
Abstract
Objective:
Health literacy helps an individual to have the capacity to obtain, process, and understand basic health information to make appropriate health decisions. This study aimed to review the association between health literacy and COVID-19 vaccine acceptance.
Method:
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses steps. Databases including PubMed/MEDLINE, Web of Science, Scopus, EMBASE, World Health Organization libraries, and Google Scholar were used to search all published articles in the area of health literacy and COVID-19 vaccine acceptance until August 1, 2022.
Result:
In this review, 1348 articles were retrieved. Finally, 13 articles were included in the review after the removal of duplicates that did not meet our inclusion criteria. In all, 10 articles showed that health literacy was significantly associated with COVID-19 vaccine acceptance. This review also showed that positive perception of the vaccine, vaccine hesitancy, adverse reaction from vaccines, residence, socioeconomic status, level of education, younger age, being a health worker, and positive belief have associations with health literacy and COVID-19 vaccine acceptance. There was significant heterogeneity in the study population and measurement tools used for health literacy and COVID-19 vaccine acceptance.
Conclusion:
This systematic review provides comprehensive evidence on health literacy and COVID-19 vaccine acceptance globally. There was significant heterogeneity in the study population and measurement tools used for health literacy and COVID-19 vaccine acceptance. Most studies reported that health literacy is significantly associated with COVID-19 vaccine acceptance. Therefore, investing in health literacy using different vaccine promotion strategies may improve COVID-19 vaccine acceptance and health decision-making to decrease the impact of the COVID-19 pandemic.
Introduction
A cluster of pneumonia cases in Wuhan, China at the end of 2019 caused a severe acute respiratory syndrome coronavirus 2 disease. The amount and length of exposure, the implementation of preventative measures, and individual characteristics all affect the risk of COVID-19 transfer from one person to another.1,2 COVID-19 spreads via respiratory droplets, close contact with infected individuals, secretions, saliva, and respiratory droplets produced when an infected person talks, sneezes, or coughs. Vaccines are effective and economical, and public health measures against infectious diseases help people develop immunity to a particular disease by stimulating their immune systems. To halt the global spread of the virus, potential COVID-19 vaccines are found and put to the test.2 –5
According to the World Health Organization (WHO), vaccine hesitancy has been identified as one of the top 10 threats to public health in 2019. 6 Vaccine hesitancy is defined as the delay in the acceptance, reluctance, or refusal of vaccination despite the availability of vaccination services. The determinants of vaccine hesitancy result from a complex decision-making process that is influenced by a range of factors at three levels generally: intrapersonal, interpersonal, and community levels, and some related to vaccine-specific factors including communication and media experiences with vaccination, risk perception, design of vaccination program, religion, cultural, gender, socioeconomic, politics, and geographic barriers.7 –9 Studies revealed that the global frequency of COVID-19 vaccine hesitancy was 25%. A higher risk of vaccination reluctance was associated with being a woman, being 50 years of age or younger, being single, being jobless, living in a home with five or more people, having less education than an undergraduate degree, working in a field unrelated to health care, and believing that COVID-19 vaccines are risky.8,10
Vaccine acceptance is defined as “the degree to which individuals accept, question, or refuse a vaccination.” 11 Research has shown that countries with the highest COVID-19 acceptance rates were Nepal and Vietnam (97%), Niger (93%), Ethiopia and Tunisia (92%), and Canada (91) while the countries with the lowest acceptance rates were Iraq (13%), Cameroon (15%), Bahrain (17%), Algeria, Lebanon, and Senegal (21%).9,11 Studies showed that the decision to vaccinate against COVID-19 depends on knowledge, attitudes, and readiness to accept.12 –16 The perceived effects of COVID-19, information, awareness of vaccine immunity, prior vaccinations, and household income were all factors connected to the COVID-19 vaccine acceptance. The most confirmed barriers to COVID-19 vaccination were deficient data regarding the vaccine’s adverse effects (potential, 74.17% and unknown, 56.31%) and insufficient information regarding the vaccine itself (72.76%).14,17 –19
Health literacy (HL) is the degree to which a person can access, process, and understand basic health information and services to make wise health decisions.20,21 It has multiple dimensions, including system requirements and complexity as well as people’s talents and competencies. There are three types of HL. Functional HL refers to the fundamental reading and writing abilities needed to function in daily life; communicative HL refers to the more advanced abilities needed to extract information from various forms of communication and apply it to changing circumstances; and critical HL refers to the more advanced abilities needed to critically evaluate information and use it to exert greater influence.22,23 According to a recent concept analysis, “Vaccine literacy (VL) is a process of providing vaccine information, building communication, and increasing people’s engagement about vaccines. It is considered a part of obtaining vaccine convenience and employing communication strategies.” 24 To grasp and use the information to embrace vaccination, people need to be more motivated and knowledgeable about vaccines. VL is a tool that helps in reducing the adverse effects of having too many misleading reports about vaccination.25–27
