
Abstract
Eosinophilic fasciitis can be a debilitating diagnosis and is often delayed given its similarities to other sclerotic conditions including morphea, such as bound-down indurated skin and inflammation and sclerotic thickening of tissue layers on histopathology. Delaying treatment can lead to joint contracture and residual hardness in skin which has both cosmetic and functional implications. Therefore, finding the definitive diagnosis and differentiating from other sclerotic diseases is important early in the disease course. We present a case of a 77-year-old female with a generalized rash on her back and extremities, and progressive symptoms of pain, joint contractures, and limited movement, which highlights the challenges in diagnosis and management given clinical and histological parallels between eosinophilic fasciitis and morphea.
Introduction
Eosinophilic fasciitis (EF), also referred to as Shulman disease, is a rare connective tissue disorder that often presents with symmetric and progressive induration of the subcutaneous tissue in the distal extremities leading to “peau d’orange” dimpling of the skin and “groove sign” and can be accompanied by myalgias, arthralgias, lower extremity edema, and morphea. 1 It may be preceded by strenuous physical exercise or trauma. 2 Investigations often show hypergammaglobulinemia, peripheral eosinophilia, elevated erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP), and diffuse fasciitis on histology.1,3,4
It was first described in 1974 by Shulman in cases presenting with scleroderma-like hardening of skin on limbs and since then over 300 cases have been described in the literature. 3 It primarily affects adults in the fourth or fifth decade of life; however, the exact incidence is unknown.
The criteria for diagnosing EF (Table 1) and classifying severity (Table 2) was published in 2016 as part of a policy research project on scleroderma and fibrotic skin diseases.3,5 The current standard of management is oral corticosteroids which is effective in more than 90% of cases, followed by methotrexate, cyclosporin, or cyclophosphamide if unresponsive to steroids. 3 Ultraviolet therapies, including psoralen and ultraviolet A therapy, can also be effective. 3
Diagnostic criteria of eosinophilic fasciitis. 3

A definitive diagnosis is made when a patient has the major criterion and one of the minor criterion, or the major criterion and two of the minor criterion.
Severity classification of eosinophilic fasciitis. 3

A total of two or more points is classified as severe.
EF is a difficult diagnosis to make given its similarity to morphea. This case shows the challenges in diagnosis and management given clinical and histological parallels to morphea.
Case report
A 77-year-old female was referred for dermatitis with a 2-year history of a generalized rash involving her back and upper and lower extremities. She presented with progressive symptoms of pain, joint contractures, and limited movement. She had been previously seen by two dermatologists and had been treated with clobetasol cream, prednisone, hydroxyzine, and hydrocortisone cream with no improvement.
On examination, affected areas included involvement of lower extremities including feet, arms, and back. There was symmetrical and circumferential swelling and erythema of bilateral feet and ankles with “groove” sign on the dorsum of both feet (Figure 1). There was induration of the skin on mid- and lower-back with peau d’orange appearance and groove sign at the midline low back (Figure 2).

