
Abstract
Necrotizing fasciitis (NF) is a rare but life-threatening soft tissue infection that spreads rapidly along the fascial planes, causing extensive tissue necrosis and high mortality. Necrotizing fasciitis can be caused by various types of bacteria; the majority of cases are polymicrobial infections. However, necrotizing fasciitis caused by a monomicrobial infection, such as Escherichia coli, is rare. Necrotizing fasciitis can affect any part of the body, but the most common sites are the lower extremities, abdominal wall, and perineum. Necrotizing fasciitis secondary to a perirectal abscess is uncommon and poses a diagnostic and therapeutic challenge. We report a case of a 75-year-old male patient who developed type 3 necrotizing fasciitis of the left gluteal region and left thigh secondary to a perirectal abscess. The patient presented to our hospital with severe pain, swelling, erythema, induration, and fever. He was diagnosed with necrotizing fasciitis based on clinical and radiological findings. He showed gradual improvement and was discharged after 28 days of hospitalization.
Introduction
Necrotizing fasciitis (NF) is a critical, uncommon, and extremely deadly infection of the soft tissue. 1 The condition is marked by a gradual advance of necrosis and swelling, starting in the subcutaneous fat, muscles, and fascia, and ultimately extending to nearby skin. 2 Manifests in the scrotum, perineum, abdominal wall, or limbs. 1 Early identification is difficult, and effective treatment is even more challenging. 3 NF is classified into four types according to microbiological observations. Type I (70%–80%) arises from a polymicrobial infection, type 2 (10%–20%) is a monomicrobial infection typically involving beta-hemolytic Streptococcus A, often associated with Staphylococcus aureus. Type 3 is a monomicrobial infection caused by Clostridium species or Gram-negative bacteria, and type 4 results from fungal infections. 1 However, coexisting conditions such as diabetes, immunodeficiency, trauma, blood disorders, or liver cirrhosis heighten the risk of this infection. 4 NF and myonecrosis resulting from Escherichia coli are exceedingly rare infections with a high mortality rate. 5
Due to its low occurrence, at about three cases per 100,000 people-year, and early symptoms often resembling benign cellulitis, this infection can lead to misdiagnosis or delayed treatment, adversely affecting patient outcomes. 6 Prompt identification, immediate broad-spectrum antibiotic treatment, and urgent, extensive surgical removal of affected tissues are vital to reduce morbidity and mortality from these fast-progressing infections. 6
Case description
A 75-year-old male with no significant medical history, a nonsmoker, underwent drainage of a left ischiorectal abscess on September 4, 2023 due to tension pain exacerbated by defecation lasting 5 h, purulent discharge, difficulty walking, chills, and pain alleviated by rest. Following drainage, he experienced left lower limb swelling, pain, skin discoloration, and fever. Despite an unspecified antibiotic prescription post-drainage, there was no improvement. Ten days later, he presented to our hospital with severe pain extending from the lower back to the left thigh, scoring 10/10 on a visual analog scale.
The examination revealed disproportionate pain with redness, hotness, bilateral lower limb pitting edema (more prominent on the left), severe tenderness, flushing, and a temperature of 40°C. No cyanosis or black discoloration was noted. The patient was referred to our hospital to rule out deep vein thrombosis (DVT) and sepsis.
See Table 1 for test results in lab where blood culture was done, which showed no bacterial growth; nasopharyngeal culture showed extended-spectrum beta-lactamase Klebsiella growth, and a urine culture showed no growth.
Initial laboratory findings on admission.

ESR: Erythrocyte sedimentation rate; HR: heart rate.
The patient underwent angiography and computed tomography (CT) to rule out DVT, and his lower limb venous system appeared patent without any filling defect.
A contrast-enhanced CT scan revealed a fluid collection in the left pararectal fossa, measuring ~9 × 5.5 cm. The collection extended into surrounding regions, including the ischioanal fossa, perianal, and left gluteal areas, descending into the posterio-lateral compartment of the left thigh, reaching the posterior aspect of the knee. Multiple hypodense collections with gas tracing between fascial planes were observed, suggesting NF secondary to a perirectal abscess. The patient was diagnosed with NF based on these findings (Figures 1 and 2).

(a) The collection extends into the ischioanal fossa, perianal, and left gluteal region. (b) There is a fluid density collection with rim enhancement seen in the left peri-rectal fossa, displacing the rectum to the right side. The collection measures about 9 × 5.5 cm (arrow colors are nonsignificant).
