
Abstract
Cerebral aneurysms secondary to human immunodeficiency virus vasculopathy are a diagnosis by exclusion and its mechanism is unknown. We report on a 21-year-old male with human immunodeficiency virus infection and suboptimal virological control, despite highly active antiretroviral therapy. An incidental discovery of multiple cerebral aneurysms occurred in this patient, who initially presented with signs of disorientation, acute psychosis, and a history of blunt cranial trauma. A non-contrasted computerized tomography scan of the encephalon showed no intracranial hemorrhage but multiple cerebral (saccular and fusiform) aneurysms. Subsequently, a non-urgent computerized tomography angiogram of the cerebral vasculature corroborated the existence of multiple cerebral aneurysms. Despite investigation, no secondary etiological factors for the aneurysmal condition were identified. The multitude of cerebral aneurysms was consequently ascribed to human immunodeficiency virus-associated vasculopathy. The patient was managed conservatively. At discharge, he was lucid and apsychotic. A unique aspect of the case is the presence of both fusiform and saccular cerebral aneurysms.
Keywords
Introduction
Neurological manifestations of human immunodeficiency virus (HIV) include meningitis, encephalitis, central nervous system opportunistic infections and space occupying lesions (toxoplasmosis, tuberculoma, cerebral abscess, and lymphomas), cerebrovascular accidents, and neurocognitive disorders.1–3 Intracranial aneurysms are in general uncommon, with global prevalence estimated at 2.3% with an unknown proportion that is HIV-associated. 4
The exact mechanisms of HIV vasculopathy leading to multiple cerebral aneurysms are unknown. However, it is postulated that HIV directly damages the endothelium and leads to endothelial dysfunction while the circulating infected monocytes, cytokines and abnormal growth may result in altered vascular flow and indirect vascular damage.5,6 In addition, opportunistic infections may play a role in the formation of fusiform aneurysms by increasing the amount of released elastases with subsequent degradation of the internal elastic lamina. 7
HIV-associated cerebral aneurysms remain a diagnosis by exclusion. They were first described in children in the 1980s and adults in 2006. 8 A recent retrospective longitudinal case series of 50 patients, with a cumulative of 82 HIV-related cerebral aneurysms, suggested that patients with a lower CD4 T-cell count and a higher HIV viral load burden may have an increased predilection to both the formation and growth of cerebral aneurysms. 9
We report a case of a 21-year-old male living with HIV who was incidentally found to have multiple cerebral saccular and fusiform aneurysms, presumed secondary to HIV vasculopathy.
Case presentation
A 21-year-old male presented to the emergency department with blunt force trauma to the head, confusion, and acute onset psychosis post-assault. There was no history of loss of consciousness or seizures or similar episodes previously.
He had a background history of being HIV-infected, which was diagnosed 5 years prior and was on a fixed dose combination of antiretroviral therapy for 4 years. He was virologically unsuppressed (923 copies/ml) with a CD4 T lymphocyte count of 623 cells/µL (Table 1). There was no history of HIV-related infections or malignancies. There was also no surgical, psychiatric, or significant family history. He did not have non-infectious risk factors for aneurysm development (i.e., hypertension, tobacco use). On physical examination, he was poorly kempt but comfortable with no stigmata of chronic illness. He had minor lacerations in the left temporal and parietal area and abrasions over the right 3rd and 4th phalanges. He was not orientated to time, place, and person. On mental state examination, he had visual and auditory hallucinations, tangential speech, and an elevated mood. There was no meningism and no clinical signs of cranial nerve dysfunction. Motor examination was normal in both upper and lower limbs. Physical examination of the chest, cardiac and abdomen, and skin were non-remarkable. The initial differential diagnoses entertained intracranial hemorrhage, acute psychosis secondary to traumatic brain injury and possible HIV-related central nervous system opportunistic infections. A primary psychiatric illness was less likely because of a good premorbid function and the acute onset of symptoms after head injury.
Laboratory results.
