
Abstract
Reactive Infectious Mucocutaneous Eruption is an acute mucocutaneous inflammation secondary to an infection with minimal to absent cutaneous features that has recently been linked to the Severe Acute Respiratory Syndrome Coronavirus-19 (SARS-CoV-19 virus). Unfortunately, the relative rarity of case reports of Reactive Infectious Mucocutaneous Eruption in paediatric populations has led to fewer known successful treatment options with the current mainstay being systemic immunosuppression (e.g. corticosteroids, cyclosporine and etanercept). In this case report, we discuss a case of an adolescent patient with (polymerase chain reaction) PCR+ coronavirus disease 2019 infection and an oral eruption without cutaneous symptoms. He was treated successfully using a single dose of dexamethasone and supportive care through amorphous hydrogel (Intrasite gel), thus providing a safe, cheap and effective treatment option in mild coronavirus disease 2019-associated Reactive Infectious Mucocutaneous Eruption in paediatric patients. We also discuss the current findings, diagnostic terms and treatment options of mucosal manifestations of coronavirus disease 2019 in children.
Introduction
Reactive infectious mucocutaneous eruption (RIME) describes acute mucosal inflammation with minimal to absent cutaneous features following a prodrome of flu-like symptoms. 1 While this used to be considered mainly caused by Mycoplasma pneumoniae infections, recent cases have shown that other viral infections, such as Epstein–Barr virus (EBV) and Herpes Simplex virus (HSV), as well as bacterial infections, can lead to similar presentations. 1 Therefore, other features such as ocular, oral or genital ulcers, a timeline showing a prodrome of an infection (often viral), increased levels of inflammatory marker (e.g. C-reactive protein (CRP), leukocytosis), and minimal to no cutaneous involvement have been used instead to help diagnose RIME cases.
Recently, cases of RIME secondary to SARS-CoV-2 have been reported.2–4 Given the novel nature of this presentation, especially in the paediatric population, there is a lack of evidence in treatment options. The current mainstay of treatment (from adult studies) is immunomodulation through intravenous or oral corticosteroids, cyclosporine or etanercept.2–4
In this report, we discuss a case of a paediatric patient with PCR+ coronavirus disease 2019 (COVID-19) infection and RIME who was successfully treated using a single dose of dexamethasone and local supportive treatment with Intrasite gel.
Case report
A previously healthy 16-year-old male presented to the emergency department (ED) with 2 days of significant oral pain and lip swelling as well as 1 day of conjunctivitis. Due to the significant oral pain, his oral intake was quite poor and needed fluid replacement. Eleven days prior to presentation, he reported a history of upper respiratory illness with nasal congestion, rhinorrhea, sore throat, and cough. Four days after onset of symptoms, he tested positive for COVID-19 via PCR testing. While these symptoms slowly resolved, he started developing erosions on his lower lip which progressed to lip swelling and increased oral pain.
Bloodwork in the ED showed leukocytosis, increased erythrocyte sedimentation rate (ESR) and a mild elevation in troponins. While his electrocardiogram was normal, he was transferred to our hospital for additional workup to rule multisystem inflammatory syndrome in children (MIS-C).
The patient received rheumatology workup which did not corroborate a diagnosis of MIS-C due to the lack of fever, the short latency between the new oral symptoms and his COVID-19 infection, and the normalizing ESR (<28 mm/Hr) and CRP levels (<10 mg/L) within 2 days of admission.
Infectious workup was negative for Group A Streptococcus on throat culture, HSV IgG, Varicella Zoster virus (VZV) swab, Cytomegalovirus (CMV) IgM/IgG, EBV IgM/IgG, and Mycoplasma pneumonia PCR. He also had negative blood cultures and a normal chest X-ray. His only intake of medications consisted of Tylenol for pain relief.
Dermatological examination showed moderate lip swelling with multiple erosions across the lower lip covered with haemorrhagic crust (Figure 1). No other skin lesions were identified. Due to the severity of mucositis, one dose of dexamethasone (0.15 mg/kg) was administered followed by pain management and local wound care with amorphous hydrogel Intrasite gel every 2 h until resolution of the lip erosions.
