
Abstract
Intravenous recombinant tissue plasminogen activator is not recommended for the treatment of acute ischemic stroke in patients with infective endocarditis due to the risk of hemorrhagic transformation of septic emboli and few reported cases in the literature. Here, we present the successful outcome of intravenous recombinant tissue plasminogen activator administration for a patient with acute ischemic stroke who was later found to have infective endocarditis. This case adds to the small number of cases reported in the literature.
Introduction
Stroke is a frequent presentation in emergency departments, and it is the third leading cause of death in Canada, according to the Canadian Stroke Best Practice Recommendations. 1 Intravenous alteplase is recommended for selected patients who present with ischemic stroke within 4.5 h of symptoms onset. 2 One of the contraindications to acute stroke thrombolysis is the presence of symptoms consistent with infective endocarditis. 2
Case presentation
A 65-year-old man presented to our emergency room with a history of muscular pain in the back of the neck 6 days prior. He complained of generalized fatigue and weakness after receiving nonsteroidal anti-inflammatory drugs (NSAIDs) for his pain, poor oral intake with no weight loss, and loose motion. He had no other significant gastrointestinal or cardiorespiratory symptoms. His general physical examination showed no significant abnormalities apart from dehydration and jaundice. His heart sounds were normal with no added murmurs. He was found to have a temperature of 39.7 C, and blood work showed increased creatine kinase 1113 U/L (normal 10–170 U/L), troponin T high sensitivity 38.28 pg/mL (normal 0–20 pg/mL), aspartate aminotransferase 72.1 U/L (normal 5–40 U/L), alanine aminotransferase 57.9 U/L (normal 5–40 U/L), total bilirubin 41.7 µmol/L (normal 2–20 µmol/L), direct bilirubin (15.5 µmol/L; normal less than 5.1 µmol/L), and white blood count 7.13 × 10³ (normal 4–10 × 10³). There was no clear consolidation on his chest X-ray. His ECG showed a normal sinus heart rate of 95 bpm and left axis deviation with no ischemic changes. His past medical history was significant for hypertension, diabetes mellitus, chronic renal impairment (baseline creatinine 110 µmol/L; normal: 60–120 µmol/L), obesity, metabolic syndrome, obstructive sleep apnea on continuous positive airway pressure, cervical and lumbar spondylosis, and G6PD deficiency.
He was admitted as a case of fever with jaundice that may have been an infection-related hepatic dysfunction or a hemolytic episode after NSAID treatment in a G6PD-deficient patient. The virology screen was negative alongside other autoimmune screens for liver disease. He was started on Ceftriaxone at 2 g OD after taking a blood culture. He displayed no more high temperatures after his admission to the general medical ward.
Two days later, returning from the washroom with the aid of nursing staff, he suddenly became unconscious. He was unresponsive, with no seizure activity. His vital signs (including heart rate, rhythm, and blood pressure) were normal. He had normal blood glucose when checked. He had left hemispheric syndrome with severe hemiparesis on the right, gaze deviation to the left, global aphasia, hemianopia, and hypoesthesia. The patient’s National Institutes of Health Stroke Scale (NIHSS) score was 18. Urgent computed tomography (CT) of the brain was arranged and showed no acute changes.
His clinical picture was judged to be related to left middle cerebral artery (MCA) ischemic stroke. Informed consent was collected from his next of kin, and intravenous recombinant tissue plasminogen activator (IV r-tPA) was administered according to the standard protocol. Onset to the needle was 30 min. He was kept under supervision in the intensive care unit (ICU).
The next day, follow-up CT of the brain showed the new ischemic infarct in left postcentral gyrus, left cerebral peduncle, and left thalamus with no hemorrhagic changes. On the same day, his blood culture, which was taken 3 days prior upon on his admission, was positive for Gram-positive Streptococcus species. Gentamicin 80 mg TID was added to his antibiotics.
Bedside and departmental transthoracic echocardiography (TTE) was performed 4 days after the stroke, followed by transesophageal echocardiography (TEE), which showed a large vegetation attached to the annulus of the posterior leaflet of mitral valve (PML), measuring 14 × 12 mm (Figure 1). There was mild to moderate mitral regurgitation with an eccentric jet.