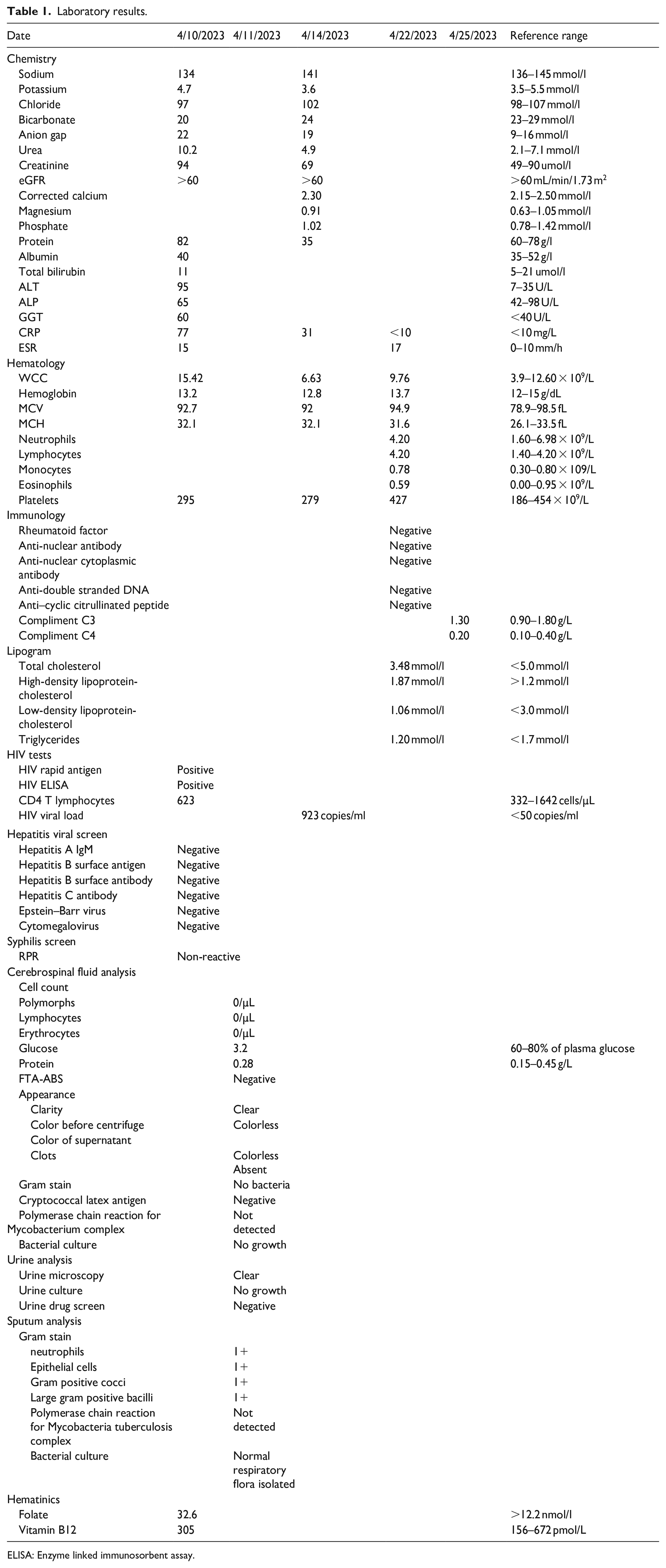
ELISA: Enzyme linked immunosorbent assay.
An emergency-unenhanced computerized tomography (CT) of the brain showed an “impression” of a cerebral aneurysm but did not demonstrate subarachnoid hemorrhage Baseline laboratories showed a raised C-reactive protein of 77 mg/L and elevated white cell count of 15.42 × 109 (Table 1). We proceeded to do a lumbar puncture while awaiting a CT angiogram of the cerebral vessels. Cerebrospinal fluid analysis was normal with no evidence of acute blood loss or xanthochromia and effectively ruled out cryptococcal meningitis, tuberculous meningitis and neurosyphilis (Table 1). The patient made a rapid recovery and was alert and apyschotic after 1 day. His urine screen for substances of abuse were negative (Table 1). CT angiogram revealed multiple cerebral aneurysms (a total of 9) (Figures 1 and 2). An extensive workup for secondary causes of vasculitis revealed no abnormalities other than the HIV infection. (Table 1). Given the association of polycystic kidney disease with cerebral aneurysms, we performed and ultrasound of the kidneys, which were normal with no suggestion of polycystic kidney disease. Angiogram of extracerebral vasculature was not possible because of limited radiological resources. In addition, the patient did not attend his outpatient appointment for carotid dopplers. He was reviewed by the neurosurgical team who elected for conservative management with repeat CT angiogram in 1 year. He remained well throughout admission and at follow-up has not had any psychotic episodes or seizures.