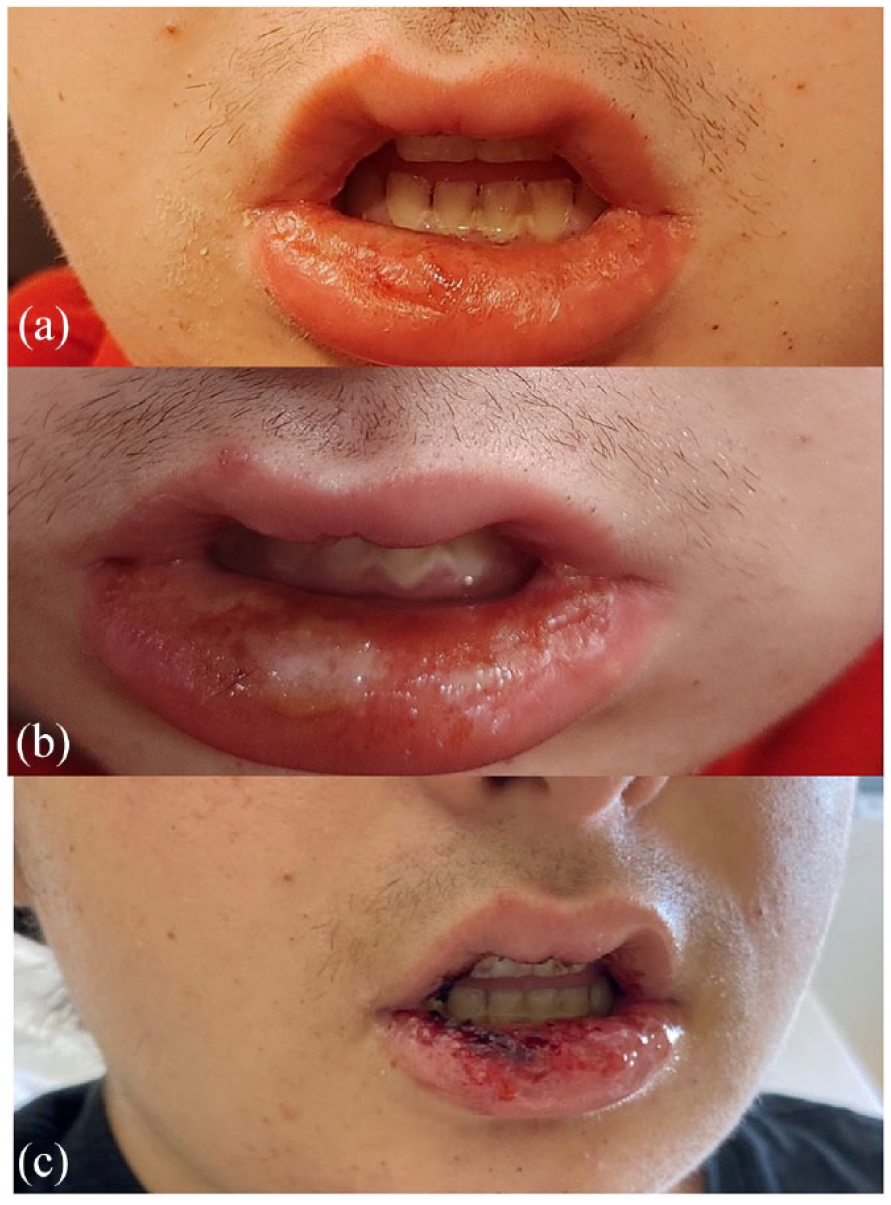
Close-up of the patient’s lower lips at initial onset of mucosal symptoms (a and b) and on presentation to our hospital (c). Pictures showing initial swelling and erythema of the lower lip (a) with the subsequent desquamation and white base erosion (b). Picture C shows the multiple erosions with haemorrhagic crusting seen in ED by our dermatology team.
On follow-up, the patient reported full resolution of his lip erosions and oral pain after 7 days of using Intrasite gel. His lips returned to normal size and completely healed (Figure 2).

Close-up of the patient’s lips post-treatment showing complete resolution of previous lesions and return of normal mucosal epithelium.
Discussion
A brief literature review of COVID-19 mucositis in the paediatric population shows that many have had a similar presentation with a prodrome of respiratory and gastrointestinal symptoms and minimal to no cutaneous features. Currently, three case reports have similarly diagnosed the oral symptoms as manifestations of RIME in COVID-19 patients (Table 1). These reports discuss four cases of adolescent males with oral/penile glans ulcers and conjunctivitis after 4–6 days of an upper respiratory infection prodrome. The latency times between symptoms of COVID-19 infection and mucosal eruptions ranged from 4 to 7 days and resolved in 5 to 24 days.2–4
Summary of COVID-19-associated RIME cases in literature as compared to our case.