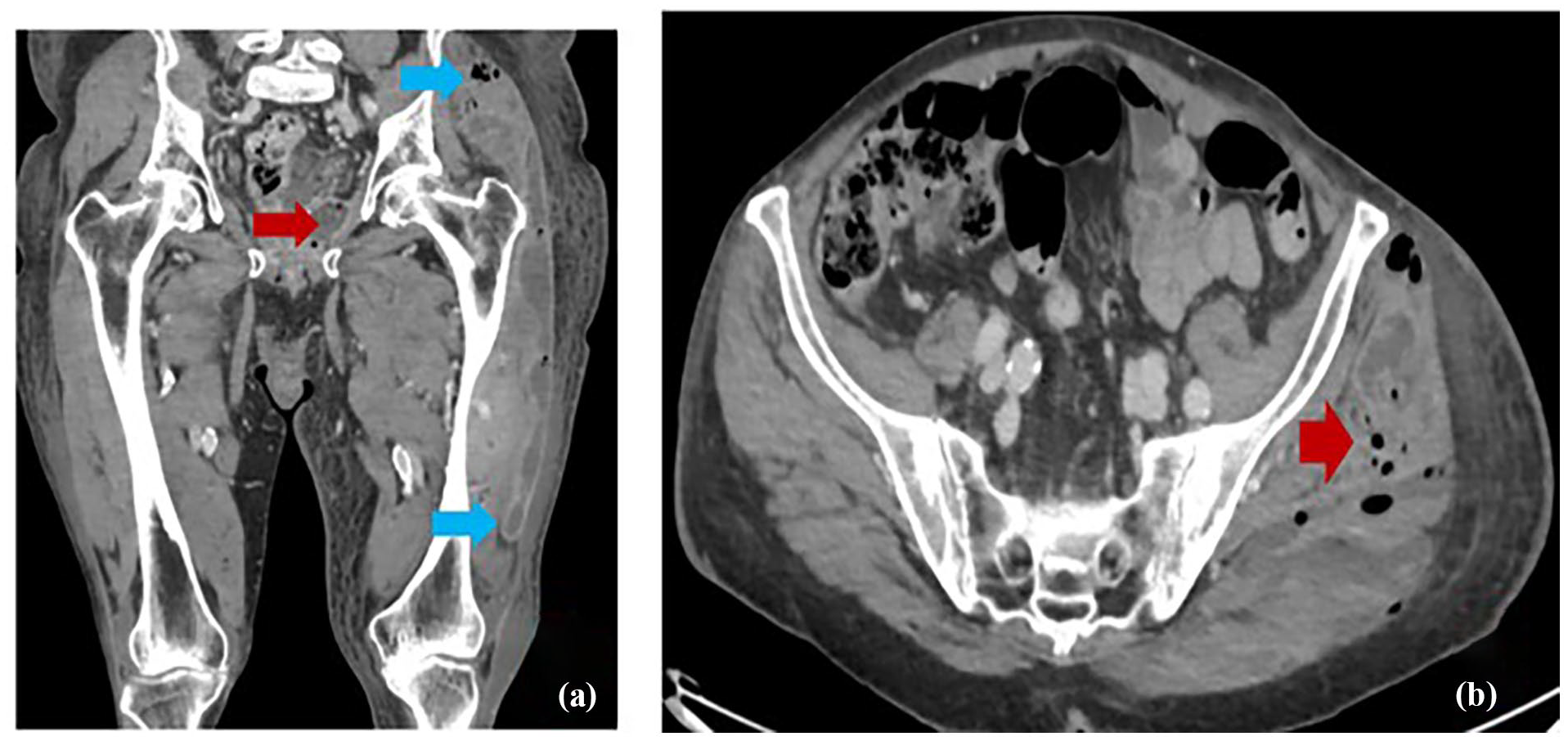
(a) The collection in left gluteal region. (b) Further descends inferiorly into the posterio-lateral compartment of the left thigh. There are multiple surrounding hypodense collections insinuating between muscles, associated with smudging of fatty planes and subcutaneous edema (arrow colors are nonsignificant).
On the day of admission (September 14), the patient underwent extensive debridement for severe NF, extending from the left peri-anal area to the iliac bone and posterior knee, under general anesthesia. Swab cultures were taken from the rectum and debrided tissue. Additional debridements were performed on September 15 and 17. On September 15, a loop colostomy was done due to fistula formation, mild pelvic serous fluid collection, and inflammation in the distal rectum and distal sigmoid diverticulosis. Wound closure and drain insertion occurred on September 24.
The swab culture from the debrided tissue showed growth of E. coli, which is sensitive to tazobactam antibiotic, rectal swab culture showed no growth.