HL is a social determinant of health, and poor HL is associated with poor education, poverty, unemployment, and low socioeconomic status, yet those with higher levels of education and income can have low HL. Good vaccine HL is important to alter societal norms in promoting vaccine uptake and establishing a foundation for herd immunity at a level appropriate for each individual’s age, mental capacity, gender, and environment.28 –32 Studies have revealed that people with poor HL had lower health outcomes and higher costs, and people of all ages, races, income levels, and educational levels are affected. The studies revealed that HL is crucial for regulating pandemic-related information and has connections to vaccination habits. Studies have shown that a lack of HL was linked to a poor ability to use the information to accept vaccination.28,30,32 –35
The understanding of health issues and interacting with the healthcare system are both impacted by low HL. Research has demonstrated that low HL is associated with less knowledge, harmful behavior, a higher risk of developing chronic diseases, less ability to control one’s health, and more admissions. To raise public awareness of the effectiveness, safety, and potential side effects of vaccines and foster vaccine uptake, effective vaccine communication is essential. Vaccine efficacy, safety, mechanism of action, immunization schedules, and faith in the healthcare system that promotes and administers vaccines are all factors that influence vaccine confidence. The ability to make informed decisions about the COVID-19 vaccine uptakes is a result of having strong vaccination literacy28,34 –38 Therefore, the purpose of this systematic review was to assess the association between HL and COVID-19 vaccine acceptance.
Methodology
This systematic review assessed the association between HL and COVID-19 vaccine acceptance. It was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Search strategy
To find studies on HL and COVID-19 vaccination acceptability, we searched PubMed/MEDLINE, EMBASE, Web of Science, Google Scholar, and WHO libraries until August 1, 2022.
The search term was developed using the following key terms: “COVID-19 vaccine acceptance” OR “SARS-CoV-2 vaccine acceptance” OR “novel coronavirus vaccine acceptance” OR “coronavirus disease 2019 vaccine acceptance” AND “health literacy *” OR “vaccine literacy.” The search strings were developed using “AND” and “OR” Boolean operators. The search records were first screened by title and abstract, and then duplicates that did not meet our eligibility criteria were excluded. We also manually scanned the references of all articles in which full-text reading was performed so as not to miss additional articles. The review protocol is available on PROSPERO (ID: CRD42022323652).
Inclusion and exclusion criteria
This systematic review includes all articles that meet the following criteria: articles that examine HL and COVID-19 vaccine acceptance were included, whereas articles written in languages other than English, short reports, letters to the editor, and discussions were excluded from the present systematic review.
Eligibility criteria
The inclusion criteria included observational studies with any design (i.e., cross-sectional, cohort, case–control) on HL or VL and COVID-19 vaccine acceptance. Primary articles were selected if published in English, peer reviewed, and when the full text was available. We excluded articles not reporting on HL and COVID-19 vaccine acceptance, data not reliably extracted, duplicate, abstract-only papers as preceding papers, conferences, editorials, author responses, books, and articles without full text.
Data extraction
Articles extracted from search engines were exported to a Microsoft Excel spreadsheet after the removal of duplicates. Studies retrieved using search terms from all databases and additional sources were screened for inclusion criteria. Then, articles that fulfilled the inclusion criteria were undertaken full-text review for admissibility and extraction. The PRISMA flowchart was used throughout all steps.
For each included article, the following information was extracted: author, publication year, country, sample size, sampling method, location of data collection, study design, measures of HL, measures of vaccine acceptance, the relationship between HL and vaccine acceptance, and factors associated with HL and COVID-19 vaccine acceptance. Titles and abstracts of the studies retrieved were screened independently by two review authors to identify all the articles that potentially meet the inclusion criteria. The full text of the eligible studies was retrieved and independently assessed for eligibility by two review team members. Two researchers performed the data extraction. Disagreements were resolved in consensus or by a third reviewer.
