
Abstract
Liposarcoma is a carcinomatous mesenchymal tumor with various histologic features and is the most common soft tissue sarcoma originating in adipose tissue. Liposarcoma commonly occurs in the lower extremities and retroperitoneum but rarely in the mediastinum, specially extending into the thoracic cavity. We report a giant primary liposarcoma of the posterior mediastinum in a 63-year-old female who complained of cough, sputum, and pain in the right chest wall. A computed tomography scan of the chest showed a giant mass of 24 × 15 × 24 cm in the posterior mediastinum of the right thoracic cavity. After a thorough examination, no suspected lipomatous lesions were found elsewhere in the patient’s body. The patient underwent a thoracotomy to remove the mediastinal mass through a right thoracic approach. Subsequently, hematoxylin–eosin staining revealed dedifferentiated liposarcoma (DDL), immunohistochemistry showed positive expression of cyclin-dependent kinase 4, and murine double minute 2 (MDM2), in addition, fluorescence in situ hybridization for the MDM2 gene was also positive, which suggested DDL. The patient was discharged without any complications, and no metastasis or recurrence was observed after 19 months of follow-up. To provide a reference for clinical diagnosis and treatment, we reviewed and discussed the literature on primary liposarcoma of the mediastinum.
Introduction
Primary mediastinal liposarcoma (PML) is an extremely rare disease with only 95 cases previously reported in the English literature, which account for 0.1%–0.75% of all mediastinal tumors, 1 and it can grow slowly and remain asymptomatic for several years. PML is usually asymptomatic until large enough to compress intrathoracic structures, causing dyspnea, chest pain, hoarseness, and superior vena cava syndrome. 2 The prognosis for liposarcoma is independent of tumor size, sex, and age. Histopathologic type may be the most important factor in determining the survival of patients with liposarcoma. 3 However, their clinicopathological features remain to be fully elucidated.
Here, we present a giant primary dedifferentiated liposarcoma (DDL) of the posterior mediastinum in a 63-year-old female and conduct a literature review to summarize the clinical presentation, radiographic characteristics, histopathological findings, management, and prognosis of PMLs.
Case presentation
A 63-year-old female patient presented to our hospital with persistent dull pain in the right chest wall for 1 day. During the disease, the patient complained of intermittent cough, expectoration, and post-activity shortness of breath for a month. The patient denied a history of other diseases or surgery. Auscultation of the chest revealed dullness in the right lower lung and decreased breath sounds. Chest X-ray showed a huge mass-like opacity in the right thoracic cavity (Figure 1(a)). A contrast-enhanced computed tomography (CT) scan revealed a large (24×15×24 cm) mass that occupied the posterior mediastinum, extending into the right thoracic cavity and compressing the lower lobes of both lungs into atelectasis. The diaphragm was also compressed and moved down (Figure 1(b)). The mass was heterogeneous in density (Hounsfield Unit, −22 to −109), with variable proportions of fat, soft tissue, and myxoid tissue. The patient underwent tumor resection through video-assisted thoracic surgery. The mass was closely related to the phrenic surface of the right lower lung and esophagus, approximately 24×15×24 cm in size, solid with an intact capsule, and extended through the posterior mediastinum to the right thoracic cavity. There was no adhesion between the tumor and the right lung. However, the esophageal and thoracic ducts were locally surrounded by tumors. The basal nutrient vessels of the tumor were ligated at the level of the mesoesophagus, and complete surgical excision with radical lymph node dissection was also performed. Grossly, there was an irregular mass with a size of 25×18×13 cm, and the cut surface of the excised tumor was multinodular with a diameter of 2–15 cm, with a well-defined gray-yellow solid part or gray-red solid translucent part (Figure 2). Well-differentiated components may be found microscopically. For example, the adipocytes varied in size, and atypical interstitial cells were observed within the fibrous septum (Figure 3(a) and (b)). Most importantly, dedifferentiated components were found morphologically, fibroblast-like cells were predominant at a relatively low density, and myxoid degeneration of the interstitium was observed with a plexiform microvascular structure. A few fat vacuoles were present focally, nuclear atypia was mild to moderate, the mitotic rate was less than 5 per 10 high-power fields, which was classified as French Federation of Cancer Centers grade 2, and necrosis was rare (Figure 3(c) and (d)). Immunohistochemistry (IHC) analysis was strongly positive for cyclin-dependent kinase 4 (CDK4) (Figure 4(a)), and murine double minute 2 (MDM2) (Figure 4(b)), slightly positive for Ki-67 (Figure 4(c)), p16 (Figure 4(d)), and protein S-100 (Figure 4(e)), and negative for smooth muscle actin and MUC-4(-). Moreover, MDM2 gene amplification was positive by fluorescence in situ hybridization (FISH; Figure 4(f)). These findings suggested a diagnosis of DDL. Considering that no suspected lipomatous lesions were found elsewhere in the patient’s body, the final diagnosis was primary DDL of the posterior mediastinum. The postoperative course was uneventful, and the patient was discharged on postoperative Day 12. During the outpatient follow-up, the patient underwent an enhanced CT examination of the whole chest and abdomen, and a magnetic resonance imaging examination of the brain, no evidence of recurrence was identified as of 19 months postoperatively, without any adjuvant therapy.

