
Abstract
Airway management in neonates is difficult because of the risk of rapid hypoxia. It presents a challenge even for an experienced anesthesiologist. Oral tumors in neonates can obstruct the airway or feeding problems in the newborn. Surgical excision is the treatment of choice but these tumors can seriously worsen the conditions of intubation. To surmount these difficulties, a particular multidisciplinary approach and special precautions are needed. We describe the airway management and precautions taken in the anesthesia for surgical removal of a case of large congenital palate teratoma associated with a wide cleft palate in a 25-day-old girl. Impossible intubation was predicted on magnetic resonance imaging. The difficult airway management cart as well as an otorhinolaryngologist skilled in performing emergency tracheostomies in neonates were available. The patient was intubated by conventional laryngoscopy under sevoflurane inhalation anesthesia. The tumor was successfully resected. This case poses a challenge for managing the airway because of the possibility of obstruction of the airway and the difficulty of the airway that radiological exams have allowed us. So, a multidisciplinary team effort is needed for successful neonatal airway management.
Introduction
Airway management in neonates is often difficult because of the anatomical specificities of the larynx and because of the risk of rapid hypoxia due to a lower functional residual capacity reserve. 1 It presents a challenge even for an experienced anesthesiologist. Several congenital oral tumors may interfere with the development of the palate. These tumors that develop before the sixth week of gestation between the two palatal shelves prevent their elevation and their fusion with the nasal septum. These tumors associated with cleft palate can be obstructive and may increase the degree of difficulty of intubation cause. 2 The surgical removal of these tumors may also lead to mucosal edema that can cause a significant decrease in airway caliber postoperatively. To surmount these difficulties, a special multidisciplinary approach and particular precautions are needed. 3 In this case report, we describe the airway management and precautions taken for the anesthesia of a newborn scheduled for surgical removal of a congenital palate teratoma with a cleft palate.
Case report
We report the case of a 25-day-old female newborn who presents with a congenital tumor of the palate associated with a cleft lip and palate (Figure 1). An antenatal ultrasound at 23 weeks of amenorrhea detected a cleft lip. So, the mother was referred to our department, and delivery was programmed at term by cesarean section. At birth, the newborn had a good adaptation to extrauterine life and weighed 3000 g. The examination showed the presence of a buccal mass measuring 4 cm × 2 cm in diameter with soft consistency relating to a wide base with the palate associated with a wide right cleft lip and palate. The mass prevented normal closure of the mouth and interfered with breastfeeding, but she did not pose an immediate airway concern. No other comorbidities were detected during the physical examination. Brain and abdominal ultrasound were normal. Preoperatively, the newborn did not present a problem of respiratory distress, and feeding was possible by force-feeding. The infant was scheduled for excision of the palate mass through an oral approach under general anesthesia. The cleft palate will be surgically repaired when 6 months old. The magnetic resonance imaging (MRI) showed a well-defined lesion attached to the nasal septum between the two palate shelves with intrabuccal extension. The lesion was heterogeneous and contained areas of hyperintense signaling. It also noted the retention of fluid within ethmoid cells upstream from the tumor evoking a mature teratoma (Figure 2). The data from the MRI predicted impossible intubation, which posed a problem for general anesthesia. Parents were made aware of airway management alternatives such as difficult intubation and the possibility of a tracheostomy during the operation.

Clinical appearance of palate teratoma associated with a cleft palate: tumor covered with fine downy skin protruding from the shelves of the cleft.
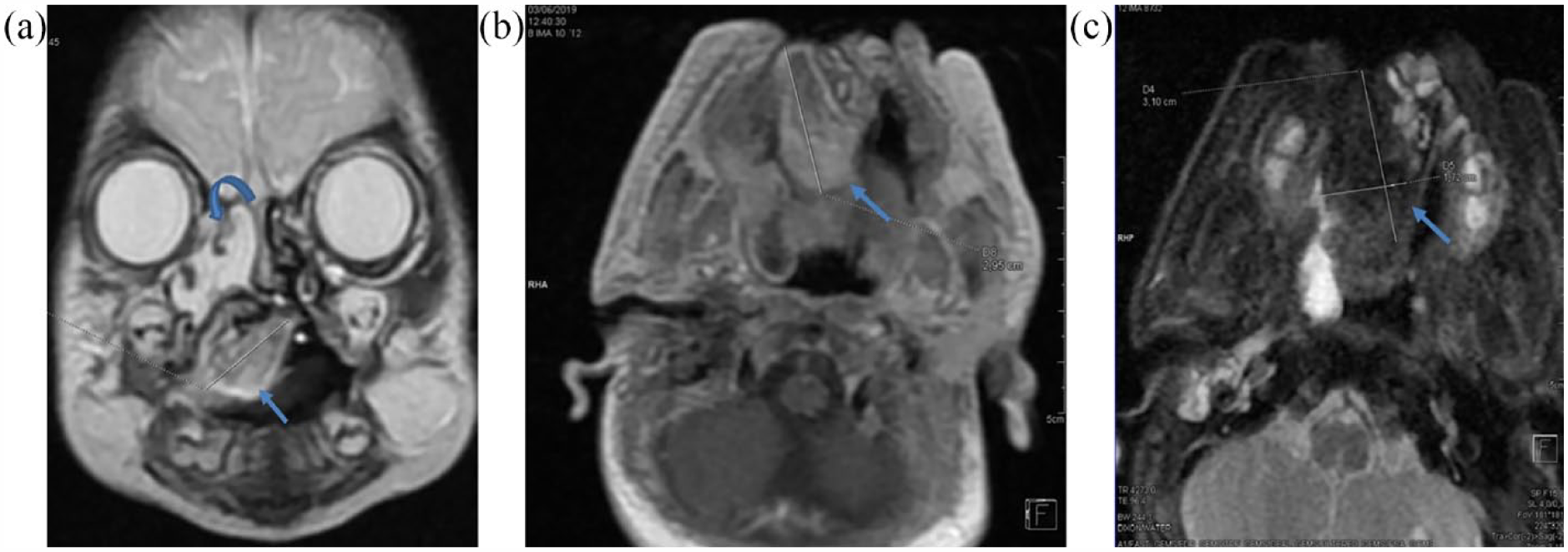
(a) MRI T2-weighted coronal image shows a lesion attached to the nasal septum between the two palate shelves with intrabuccal extension. The lesion is heterogeneous and contains areas of hyperintense signaling (arrow). we note also retention of fluid within ethmoid cells upstream from the tumor (curved arrow). (b) An axial T1-weighted image shows a hyperintense heterogeneous encapsulated lesion measuring 3 cm approximately. (c) T2-weighted fat suppressed axial image shows loss of signal intensity on the tumoral lesion which suggests the presence of macroscopic fat (arrow).