Quality assessment
Two review writers independently evaluated the quality of the studies included in this systematic review, and a third reviewer settled disagreements. The Newcastle–Ottawa Scale (NOS) criteria were used for quality assessment to include this systematic review. 39 For observational investigations, this tool provides seven points in each of the three modified NOS component domains. Studies that received five or more points were included. Six of the articles received a quality assessment score of 6, five received a score of 7, and two articles had a score of 5 (Table 1).
Modified NOS regarding star allocation to assess the quality of cross-sectional studies (out of a total of seven stars) included in the systematic review of HL and COVID-19 vaccine acceptance.

NB: Y, yes; N, No.
Data analysis
Descriptive statistics were used to summarize the study’s findings. It was impossible to perform a meta-analysis or best evidence narrative synthesis due to the high heterogeneity in the study population and measuring instruments utilized on study participants to assess HL.
Result
In this systematic review, 1348 articles were retrieved from all searched database sources. After the removal of 406 duplicates, 942 articles were assessed using title and abstract, then 886 articles out of 942 articles were excluded due to not evaluating the outcome of interest in HL or VL and COVID-19 vaccine acceptance. In all, 54 articles were included in the full-text review and then 13 articles were included in the final systematic review. 52 The studies were conducted in 11 countries, with Turkey and Japan having two research each, as well as one study each from Italy, Israel, Singapore, Cortina, Spain, Tunisia, the United States, Iran, and Bangladesh. All studies were performed online, and all of them were cross-sectional study designs. All studies were performed from 2020 to 2022 (Figure 1).

PRISMA flow diagram for a systematic review of HL and the COVID-19 vaccine.
In this study, eight articles used the reliable and validated adult Italian HL tool using the mean VL score. This measure includes 12 questions adapted from a self-reported questionnaire for adulthood vaccination built on the Ishikawa test for chronic noncommunicable diseases, which has already been validated for content and construct. Four items of the questionnaire were aimed at assessing functional VL and eight items evaluated interactive-critical VL according to Nutbeam’s definition.40,41 From the psychometric point of view, functional VL questions were mainly about language, involving the semantic system, while the interactive-critical questions focused more on cognitive efforts, such as problem-solving and decision-making. Each response was rated with a 4-point Likert scale (4—never, 3—rarely, 2—sometimes, 1—often, for the functional questions; 1—never, 2—rarely, 3—sometimes, 4—often, for the interactive-critical questions). The score was obtained from the mean value of the answers to each scale (range: 1–4), with a higher value corresponding to a higher VL level. These variables were treated as numerical, as in previous studies where comparable instruments were employed.42,23,43
Four studies use the European Health Literacy Survey HL (HLS-EU-Q47) questionnaire to assess HL status with each item rated on a 4-point Likert scale for a perceived level of difficulty in the competencies of accessing, understanding, evaluating, and applying healthcare-related information in the domains of health care, disease prevention, and health promotion. The European Health Literacy Survey (HLS-EU, 2009–2012) revealed good construct validity, item-scale convergent validity, internal consistency, and no floor or ceiling effect. Most studies measure current vaccination status with a yes-or-no questionnaire.30,44
One study measured vaccination behavior using a 15-item tool developed from a “5C model” of psychological antecedents to vaccination. Each of the five antecedents, including confidence, complacency, constraints, calculation, and collective responsibility, was assessed by three rating items on a 5-point scale (5—strongly agree, 1—strongly disagree). A mean score of items under each domain was computed, with a higher average score indicating a higher HL level regarding the corresponding HL domains of health care, disease prevention, and health promotion.23,45 The study in the United States measured HL with a modified version of the Single-Item Health Literacy Screener, designed to measure limited reading ability, a principal component of HL. 46
