basal alveolar opacities. Treatment continued and a follow-up appointment was scheduled for 2 weeks later.
Clear clinical improvement was observed 3 weeks post treatment with a slight decrease in ferritin. Chest X-rays showed a substantial decrease in the interstitial-reticular pattern and bilateral basal alveolar opacities. Treatment continued for another 4 weeks (total of 8 weeks) with a dosing frequency reported above apart from CaD (500 mg every 12 h). The patient reported complete remission of symptoms.
Case 2
A fit 50-year-old male (blood group A) presented with rhinorrhoea, headache, chest tightness, odynophagia and fever for 2 days. He tested positive for COVID-19 by PCR test. 22
The patient presented to the clinic on day 3with an intense constant cough and an average oxygen saturation of 87%. Treatment with CaD (500 mg every 8 h), colchicine (1 mg every 12 h), inhaled steroid with 160/4.5 mcg of budesonide/formoterol (every 12 h), anticoagulant (every 24 h) and dexamethasone (4.5 mg every 24 h) was initiated. An initial posteroanterior chest X-ray was requested which showed evidence of a notable interstitial-reticular pattern with bilateral basal predominance.
Laboratory tests were obtained on different dates to ensure a comprehensive follow-up of the patient (Table 1).
Laboratory test results showing changed parameters.

Day 15 of the disease demonstrated a correlation between worsening of cough and chest tightness without a decrease in oximetry, and laboratory results with a substantial elevation of acute phase and liver function parameters. Despite this, no supplemental oxygen or higher dose of dexamethasone was required.
CaD 500 mg was prescribed every 12 h for 8 weeks, followed by a chest X-ray which demonstrated substantial improvement in the interstitial-reticular pattern, with no remaining symptoms.
Both patients remain asymptomatic.
Discussion
Endothelial dysfunction is a significant feature of COVID-19 and is associated with severe cases of the disease. 2 Given the current knowledge, it is known that risk factors such as obesity, high blood pressure, insulin resistance, dyslipidemia, diabetes mellitus, and blood group A and AB predispose patients to COVID-19 disease progression.23,24 Hence, there is an urgent need for suitable treatments particularly where these risk factors are highly prevalent such as in the Mexican population. CaD is a cost effective, established treatment with proven pleiotropic effects, with an easy dosage regimen and minimal adverse effects. 6
In the first case, satisfactory clinical, radiographic and laboratory improvements were achieved when CaD was administered. This favorable outcome was accomplished without systemic steroids which may have more severe side effects in older patients, especially when administered for long periods and at high doses, not discounting the economic cost. We see an opportunity to administer CaD in patients with post-COVID-19 syndrome as well as during the acute phase of the disease.
In the second case, we reported the benefits of CaD in the acute phase of the disease in a younger patient without comorbidities. Based on our current knowledge of the disease, we assumed that there would be no major radiographic or laboratory alterations; however, this was not the case. Fortunately, it was not necessary to administer supplemental oxygen or increase the dose of dexamethasone in this patient.
One potential limitation to the case reports lies in the fact that as the patients remained asymptomatic, the medical team did not deem it necessary to continue to monitor them and so no follow-up tests were performed.
Conclusion
In addition to the aforementioned, treatment and follow-up should be offered to patients with post-COVID syndrome as it can impact on the patient’s quality of life of. The efficacy and safety of CaD in patients with COVID-19 should be further evaluated in well-controlled clinical trials. The results could then be extrapolated to other populations with characteristics similar to the Mexican population.
Footnotes
Acknowledgements
Editorial assistance in the preparation of this article was provided by Woolford Medical Media Ltd.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this assistance was funded by OM Pharma.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article. – YES