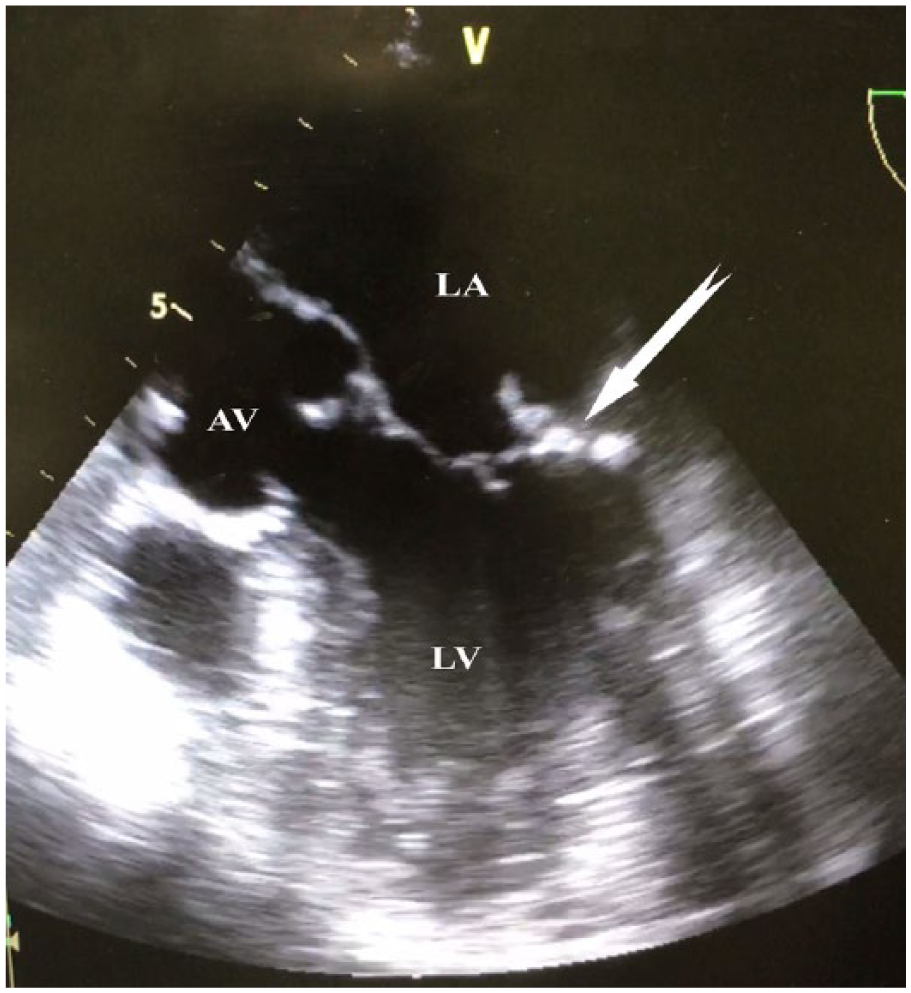
Transesophageal echocardiography showing vegetations attached to the annulus of the posterior leaflet of the mitral valve.
Blood culture showed the definitive growth of Streptococcus agalactiae (Lancefield group B streptococcus (GBS)). He was put on combined therapy of Gentamycin for 2 weeks and Vancomycin for 6 weeks.
A follow-up TEE 8 weeks later showed no evidence of fresh vegetations or abscess. There was no evidence of hemorrhage or mycotic aneurysms on a follow-up CT of the brain (Figure 2). Brain magnetic resonance imaging (MRI) and CT angiography was not done in our hospital as the service was not available. His neurological deficits at that time were speech difficulties and right hemiparesis requiring a cane to ambulate.

Follow-up brain CT scan showing the newly developed ischemic area (arrow) with no hemorrhage.
Discussion
The incidence of stroke in patients with infective endocarditis is approximately 10% and can result either from embolic infarction or hemorrhage. 3 Ischemic stroke is more frequently observed than hemorrhage.4 Septic emboli causing pyogenic arteritis and mycotic aneurysm underlie most intracranial hemorrhages during uncontrolled infection. 4 The vegetation in ischemic stroke is composed of platelets, fibrin, microorganisms, and inflammatory cells, as well as leaflet disruption. 5 Thus, fibrinolytic therapy may be helpful in resolving the embolus that includes the fibrin from vegetation or new fibrin that may develop after embolization.
The safety and outcomes of thrombolysis in infective embolic stroke remain a matter of debate. Patients with infective endocarditis are not recommended for thrombolytic therapy of acute ischemic stroke (Class III, level of evidence C). 6 Walker et al. 7 reported 18 cases in a retrospective, descriptive case series of infective endocarditis-related stroke with a mortality rate of 75% for those who received thrombolysis. The conclusion was that thrombolytics in patients with IE-associated stroke were associated with very poor outcomes. There have been four reported cases of thrombolysis in ischemic stroke secondary to infective endocarditis, two of them intraarterial and two intravenous, with good clinical responses. 8 In a review of 15 case reports with embolic infective endocarditis, the use of mechanical thrombectomy with or without adjuvant thrombolytics in such situations was reported in 7 cases. 9 Interestingly, none of the reported cases showed any intracerebral hemorrhage, and the clinical outcome was good. On the other hand, eight cases received intravenous thrombolysis, and about half of the patients suffered intracerebral hemorrhage, which might be associated with the use of thrombolytics or preexisting mycotic aneurysms. 9
We describe the management of ischemic stroke in a patient with a single recording of fever who was found later to have infective endocarditis based on blood cultures and echocardiography. The decision to treat him with r-tPA was based on clinical grounds and risk-benefit balance considering the timely presentation and intervention. The main treatment for infective endocarditis is to start early effective antibiotic therapy as soon as possible to reduce the mortality and morbidity from embolic complications and heart failure. However, there has been no comparative research or consensus statement on how to manage ischemic stroke patients with large vessel occlusion due to infective endocarditis. The case also illustrates the need for dedicated departmental echocardiography in evaluating patients with ischemic stroke and looking for potential etiologies.
The successful treatment of acute ischemic stroke with IV r-tPA in our case adds to the limited body of knowledge related to thrombolysis in patients presenting with acute ischemic stroke in the setting of infective endocarditis. Future decisions on thrombolyzing infective endocarditis patients presenting acutely with ischemic stroke should not be made based on this case, but rather it would create a base, with other similar case reports, for future more accurate recommendations related to thrombolyzing patients with infective endocarditis.
Conclusion
Thrombolytic therapy in cases of stroke due to infective endocarditis manifesting with major neurologic deficits is a subject of controversy and requires careful evaluation in a randomized trial. The beneficial effects of therapy can be greatly jeopardized by the serious complications of intracranial hemorrhage.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval to report this case was obtained from Ahmadi hospital Ethics committee.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article. The patient had decisional capacity to give informed consent.