
Abstract
Cutaneous angiosarcomas are rare soft tissue tumours originating from hematogenous vasculature that are aggressive and carry a poor prognosis. We describe the case of a 73-year-old man with a low-grade well-differentiated angiosarcoma. Our case distinguishes itself from those previously reported in the slow progression and important delay to the presentation of 30 months and survival time of 5.5 years. Additionally, its severe clinical appearance (T2 stage) but milder pathological picture (T1 stage) is very uncommon. A repeat biopsy is warranted when results are inconclusive and there is a high clinical suspicion of angiosarcoma.
Introduction
Cutaneous angiosarcomas (cAS) are soft tissue tumours originating from hematogenous vasculature, representing approximately 1% of all soft tissue sarcomas. 1 Of the three main subtypes, cAS of the head and neck, also known as Wilson-Jones angiosarcoma, are the most common. The disease is usually rapidly fatal if left untreated and carries a poor prognosis, with high local recurrence and metastasis rates.2,3 We report a case of cAS demonstrating an unusually slow progression and clinicopathological discrepancy, both reflecting a remarkably indolent course and being uncommon for cAS.
Case presentation
A 73-year-old man presented with a 30-month history of a violaceous rash involving the left side of his face. The lesion expanded from his cheek to his forehead and later became pruritic and mildly painful, prompting him to seek medical attention. Physical examination revealed multiple confluent erythematous to violaceous and brown patches extending from his left frontal region to the left temple, down to the infraorbital area, and occupying the left cheek and zygomatic area. The lesion also extended down to the left submandibular and submental regions where nodules were present, the largest of which measured approximately 3 cm. These nodules were sensitive to light palpation (Figure 1(A) and 1(B)). There was no involvement of the oral cavity and no palpable lymphadenopathy.
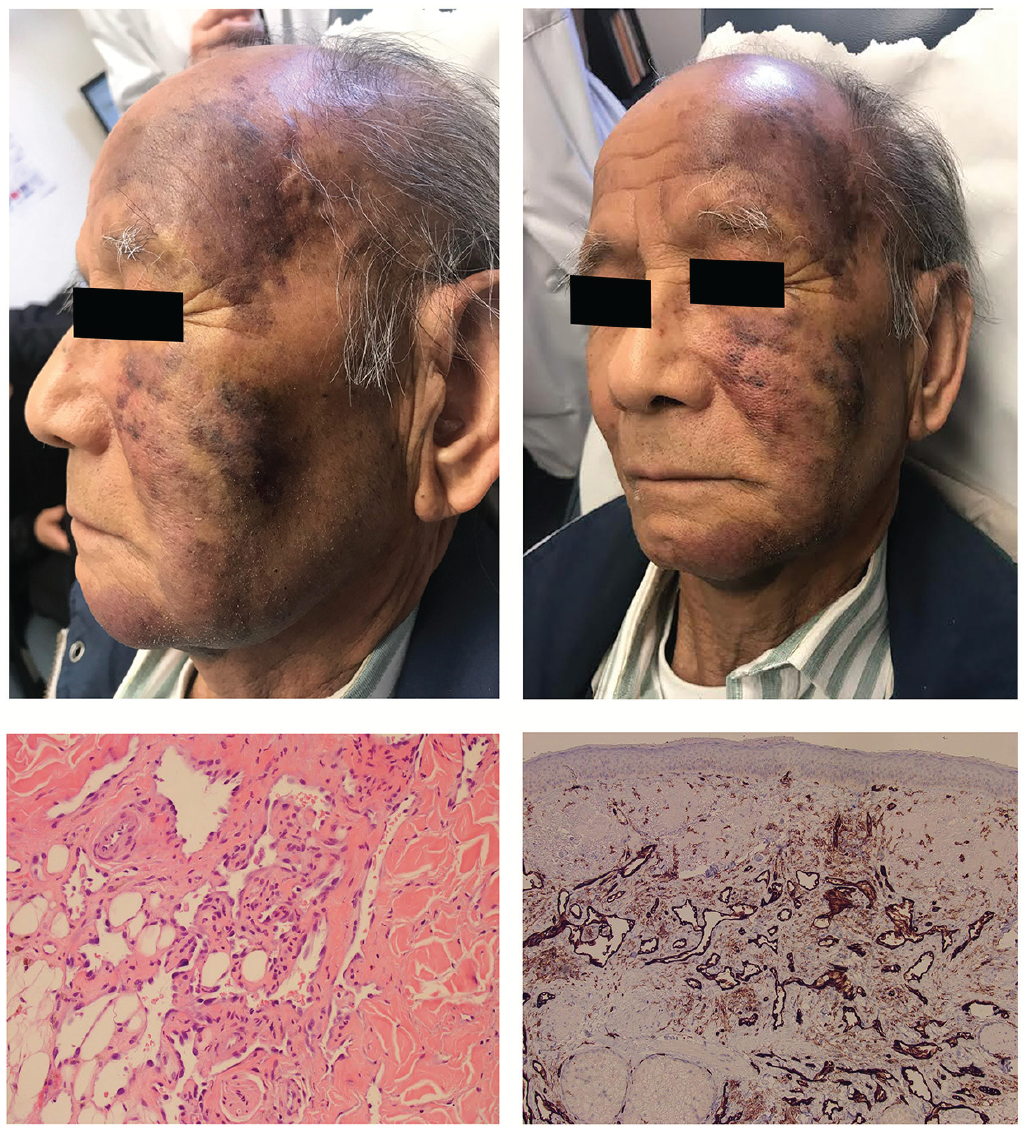
(A) and (B) Clinical photographs of the patient at presentation showing multiple confluent erythematous to violaceous and brown patches extending from his left frontal region to the left temple, down to the infraorbital area, and occupying the left cheek and zygomatic area. The lesion also extended down to the left submandibular and submental regions where nodules were present, the largest of which measured approximately 3 cm. These nodules were sensitive to light palpation (C) Haematoxylin and eosin histopathology at 20× magnification of the second skin biopsy shows an irregular infiltrative pattern of mildly atypical vascular structures present predominantly in the dermis with features highly suspicious of a well-differentiated angiosarcoma. (D) CD31 immunohistochemical stain at 4× magnification highlighting the large irregularly shaped vascular channels.
The first biopsy of the forehead showed mild dermal chronic inflammation with fibrosis and prominent vascular telangiectasia with focal mild endothelial atypia but there were insufficient features of malignancy for the diagnosis of cutaneous angiosarcoma. A second deeper biopsy was taken of the cheek, showing bland infiltrating vascular proliferation with atypical endothelial cells, consistent with a low-grade angiosarcoma (Figure 1(C) and 1(D)).