Characteristics of articles included
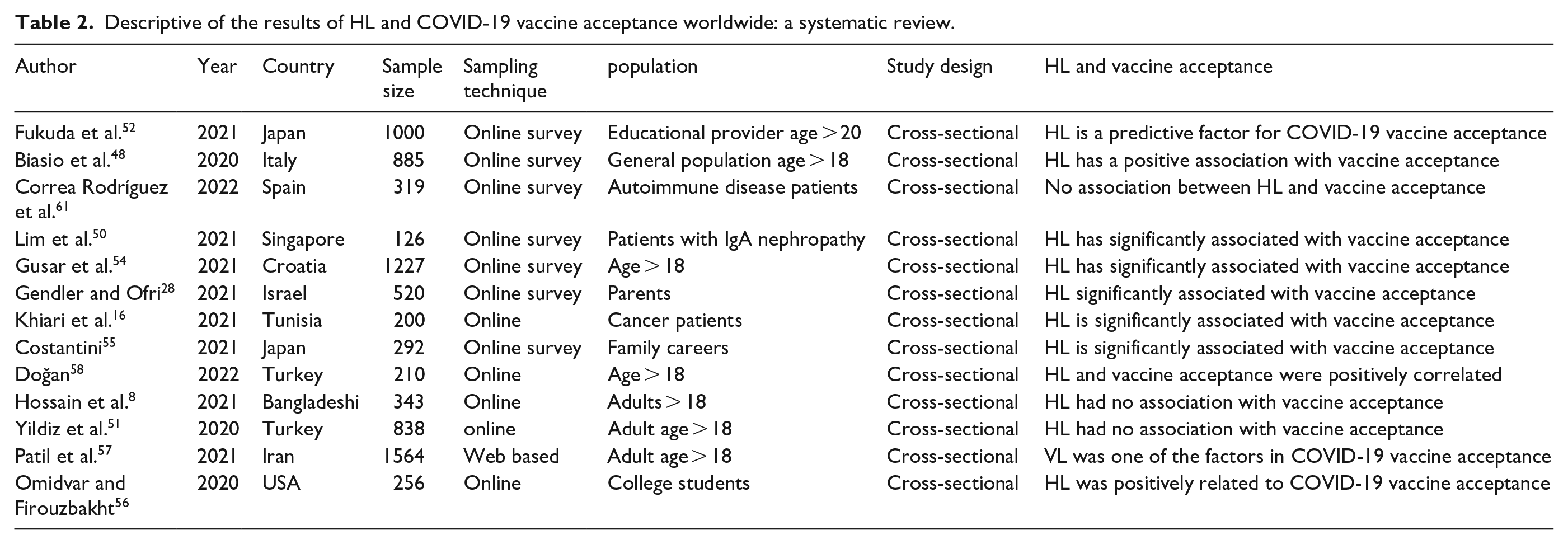
This systematic review included studies on HL and COVID-19 vaccine acceptance published up to August 1, 2022. In all, 13 articles were included in the final systematic review. From the 13 articles, 10 articles showed that HL and COVID-19 vaccine acceptance were significantly associated. Three of the article’s findings showed there is no significant association between HL and COVID-19 vaccine acceptance. There were heterogeneous study participants such as educational providers, general population, autoimmune disease patients, patients with IGA nephropathy, parents, caregivers, and cancer patients (Table 2).
Descriptive of the results of HL and COVID-19 vaccine acceptance worldwide: a systematic review.
The study in Italy explained that the mean score of functional VL was 2.92 ± 0.70 (median 3.0), while the interactive-critical score was 3.27 ± 0.54 (median 3.4), out of a maximum of 4, and the functional VL score was lower in females than males (p < 0.05) while the interactive-critical scores were 3.28 ± 0.55 and 3.26 ± 0.52, respectively. A “limited” VL (score value ⩽ 2.50) was observed in 33% of persons for the functional and 11% for the interactive-critical scale. 47 The research in Spain reported that the mean VL functional and interactive-critical scores were 2.59 ± 0.74 and 3.07 ± 0.60, respectively, out of a maximum of 4. 48
In Singapore, the median general HL index was 31.74 (29.88, 35.82) with significantly greater difficulty in the competency of appraising health information and the domain of disease prevention (p < 0.001). In all, 45 patients (93.8%) received at least one dose of COVID-19 vaccine. The study showed that younger participants <50 years old and those who spoke English at home had significantly higher general HL with 85.4% of participants finding it very easy to find information on vaccinations and understand the need for vaccinations. 49 Research in Turkey revealed that the HL scale total score mean was 54.92 ± 23.64 and from them 56.4% received the COVID-19 vaccine. The total mean scores from the HL scale were found to be significantly higher among civil servants (p < 0.05). 50 The average total HL score for educators was 33.5 ± 7.61 from a study in Japan. 51
In Israel, parents who intend to vaccinate their children had higher mean levels of VL (2.99 ± 0.47 versus 3.07 ± 0.44, respectively, p = 0.06), more positive perception of the vaccine (mean scores of 2.26 ± 0.75 versus 3.44 ± 0.68, respectively, p < 0.001), and lower perceived vaccine hesitancy (7.53 ± 2.37 versus 4.68 ± 2.71, respectively, p < 0.001) than parents who do not intend to do so. 28 The study in Tunisia described that a low VL score (<2.5) was observed among 27.5% and 81.0% participants for functional and interactive-critical scales, respectively. 52
The study in Croatia showed a medium level of VL (M = 2.37, SD = 0.54) and a significant difference between functional and interactive-critical VL (p < 0.001). 53 Among participants, the mean score for VL is slightly lower than for HL (mean of 2.73 versus 2.86, p = 0.004), with a 0.64 correlation. The mean scores across the nine items range for VL from 2.55 to 2.84 and for HL from 2.69 to 2.94. 54 In Iran, 70% of the participants accept COVID-19 vaccines. 55 The study in the United States reported that 49% had adequate HL, 51% had low HL, and 24% of them were compliant with all recommended public health behaviors. Students with low HL were, on average, 2.3 years older than those with adequate HL (p < 0.001). 56
Determinants of HL and COVID-19 vaccine acceptance