Before anesthesia induction, the difficult airway management cart was tested and it was available in the operation room. Suction was also functional on the head of the patient. A supraglottic airway device (I-Gel) was available as a rescue airway. Finally, an otorhinolaryngologist, skilled in performing emergency tracheostomy in a neonate was ready. Intravenous access was obtained before the intervention. Then sevoflurane induction was done, and a laryngoscopic look showed the epiglottis and the lower part of the vocal cords. The anesthesiologist in charge estimated that intubation would be easier with a succinylcholine (2 mg/kg) injection. Then the patient was successfully intubated with a 2.5-diameter tube. Deep anesthesia allowed the excision of the tumor. Preoperatively, anesthesia was maintained by sevoflurane and remifentanil without myorelaxants. The patient received antibiotic prophylaxis based on amoxicillin and clavulanic acid. Dexamethasone was given at the dose of 1 mg perioperatively to prevent postoperative mucosal edema. The patient was extubated 24 h after the intervention to avoid postoperative bleeding, edema, and laryngospasm. The anatomopathological examination concluded a mature teratoma of the palate. Histological examination confirmed the diagnosis of a mixed mature and immature true teratoma.
There were no complications such as infection, bleeding, or residual recurrence following surgery. The outcome was favorable after complete resection of the tumor and cleft closure. After a 6-month follow-up, there was no recurrence of the teratoma.
Discussion
Teratomas occur in 1 out of 4000 live births. A female predominance of 6/1 has been reported in the literature. 4 Early diagnosis and surgical excision under general anesthesia are the mainstays of treatment. 5 The most important factor affecting the outcome is whether the teratoma could be resected successfully during initial surgery. 6 The airway management of these cases presents a real challenge for the anesthesiologist in charge of the patient. A failed intubation in such a situation can lead to severe life-threatening hypoxemia. Preoperative prediction of the difficulty of the intubation by the CT scan and MRI is imperative to organize a complete strategy for airway management.
Our case report illustrates that predicting a difficult airway in a newborn by clinical evaluation and radiological exams (MRI) allowed us to take necessary precautions for successful neonatal airway management. Even if intubation was performed by conventional laryngoscopy with tracheal manipulation maneuvers under sevoflurane inhalation anesthesia, a complete strategy to manage a failed intubation should be adopted by parents and the team in charge of the patient.
The use of supraglottic devices (laryngeal mask or I-Gel) is contraindicated because of the presence of the tumor. 7 The use of a video-laryngoscope may help more than conventional intubation. 8 The neonatal nasofibroscope is very useful in this situation but it was not available in our department. In case of failed intubation, tracheotomy is a solution to ventilate the patient but it needs a special organization and a ready and experienced otolaryngologist before anesthesia induction. 9
Postoperative airway complications such as laryngeal edema, bleeding, and laryngospasm are expected in such cases. 10 Systemic steroids can prevent mucosal edema. In our case, the steroid was efficient in preventing edema.
Conclusion
In conclusion, neonates’ airways should be managed by a multidisciplinary approach, including an experienced team of an otolaryngologist, an anesthesiologist, and a neonatologist in an institution with adequate infrastructure.
Footnotes
Acknowledgements
None.
Author contributions
A.J. and C.R. conceived the idea of reporting this case; A.J., C.R., S.K., I.M., and F.K. were involved in the management of the patient data collection and interpretation; A.J., C.R., and S.A. wrote the article, R.M., K.K., A.B.T., and N.H. modified the article; and all authors approved the final version for article.
Availability of data and materials
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Statement of informed consent
Written informed consent was obtained from a legally authorized representative(s)for anonymized patient information to be published in this article.