Chest images. (a) Chest X-ray showed a huge mass-like opacity in the right thoracic cavity (arrow). (b) CT scan revealed a large (24 × 15 × 24 cm) mass that occupied the posterior mediastinum, further extended into the right thoracic cavity and compressed the lower lobes of both lungs into atelectasis; the diaphragm was also obviously compressed and moved down.

Gross appearance of the resected tumor. Grossly, there was an irregular mass with a size of 25 × 18 × 13 cm. The cut surface of the excised tumor was multinodular with a diameter of 2–15 cm, which was a well-defined gray-yellow solid part or gray-red solid translucent part.
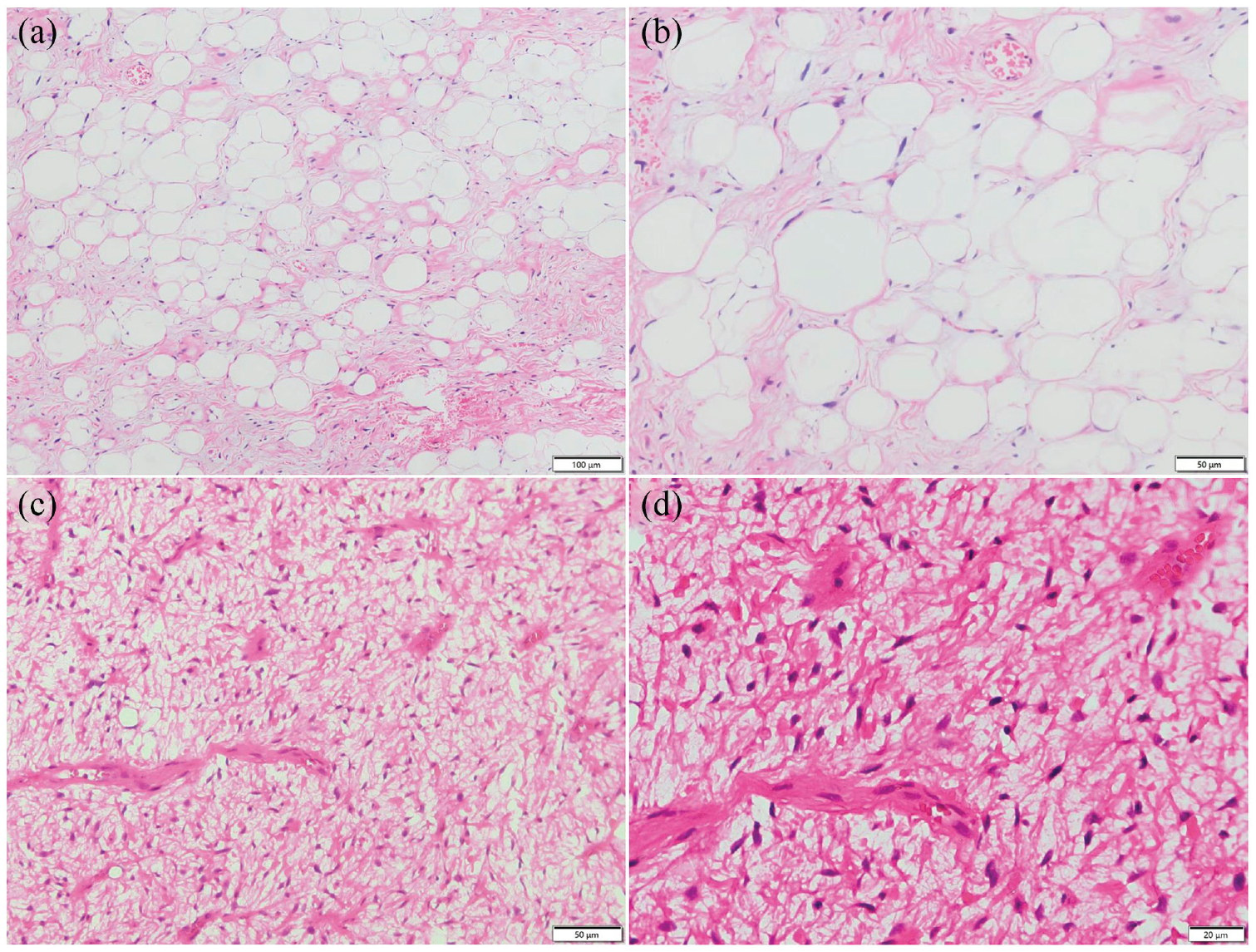
Well-differentiated components were found morphologically. The adipocytes varied in size, and atypical interstitial cells were observed within the fibrous septum. (a) H&E, ×100. (b) H&E, ×200. Dedifferentiated components were found morphologically. Morphology revealed that fibroblast-like cells were predominant with relatively low density and myxoid degeneration of the interstitium was observed with plexiform microvascular structure. A few fat vacuoles were present focally; nuclear atypia is mild to moderate; mitotic figures were less than 5/10 HPF; and necrosis was rare. (c) H&E, ×200. (d) H&E, ×400.

IHC and FISH findings of the tumor. Positive immunoreactions for CDK4 (a), MDM2 (b), Ki-67 (c), P16 (d), and S-100 (e) in the nuclei of tumor cells, in addition, (f) FISH analysis identified MDM2 amplification, confirming the diagnosis of DDL.