The study done in Italy showed that higher educational levels and positive beliefs have a significant association with COVID-19 vaccine acceptance. 66% of the study participants have positive observed attitudes and perceptions on future COVID-19 vaccination, with 73% of participants who were at higher age were willing to take vaccination. 47 Research in Spain reported significant differences were observed between the different education levels, for both the functional and the interactive-critical scores, the highest score was observed in patients who completed a university degree. Observed attitudes and perceptions on COVID-19 vaccines among autoimmune disease patients were mostly positive, with affirmative responses between about 80% and 90% for all questions, except for two questions. It is also especially relevant to the high percentage (96.7%) of patients who have the intention to get vaccinated against COVID-19. The VL interactive-critical score was higher in females than in males while the functional scores were 2.52 ± 0.91 and 2.59 ± 0.72, respectively. Interactive-critical scores were associated with the area of residence, civil status, and socioeconomic status, with the highest score in urban areas of ⩾100,000 inhabitants, in widow patients and in patients with high socioeconomic status. 48
Another study in Turkey showed that the HLS scores of the women and unemployed ones were high (p < 0.05). ATV-COVID-19 scores of those with chronic diseases in their families were higher. (p < 0.05). It was determined that the adult individuals’ HL and attitudes toward the COVID-19 vaccine were positively correlated. 57 The level of VL grew with the level of education (p = 0.031) and reduced with age (p < 0.001). Participants who were employed, had chronic diseases, took medicine, or consumed alcohol daily had a lower level of VL. 53
Gender has a significant relationship with the knowledge of the disease, attitude, and literacy of the vaccine. Marital status was also seen to exhibit a significant relationship with the knowledge of the disease and attitude toward the vaccine. 55 Students with low HL were, on average, 2.3 years older than those with adequate HL (p < 0.001). Students who identified as female or gender variant were roughly twice as likely to have adequate HL than students identifying as male (p < 0.001). Those with low HL were significantly more likely to be first-generation students (p = 0.047). 56
Research in Tunisia discussed that a higher functional VL score was associated with a higher educational level (3.7 ± 0.5 among individuals with a university degree level versus 2.5 ± 1.2 among illiterate, p < 0.001). Interactive-critical VL significantly increased with educational level (p < 0.001) and was significantly higher among healthcare workers (2.5 ± 1.3 versus 1.7 ± 0.9, p < 0.001), those who accepted to get the COVID-19 vaccine (2.0 ± 0.9 versus 1.60± 0.8, p = 0.002), who did not believe that vaccines are unsafe (1.9 ± 0.9 versus 1.40 ± 0.7, p < 0.001), and that there is no need to be vaccinated since natural immunity exists (2.11 ± 0 versus 1.70 ± 0.8, p = 0.016). 52
In Japan, the association was observed between positive behaviors and age (the older the respondent, the more positive the behaviors), gender, physician care status, and HL. Respondents who are male with a history of being under a physician’s care and higher HL had a significantly higher willingness to undergo vaccination. 51
Discussion
WHO identified HL as a key pillar for achieving sustainable development goals in assessing community health and used it as an indicator for assessing population health. This systematic review aimed to review the association between HL and COVID-19 vaccine acceptance worldwide. WHO defines HL as, “the personal characteristics and social resources needed for individuals and communities to access, understand, appraise and use information and services to make decisions about health.” HL promotes and empowers people and communities to participate in their health care, it improves health and well-being, addresses health inequalities, and builds individual and community resilience. HL is one of the vaccine hesitancy determinants along with confidence, complacency, and convenience that can influence vaccine acceptance. HL skills allow patients to take control of their well-being by making smart healthcare choices, improving their communication with doctors, and equipping them with information to advocate for themselves in a medical setting.20,58
The majority of studies found that HL is a significant factor in COVID-19 vaccine acceptance.28,47,50,52,53,55 –57,59 The research also showed that HL is a predictor of vaccine hesitancy, and low HL skills might result in vaccine hesitancy when people find inadequate and inaccurate information about the COVID-19 vaccines on the internet.29,47 The study in Turkey reported that the association between vaccine hesitancy and health system mistrust was mediated by HL. 57