3D Virtual reconstruction of cerebral angiogram: Arrows depicting multiple fusiform and saccular intracranial aneurysms of the bilateral MCA (blue arrows), right ACA (green arrow), left PCA (pink arrow), and basilar arteries (black arrows). Additional variant with aplasia of the right A1 segment of ACA with compensatory ectasia of the left ICA, A1 ACA, and Ant com arteries.

3D Vessel segmentation of cerebral angiogram: Arrows depicting the bilateral MCA (blue arrows). Remaining aneurysm are not appreciated on this reconstruction. Additional variant with aplasia of the right A1 segment of ACA with compensatory ectasia of the left ICA, A1 ACA, and Ant com arteries.
Our final diagnosis was that of multiple cerebral aneurysms secondary to HIV-related vasculopathy.
Discussion
The present clinical case exhibits notable divergences from the recorded instances of multiple cerebral aneurysms consequent to HIV-associated vasculopathy. As a preliminary point of distinction, in the cases chronicled by Tello et al. 10 and Kim et al. 11 the afflicted individuals manifested symptomatic indications correlating with cerebral aneurysms, encompassing manifestations such as headache and cerebrovascular accident. Contrarily, our patient’s multiple cerebral aneurysms were serendipitously discovered, presenting as incidental findings. In addition, our case diverges from the triad of South African cases outlined by Modi et al. 12 where patients were devoid of antiretroviral therapy intervention. In contradistinction, our patient has a confirmed HIV positive status and has been subject to a regimen of antiretroviral therapy for a span of 4 years, antedating the incidental identification of cerebral aneurysms. The third point of distinction involves the presence of both fusiform and saccular cerebral aneurysms concurrently in our patient. This concomitant manifestation, to the best of our scholarly knowledge, remains unprecedented in the existing literature. Predominantly, fusiform aneurysms have been linked with HIV-infection, similar to individuals without HIV-infection.13,14
The underlying etiological factors contributing to our patient’s simultaneous manifestation of both saccular and fusiform aneurysms remain enigmatic. Lastly, the present clinical case reports the presence of nine cerebral aneurysms, the highest reported in the literature is six. 4
Owing to the abundant presence and positioning of the aneurysms, we opted for a conservative approach toward the management of the patient. Our clinical judgment deemed the potential risks inherent in surgical intervention to supersede the prospective benefit. Additionally, given the patient’s virological status—being unsuppressed—we introduced adherence counseling with the aim of amplifying compliance to the antiretroviral therapy regimen.
The medical literature delineates surgical, endovascular, and pharmacological therapeutic strategies, although the substantiating evidence base largely comprises case reports and case series.9,10,15–17 Despite a paucity of definitive treatment guidelines for HIV-associated multiple cerebral aneurysms, there are instances where diligent adherence to antiretroviral therapy has been associated with decelerated aneurysm progression or even reduction in size. 18
A retrospective, longitudinal case series encompassing 50 patients illustrated that inconsistent usage of antiretroviral therapy engenders progression in aneurysm formation and growth. 9 However, limited evidence exists as to whether initiating antiretroviral therapy in those previously uninitiated or non-adherent to treatment might incite an immune reconstitution inflammatory syndrome, thereby potentially stimulating aneurysm progression and growth. 2
Clinical outcomes associated with this condition are particularly adverse in pediatric cases. Adult outcomes remain indeterminable due to lack of data. Median survival duration among children post-diagnosis is approximately 8 months, further shrinking to 5.5 months should cerebrovascular accidents occur. 19
One major limitation of our study is the non-imaging of extracerebral vessels. Given the substantial intra-cerebral aneurysms, additional extracerebral aneurysms that might have been receptive to surgical or endovascular intervention could have been overlooked. However, resource constraints restricted further imaging.
For an all-encompassing understanding, additional research is imperative to elucidate the incidence of HIV-associated multiple cerebral aneurysms, along with the roles of antiretroviral therapy, surgical intervention, and endovascular therapy in ameliorating associated morbidity and mortality.
Conclusion
The occurrence of multiple cerebral aneurysms as a secondary effect of HIV-associated vasculopathy is a relatively infrequent phenomenon, typically identified following the exclusion of alternative etiologies. The precise pathogenic mechanisms orchestrating this condition remain elusive. Therefore, concerted research is necessary to determine the optimal clinical management strategies for this rare but significant condition.
Footnotes
Author contributions
P.N. and S.P. contributed to coordination, writing (original and final draft), reviewing, and editing. Y.N., T.U., and P.H. contributed to writing original and final draft, reviewing, and editing. All authors approved the final version of manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.