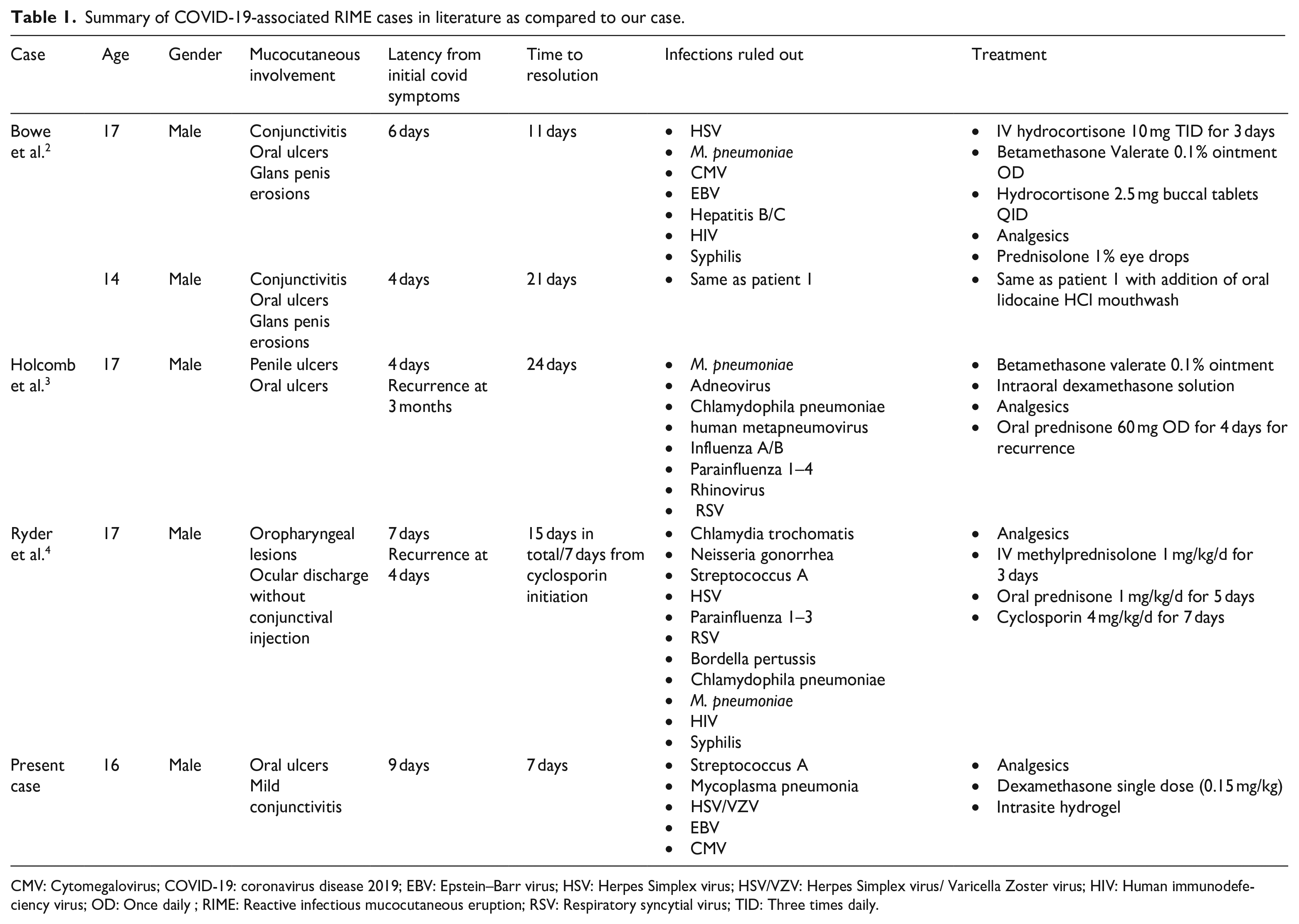
CMV: Cytomegalovirus; COVID-19: coronavirus disease 2019; EBV: Epstein–Barr virus; HSV: Herpes Simplex virus; HSV/VZV: Herpes Simplex virus/ Varicella Zoster virus; HIV: Human immunodefeciency virus; OD: Once daily ; RIME: Reactive infectious mucocutaneous eruption; RSV: Respiratory syncytial virus; TID: Three times daily.
While Bowe’s cases 3 were treated effectively with intravenous hydrocortisone, Betaderm ointment and hydrocortisone tablets, Holcomb’s cases required oral prednisone at 1 mg/kg dosing due to worsening despite Betaderm ointment and intraoral dexamethasone solution, while Ryder’s 4 cases needed a 7-day course of cyclosporin due to worsening symptoms while on IV methylprednisone. Interestingly, Holcomb’s case had a recurrence 3 months later and Ryder’s case had a recurrence after 4 days, suggesting the possibility of recurrence of COVID-19 RIME. Comparison of our case to those in the literature shows that ours was milder in nature, able to be managed with more conservative measures carrying less side effects for the patient.
Intrasite gel has been used frequently in wound management. This is due to its ability to provide hydration to encourage the migration and regrowth of the epithelial layer, as well as to act as a solid structure, able to absorb the sloughed-off necrotic tissue and retain it within the gel until it is cleaned before the next application. 5 Its use has already been observed to be effective in the management of cases of radiation-induced oral mucositis. 6 Additionally, since it is composed of water, carboxymethyl cellulose, and propylene glycol, the Intrasite gel is safe to use in younger patients with the main side effect being gastrointestinal irritation if ingested. The risk of side effects is further decreased by using the applicator to minimize excess product. Compared to the side effects of steroid treatments such as atrophy, irritation, opportunistic infections and mood changes, 7 use of Intrasite gel and other wound care measures in milder cases such as ours may provide the same benefit with less risks.
Although RIME has an excellent prognosis with a self-limiting course, the estimated rate of recurrence is 8% and the sequelae include scarring and pigmentary changes. 4 This patient experienced complete resolution within 7 days following the initiation of one dose of dexamethasone at admission and prompt treatment with hydrogel wound dressing. However, it is also possible that this response may represent a natural resolution of the disease.
Overall, this case report provides further support for the ability of COVID-19 infection to trigger RIME in paediatric patients as well as demonstrates the benefit of using amorphous gels as a safer option for supportive treatment in milder cases.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent
Written informed consent was obtained from the patient’s parents for publication of this case report and any accompanying images.