Discussion
Of the 95 cases of PMLs, 36 occurred in the anterior mediastinum, 19 in the posterior mediastinum, 4 in the middle mediastinum, and the others were unstated. In addition, 55 cases occurred in men, and 40 cases occurred in women. The mean age of the patients was 52.6±17.4 years. The youngest patient was 3 years 4 and the oldest was 82 years. 5 Tumors reported in these studies ranged in size from 2.2 to 61 cm in the greatest dimension. 4 Histologic examination revealed 35 cases of well-differentiated liposarcoma (WDL), 21 cases of DDL, 21 cases of myxoid liposarcoma, 6 cases of pleomorphic liposarcoma (PL), 1 case of myxoid pleomorphic liposarcoma, and 11 cases of unstated type, as detailed in the Supplemental Table. PMLs develop most commonly in the posterior mediastinum in approximately 48% of cases, followed by 28% in the anterior mediastinum and 11% in the middle mediastinum. 6 The DDL we report in this study occurred in the posterior mediastinum. The radiologic features of mediastinal liposarcomas are nonspecific but are suggestive of the diagnosis. On CT, the appearance of mediastinal liposarcomas varies from a predominantly fat-containing mass to a solid mass, like liposarcomas located at other sites in the body. 7 Low attenuation values between −50 and −150 Hounsfield units are consistent with that of a tissue composed of fat. 8 In this case, the mass was heterogeneous in density, with variable proportions of fat, soft tissue, and myxoid tissue, with Hounsfield unit values ranging from −22 to −109.