A diagnosis of cutaneous angiosarcoma was made. Staging studies revealed no nodal involvement or internal organ metastases. The patient underwent radiotherapy and was deemed to be in remission after several months of treatment but developed grade 3 radiation dermatitis with vision difficulties and osteonecrosis of the mandible. After a 6-month follow-up, the extension of the lesion onto the right side of his face was noted, prompting a repeat positron emission tomography scan which showed involvement of cervical lymph nodes. Paclitaxel chemotherapy was initiated and after 6 months of treatment, slight imaging and clinical improvement were seen. Shortly thereafter, the patient was admitted for pneumonia and sadly passed away from related complications, 5.5 years after his initial diagnosis.
Discussion
Clinical presentation of cAS is highly variable in the early stages, usually appearing as a poorly defined bruise-like violaceous indurated macule or plaque and can mimic numerous conditions, 4 which explains frequent delays in presentation. In most reports, patients presented within 2–6 months from onset of symptoms. 2 The disease is rapidly fatal; a study of 72 patients with cAS of the face and scalp showed 50% had died within 15 months of presentation. 5 Five-year survival rates have generally been reported to be between 10% and 30%,2,3,6 but up to 40%–45% per a recent meta-analysis. 1
Contrary to other types of sarcomas, histological grade is not a prognostic factor in cAS.1,7–9 However, certain histological findings are suggestive of worse outcomes, including the presence of necrosis, epithelioid morphology, and deeper invasion, 10 none of which were present in our patient. On histopathology, cAS uncommonly present as low-grade tumours, with one study showing only 6% of cAS being low grade. 10
Tumour size and age of the patient are defined as the most relevant prognostic factors for cAS. 7 Soft tissue sarcoma staging defines tumours smaller than 5 cm as T1, and those larger than 5 cm as T2, the latter carrying the worst prognosis. Our patient presented with a lesion measuring approximately 10 cm by 20 cm. However, this clinical staging method can underestimate the pathological stage. A study conducted on 29 patients with scalp angiosarcoma discussed difficulty with accurate staging, where 18 patients were clinically staged as T1, of which 16 went on to be staged as T2 pathologically. All patients with clinical T2 staging remained T2 in the pathological stage. 2 Our patient’s severe clinical appearance (clinical T2 stage) but a milder pathological picture (pathologic T1 stage) is unusual.
As for age, no clear prognostic threshold has been defined in the literature, rather a general tendency that patients with better response to treatment and survival rates are on average younger than those with worse outcomes. 1
We report this case for its rare slow progression and clinicopathological discrepancy, both reflecting a remarkably indolent course and being uncommon for cAS. This case also illustrates the importance of keeping a high level of suspicion when presented with large pigmentary changes in the head and neck. A repeat biopsy is warranted when results are inconclusive, and there is a high clinical suspicion for angiosarcoma.
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient consent
Informed consent was by the next of kin for the collection and publishing of the non-identifiable images. Upon request, the informed consent form can be provided.