Bilateral lower extremities with symmetrical and circumferential swelling and erythema. Groove sign present on the dorsum of either foot.
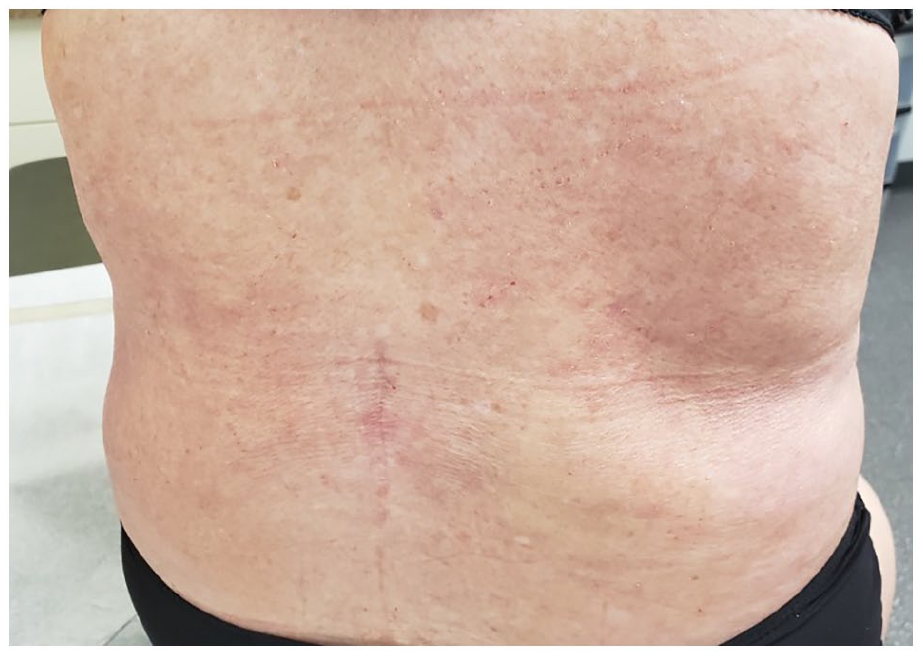
Induration of the skin on mid- and lower-back with peau d’orange appearance. Groove sign present at the midline of lower back.
This patient had a past medical history of hypertension, microscopic colitis, and a remote history of possible psoriasis in her teenage years. Her only medications included Telmisartan and Cholestyramine resin. She had a latex allergy, but no known drug allergies. There was no significant family history. She was a retired housekeeper.
In April 2021, she had a biopsy of the right middle and lower back which showed a thickened reticular dermis that surrounds adnexal structures with thickened collagen bundles as well as other minor changes including irregularity in the lower levels of epidermis associated with prominent stromal cells, few chronic inflammatory cells around superficial blood vessels, acanthotic epidermis with parakeratosis—all in keeping with morphea. A repeat biopsy was done May 2021 of her right and left abdomen and pathology showed thinned epidermis with minimal hyperkeratosis, sparse perivascular lymphocytic infiltrate, and dermal sclerosis with increased spaces between collagen bundles and loss of adnexal structures all consistent with morphea again.
In July 2021, she was referred by rheumatology to general surgery for a biopsy of the left calf with full-thickness fascia, which showed features consistent with EF. Her laboratory investigations showed eosinophilia, positive antinuclear antibody (ANA) titer of 1:80, and positive smooth muscle antibody titer of 1:80. She had a normal peripheral blood smear, ESR and CRP values within normal range, and negative anti-SCL 70, anti-centromere, and anti-mitochondrial antibodies. Her serum protein electrophoresis (SPEP) showed trace restriction/band in gamma region with no apparent background gamma suppression, the significance of which was uncertain, possibly due to recent infection or inflammation and was suggested to repeat in 3–6 months or urine electrophoresis for monoclonal light chains.
These findings placed together led to the diagnosis of EF, and the patient was started on 40 mg prednisone with a taper and methotrexate with significant improvement in the appearance of the lesions and ability to ambulate with ease only a few weeks after initiation of therapy.
Discussion
The diagnosis of EF is often difficult, and treatment can be delayed, as was the case for the patient discussed. EF has a 50% overlap with morphea both clinically and histologically, which is what makes it a particularly difficult diagnosis. Clinically, both conditions present with bound-down indurated skin and histopathologically, both show inflammation and sclerotic thickening of tissue layers. 6
In addition, the gold standard for diagnosis of EF is a full-thickness skin biopsy containing fascia and muscle tissue, whereas morphea tends to be more of a clinical diagnosis, which may require a skin biopsy only if the clinical presentation is unclear. 4 Our case highlights how two previous biopsies were consistent with morphea likely because the biopsy was not deep enough; however, the full-thickness biopsy was consistent with EF. Biopsies for EF usually show infiltration of the fascia with lymphocytes, eosinophils, plasma cells, and macrophages; however, the eosinophils may be transient if previously treated with systemic corticosteroids or immunosuppressive drugs.
Oral corticosteroid therapy is the mainstay of treatment of EF and is effective in over 90% of cases with good prognosis. Delaying treatment, however, can lead to joint contracture and residual hardness in skin, which has both cosmetic and functional implications. 3 Therefore, finding the definitive diagnosis and differentiating from other sclerotic diseases is important early in the disease course.
In conclusion, EF can be a debilitating diagnosis and is often delayed given its similarities to other sclerotic conditions; however, timely diagnosis and treatment is necessary to prevent permanent cutaneous and muscular damage and improve function and ambulation in patients.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient consent
Patient consent was obtained for publication of the case report content.