The patient was admitted to the ICU and received broad-spectrum antibiotics (tazobactam 1 mg every 12 h, vancomycin 1 g every 12 h). After the culture results, the tazobactam dose was increased to 3.75 mg four times daily. In addition, he got analgesics, antipyretics, furosemide (40 mg every 12 h), Low molecular weight heparin (clexane; 30 mg every 12 h), and fluid resuscitation. With gradual improvement and wound healing, he transitioned from the ICU to the surgical department 9 days later.
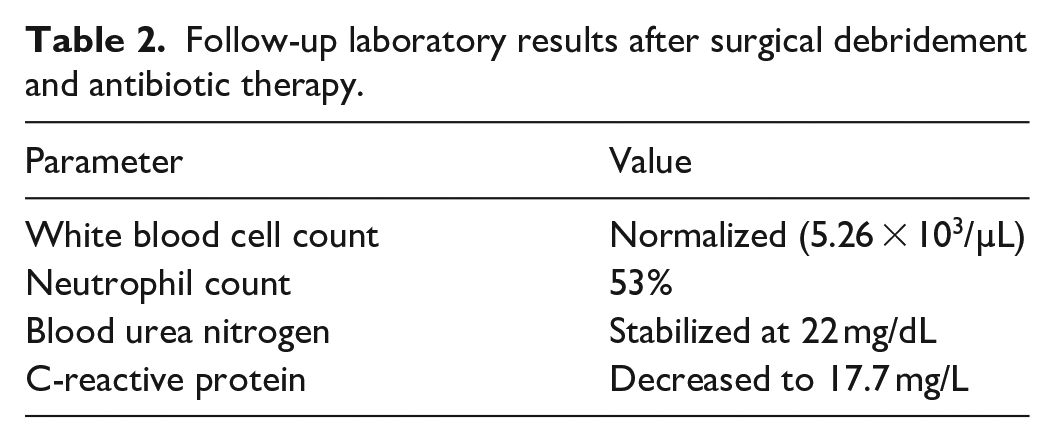
After debridement, antibiotics, and physiotherapy, his daily improvement reflected in better laboratory results. Six days later, his labs were improved (Table 2).
Follow-up laboratory results after surgical debridement and antibiotic therapy.
He was discharged 3 days later on oral antibiotics. Follow-up at the outpatient clinic was recommended for wound care and colostomy reversal.
Discussion
NF is a type of soft tissue infection that can progress quickly and aggressively. Diagnosis of NF can be challenging as it primarily depends on clinical signs. NF has the potential to affect any part of the body, but it is more common in the lower limbs, abdominal wall, and perineal region. 7
This case is unique in several ways due to the atypical presentation of NF. It is noteworthy that the patient did not have any significant medical history or common risk factors associated with NF, such as diabetes mellitus, immunosuppression, or a history of trauma. 4
Furthermore, the individual demonstrated a unique manifestation of NF, marked by swelling in both lower extremities and a slow heart rate. In addition, the individual suffered from an uncommon variant of NF, specifically type 3, caused by a monomicrobial E. coli infection. This particular form is linked to a significantly high fatality rate, estimated between 30% and 40%. 8
The patient’s NF extensively impacted not only the perineal and gluteal areas but extended to the rear part of the left knee as well. Also, there was a delay in diagnosing the condition as initial efforts were focused on excluding sepsis of unknown origin and DVT. This led to a complex progression of NF, necessitating several surgical debridements, the creation of a loop colostomy, wound closure procedures, and an extended course of antibiotic treatment.
In spite of these obstacles, the patient gradually recovered and was discharged after a 28-day stay in the hospital. This positive outcome can be ascribed to several key factors. Initially, we kept a vigilant lookout for NF and swiftly proceeded with surgical intervention as soon as the diagnosis was established. Second, we administered broad-spectrum antibiotics effective against both aerobic and anaerobic bacteria from the start, adjusting the dosage based on culture findings. Third, we ensured supportive care that included fluid resuscitation, hemodynamic monitoring, and nutritional support. Fourthly, the patient’s care involved a collaborative effort from a multidisciplinary team, including surgeons, intensivists, infectious disease experts, wound care nurses, and physiotherapists. Our case underscores the critical need for high vigilance regarding NF and the consideration of unusual sources of infection, such as perforated malignancies.
Conclusion
NF resulting from a perirectal abscess, though uncommon, is a severe condition demanding immediate recognition and assertive management. Swift surgical action, appropriate antibiotic treatment, and comprehensive supportive care are crucial in minimizing complications and reducing the risk of death.
Footnotes
Acknowledgements
The authors express profound gratitude to the Polytechnic Medical Students’ Research Association (PMRA) for their invaluable contributions and unwavering support that significantly enriched every stage of the research journey.
Ethical considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for publication
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article, including accompanying images.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data supporting the findings of this study are readily available within the article.