In this review, research findings reported that average VL scores for both the functional and interactive-critical scales were relatively high, and there was a medium level of VL. The review showed the highest interactive-critical scores in females, patients living in an urban area, widow patients, and patients with high socioeconomic status. This is consistent with studies showing that males have lower HL levels than females. 60 The research revealed that study participants who were employed had chronic diseases, took medicine, and consumed alcohol daily had a lower level of VL. The findings showed that unemployed individuals had higher HL and that restrictive measures obliged individuals to spend most of their time at home, consuming large amounts of information, which is quite relevant, and may reflect the fact that interactive-critical HL during the pandemic has often been reported to be higher than the functional HL as if it was stimulated by the COVID-19 infodemic. On the contrary, functional skills may have been challenged by complex terminologies and technical information provided by the media, which may explain the lower functional score, also among highly educated individuals.28,34,35,47,50,53,55,57,59,61 –63
In this review, the highest scores for both functional and interactive-critical scales were found in patients who completed a university degree, supporting that a higher level of education is positively associated with a higher level of VL.53,59,61 This is comparable with studies showing that education is the most determinant factor of HL and those who have a higher level of education have a higher level of COVID-19 VL. 64 According to the review, most patients received at least one dose of the COVID-19 vaccination, and those with high literacy scores are more likely to accept it. 25
According to this review, findings showed that positive perception of the vaccine, vaccine hesitancy, adverse reactions from vaccines, residence, socioeconomic status, level of education, younger age, being a health worker, and positive belief have associations with vaccine HL and COVID-19 vaccine acceptance. This is consistent with studies in which educational level, perceived social status, financial deprivation, unemployment, and economic capacity were found to be determinants of VL and COVID-19 vaccine acceptance.23,37,41,43,51 The possible reason might be these factors influence a person’s ability to access and comprehend medical information that aids in making informed decisions about accepting the COVID-19 vaccine. In this review, perception of the vaccine and fear of side effects were determinant factors of vaccine acceptance. This finding was similar to the findings in previous studies demonstrated that low vaccine uptake can be influenced by perceptions and misconceptions about vaccine efficacy, adverse effects, and vaccinations causing disease.65,66
Limitations
This review is not without limitations. Most of the studies were cross-sectional that could not show the cause–effect relationship. Due to the heterogeneity of study participants, a meta-analysis was not done. We had selected studies published up to mid-2022 which may have left relevant literature on the subject.
Conclusion
This systematic review provides comprehensive evidence on HL and COVID-19 vaccine acceptance globally. Most studies report that HL was significantly associated with COVID-19 vaccine acceptance. Those with good HL are generally able to manage their health more effectively than those without. Therefore, investing in HL using different vaccine promotion strategies may improve COVID-19 vaccine acceptance and health decision-making to decrease the impact of the COVID-19 pandemic.
Footnotes
Acknowledgements
Not applicable.
Author contributions
ETF, TFA, and MGT had the idea for the study and designed the study. AM, BG, AA, ZA, and LW searched, screened, and extracted the data. NK, EK, and BGA analyzed the data. ETF and TFA wrote the first draft of the article. MGT, NK, LW, BGA, AM, ZA, and EK, AA, and BG reviewed and edited the article. All authors approved the final article to be published; agreed on the journal to which the article had been submitted; and agreed to be accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Not applicable.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Not applicable.