The histological type of liposarcoma influences the prognosis of the tumor. Dedifferentiated types are regarded as highly malignant tumors with a tendency toward local recurrence and metastasis. 9 Currently, DDL is thought to respond poorly to chemotherapy and radiotherapy. Ifosfamide and doxorubicin are the most common chemotherapy agents for the treatment of mediastinal liposarcoma. However, adjuvant therapy for mediastinal liposarcoma remains controversial.9,10 Therefore, the best treatment for DDL appears to be complete surgical excision. 11 Previous case reports or research on primary mediastinal DDL have shown that complete surgical excision was performed in almost all patients.4,11–14 As mentioned above, a total of 41 literature reported 95 cases of PMLs, Of them, histologic examination confirmed 21 cases of DDL, but only 3 cases of DDL in the posterior mediastinum had been reported, and as follows: Kentaro Miura et al. 12 reported a 75-year-old man, who did not exhibit any symptoms, but chest CT showed a huge tumor (20 cm in diameter) in the posterior mediastinum, which projected on either side of the intrathoracic space, surgical resection was performed, pathology revealed DDL, and there was no recurrence at 3 months. Hejin P. Hahn et al. 4 reported a 65-year-old man, whose chest CT showed a 17 cm huge tumor in the posterior mediastinum. The tumor was removed by surgery, and the pathology revealed DDL, the recurrence was found 23 months after the postoperative follow-up, and the patient was still alive 30 months after the follow-up. Bema Coulibaly et al. 15 reported a 34-year-old woman who complained of increasing dyspnea; imaging features revealed a bulky posterior mediastinal mass, a gross total resection was performed by thoracotomy, the tumor weighed 1029 g and measured 20 cm, histological examination showed a DDL, MDM2, and CDK4 were positive by IHC, and FISH analysis showed amplification of MDM2 and CDK4 genes in 12q14–15 region, the patient recurred after 15 months, which was completely resected again, but recurred after 8 years and died. The case we reported was a 63-year-old woman who complained of cough, sputum, and pain in the right chest wall. Chest CT revealed a giant mass of 24×15×24 cm in the posterior mediastinum of the right thoracic cavity. Resection was performed, and histological examination revealed a DDL, MDM2, and CDK4 were positive by IHC, and FISH analysis showed amplification of MDM2. Compared with the first two cases above, there were some similarities. For example, the patients were all elderly, and the tumor size of the patients was also large, which could achieve a better therapeutic effect through surgical resection (although the follow-up time of the first case was only 3 months). In the third case, a young woman whose tumor was almost the same size as the one we reported, and the results of the auxiliary tests were the same. However, she recurred after 15 months of follow-up.
Patients with DDL or PL have significantly worse survival and prognosis than patients with myxoid or WDL. Compared with WDL, DDL at all sites had significant rates of metastasis (17%) and disease-related mortality (28%). 16 In our case report, no metastasis or recurrence was observed in this elderly patient during 19 months of follow-up after surgical excision; however, long-term, careful follow-up is still strongly needed.
Conclusion
In conclusion, mediastinal liposarcoma is a rare malignant tumor, based on the clinical practice of this case and previous literature, the best treatment is complete surgical removal. As with most sarcomas, the risk of recurrence is related to the completeness of the resection. Nonetheless, a long-term follow-up will be required for this patient.
Supplemental Material
sj-docx-1-hpq-10.1177_2050313X231206031 – Supplemental material for Giant primary liposarcoma of the mediastinum: A case report and review of the literature
Supplemental material, sj-docx-1-hpq-10.1177_2050313X231206031 for Giant primary liposarcoma of the mediastinum: A case report and review of the literature by Jingjing Rao, Qingling Zhu and Xuejiao Yang in SAGE Open Medical Case Reports
Footnotes
Acknowledgements
We would like to acknowledge all members of the Department of Thoracic Surgery, Taihe Hospital, Hubei University of Medicine.
Author’s contribution
Xuejiao Yang conceived the study. Jingjing Rao and Qingling Zhu drafted the manuscript. Jingjing Rao and Xuejiao Yang collected pathological and surgical data from patients. Qingling Zhu assisted with updating the patient follow-up information and the literature search. Xuejiao Yang and Qingling Zhu confirmed the authenticity of all the raw data. All authors read and approved the final version of the manuscript.
Availability of data and materials
The data generated in the present study are not publicly available (due to compelling reasons why data are not public) but may be requested from the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Study on clinical application of neonatal thalassemia detection in Shiyan city(22Y98).
Ethics approval and consent to participate
This study has been approved by the ethics committee of Shiyan Maternal and Child Health Hospital (the ethics approval number, 2022KS027), and performed in accordance with the principles of Good Clinical Practice following the Tri-Council guidelines. Written informed consent was obtained from the patient for anonymized information to be published in this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.